Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2012) Volume 2, Issue 1
Keywords: Treatment; Heart failure; Guidelines; Romania
Optimal therapy in CHF patients was subject of many studies that reported decreased awareness regarding of the severity of this disorder and the underuse of evidence based treatment [1-7]. Literature data suggest yet a trend of improvement in adherence to the treatment recommended by guidelines over time, due to both implementation of educational programