Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Review Article - (2016) Volume 5, Issue 3
Background: The burden of mental disorders is increaasing in low and middle income countries including Ethiopia but the number of psychiatry professionals is scarce. Integrating mental health in primary health care is vital to address the problem. This survey aimed in assessing the experiences, strengths and challenges of integrating mental health in primary health care in Ethiopia.
Methods: Facility based supervisions was done in primary health care centers where the scale up program was implemented and giving mental health services. Semi structured and standardized WHO mental health Global Action Programme support and supervision questionnaires was used to collect information's.
Findings: A total of 1576 mental, neurological and substance use (MNS) disorders were identified and treated in selected four regions. Majority of identified cases were epilepsy (46.64%) followed by psychosis (28.49%). Essential drugs for treating psychosis, depression and epilepsy were available in almost all health institutions. Delayed support and supervisions, staff turnover, interrupted supply of drugs and shortage of budget were the major identified challenges of integrations.
Conclusions: In general the experiences of mental health integration in Ethiopia have shown promising findings in achievements in number of trained professionals, health care centers involved, availability of drugs and cases identified and treated by trained professionals. Increasing number of staff trained in mental health care and Continuous support and training for trained professionals, supply of psychotropic medication is vital for effectiveness of integration. In additions researches in scale up concentrating on impact and outcomes of interventions are implicated for understanding the success of interventions.
<Keywords: Mental health, Premature mortality, Health care programs
Today, mental disorders are recognized as a public health problem in developed as well as developing countries. They now account for about 14% of the global burden of disease mostly chronically disabling illness, depression and other common mental disorders such as psychosis [1,2] and this will rise to 15% by the year 2020. For disability alone, without the effects of premature mortality, the impact of neuropsychiatric conditions is starker still: they account for 31% of all years lived with disability. The stigma and violations of human rights directed towards people with these disorders compounds the problem [3].
In low income countries, such as Ethiopia mental disorders which are not considered as not life threatening problems are not given attention for long time [4,5] As a result mental health services are not given due priority and the needs of people for mental health care are not meet [6,7]. In Ethiopia, only 10% of people with severe forms of mental disorders ever receive effective care [4]. Untreated mental disorders leads disability, create a substantial personal burden for affected individuals and their families, poor quality of life, human rights abuses, stigma and discrimination, poverty, decrease productivity, suffering, poor physical health and premature mortality [8-12].
In addition to increasing burden of mental disorders in low to middle income countries (LMICs), which are often co-morbid with physical diseases, there is a scarcity of mental health specialists [3,12], In order to address the problems and support huge neglect of people with mental disorders World Health Organization (WHO) launched the mental health gap action programme (mhGAP) for scaling up of mental health care through integration into primary health care (PHC) and general medical services [3]. The main aim of the programme is treating common mental, neurological and substance use (MNS) at PHC level( non specialized setting) by trained non specialized professionals [13-15].
Due to burden of mental disorders, available treatment gap and high co-occurrence of physical and mental disorders in addition to increase access, reduction in stigma and affordable and low cost, integration of mental health in primary health care is essential and un debatable. In order to overcome problems of low coverage of mental health service in Ethiopia ministry of health is implemented integrated treatment of mental disorders in primary health care (PHC) based on WHO mental health scale up programme [3]. This paper aimed in assessing the experiences, strengths and challenges of the integration.
Ethiopia has been implementing Health Sector Development Programme (HSDP) since 1997.
Currently the country launched phase five HSDP having four tier structures [16,17]. This health care structure is found to be very suitable for easy success and achievements of integrating mental health in primary health care.
Tier 1
The Primary Health Care Unit. A health center will provide for 25,000 people and is fed by five health posts, each responsible for 5,000 people. Every health center is to be staffed by a health officer, a clinical nurse, a community nurse, an environmental sanitarian and a laboratory technician.
Tier 2
The District Hospital. To be fed by ten health centers covering a population of 250,000. Staffed by four GPs and a health officer, together with clinical and community nurses, a pharmacist and a laboratory technician. It will carry out routine curative and referral care and oversee the community health work of the population. There will be only limited cold surgery as the emphasis will be on life saving surgery with appropriate training provided for GPs.
Tier 3
The Regional Hospital. Staffed by six or more specialists and serving a population of one million, it will be responsible for the referral work from district hospitals and will be the focus of training and development.
Tier 4
Specialist Hospitals. These comprise of regional hospitals with specialist units serving 5 million people.
Ethiopia is a typical case of a developing nation, The country is with a population of over 96 million, has less than 100 psychiatrists, around 150 MSC trained mental health professionals, about 200 BSc psychiatry nurses and more than 300 diploma psychiatry nurses.
With this mental health professionals it is difficult to address the mental health care needs of the country (Table 1). So integrating mental health to primary health care is necessary and vital to address the needs of the community.
| No. | Professional | Frequency |
|---|---|---|
| 1 | Psychiatrist | 63 |
| 2 | MSC mental health professionals | 150 |
| 3 | BSc psychiatry nurses | 200 |
| 4 | Diploma psychiatry nurses(trained) | 446 |
| 5 | mhGAP trained health professionals | 360 |
Table 1: Health Professionals involved in mental health care in Ethiopia, April, 2016.
In Ethiopia mental disorders which are considered as not lifethreatening are not given attention for long time. There is only one mental health hospital (Amanuel Mental Specialized Hospital) giving services for mental health for long time. In order to address mental health care needs of the country the Ethiopian government is practicing community based mental health services including integration of mental health service at primary health care (PHC) level.
Integrating mental health service in primary health care (Mental Health Gap Action Program (mhGAP) for people suffering from mental, neurological, and substance use disorders) in Ethiopia
After successful three years pilot program (2010-2013) of Mental Health Gap Action Program (mhGAP) for people suffering from mental, neurological, and substance use disorders in different regions of Ethiopia, federal ministry of health (FMOH) decided implementation mhGAP Scaling up care for mental, neurological, and substance use disorders in Ethiopia in 2013 and was started to be implemented before one year and six month in different regions of Ethiopia (2014). The purpose of mhGAP programme is implementation and Scaling up care for mental, neurological, and substance use disorders in primary health care facilities(nonspecialized health-care settings) by non-specialized professionals (working at first- and second-level facilities).
The scale up was planned to be undertaken in phases. Scale up - phase one (2014-2016) was to planned to train 1266 professionals from 633 health facilities. For 2014 plan was to train 200 health professionals from 100 heath facilities. For phase one scale up around 360 primary health care professionals selected from different health care facilities were trained on selected mhGAP priority disorders (Table 2).
| Number | Region/administrations | Number of participants | Numberofhealth institutions |
|---|---|---|---|
| 1 | Gambella | 8 | 4 |
| 2 | Benshangul | 7 | 4 |
| Gumuz | |||
| 3 | Addis ababa | 80 | 40 |
| 4 | Afar | 16 | 8 |
| 5 | Tigray | 36 | 18 |
| 6 | Amhara | 40 | 20 |
| 7 | South ethiopa | 70 | 35 |
| 8 | Oromia | 76 | 38 |
| 9 | Harari | 12 | 6 |
| Total | 360 | 180 |
Table 2: Number of participants, respective regions and their professions involved for mhgap service scale up training in ethiopia 2014.
The scale up was decided on four WHO mhGAP priority disorders:
• Alcohol use disorders
• Depression
• Psychosis
• Epilepsy
mhGAP support and supervision for trained professionals: One of the major component of mental health integration is continues support, supervision and mentoring. The aim of support and supervision to assist mhGAP trainees to deliver improved mental health care (clinical supervision) and provide support in the work environment related to mhGAP implementation(administrative and programmatic supervision).
Support and supervision is considered as one part of the training and was planned to be undertaken every three month. After training and experience of for average of nine months the professionals were supervised and support once which is below expected standard of support and suppervisions.
mhGAP priority conditions identified by trained professionals: In average of nine months services a total of 1576 cases were identified and treated by trained professionals in selected three regions. The commonly identified disorder was epilepsy followed by psychosis and alcohol use disorders is the least identified disorders among selected priority disorders for scale up (Table 3).
| Disrobers | Addis Ababa city | Somali region | Benishangul region | Total |
|---|---|---|---|---|
| Depression | 128 | 55 | 35 | 218 |
| Psychosis | 89 | 345 | 15 | 449 |
| Epilepsy/Seizures | 307 | 230 | 198 | 735 |
| Alcohol Use Disorders | 20 | - | - | 20 |
| Bipolar Disorder | 12 | 37 | 1 | 50 |
| Developmental Disorders | 9 | - | - | 9 |
| Dementia | 2 | 5 | 7 | |
| Drug use disorders | 1 | 9 | 10 | |
| Behavioral Disorders | 12 | - | 12 | |
| Self-harm/Suicide | 30 | 20 | 5 | 55 |
| Other MNS condition | 11 | - | 11 | |
| All | 621 | 701 | 254 | 1576 |
Table 3: Conditions identified by trained provider in selected three regions from December 2014 to August 2015.
Percentage distribution of Conditions identified by trained provider in selected three regions from December 2014 to August 2015: Epilepsy was disorders with com monly identified in all regions 46.4% from the total cases followed by psychosis 28.49 percent (Figure 1).
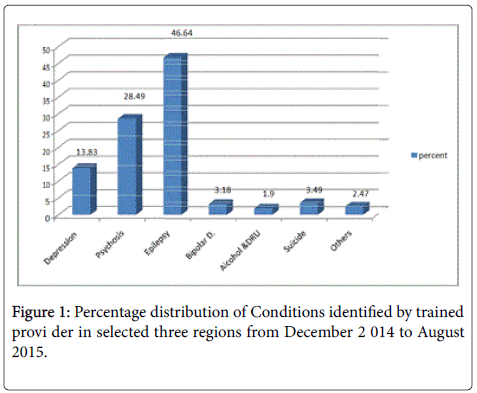
Figure 1: Percentage distribution of Conditions identified by trained provi der in selected three regions from December 2 014 to August 2015.
Psychotropic medications available at primary health care level in Ethiopia
In majority of primary health care facilities common drugs for treating depression, psychosis, and epilepsy were available (Table 4).
| Type of psychotropic drugs | Available groups |
|---|---|
| Antidepressants | Fluexetine, amitriptiline |
| Antipsychotics | Chlorpromazine, haloperidol, respirodone |
| Anticonvulsants | Phenobarbitone , phenytoine, sodium Valporate, carbamazepine |
| Mood stabilizers | Sodium valporate, carbamazepine |
| Anxiolytics | Diazepam, clonazepam |
Table 4: Psychotropic drugs available at primary health care levels in selected three regions of Ethiopia from December 2014 to August 2015.
• Government leadership and political commitment
• Necessary policies and strategies in place including Multifaceted, system wide approach incorporating health extension workers, referral network, infrastructures as well as support and supervision for health workers
• Number of health institutions planned to give the service (more than 90% achieved)
• Number of professionals planned to be trained (more than 90% achieved)
• Availability of drugs used for treating mental disorders in good number of the health centers/hospitals
• Strong and well developed health care delivery system
• Staff turnover
• Lack of attentions, awareness and understanding of the program by regional health bureaus
• Inadequate promotion and follow-up of the mhGAP scale up by the stake holders
• Delayed and inadequate supportive supervisions for trainees
• Shortage of budget for supportive supervision and mentoring
• Interrupted supply of drugs
• Inadequate demand for the service
• In general the experiences of mental health integration in Ethiopia have shown promising findings in achievements in number of trained professionals, health care centers involved, availability of drugs and cases identified and treated by trained professionals.
• Increasing number of PHC staff trained in mental health care and Continuous supply of psychotropic medication is vital for effectiveness of integration.
• Continuous support and training for trained professionals is necessary for sustainability of the program.
• Creating awareness to the necessary stake holders is vital.
• Integration of mental health into primary care is necessary and practicable with challenges.
• A collaborative effort and the use of existing community-based structures are necessary for effective mental health service delivery at the grassroots.
• Future researches in scale up concentrating on impact and outcomes of interventions are implicated for understanding the success of interventions.
The authors acknowledge World Health Organization(WHO) and federal ministry of health of Ethiopia for funding pilot mhGAP program, mhGAP training and supportive supervisions.
The authors appreciate the respective institutions and the trained professionals for their cooperation in providing the necessary information.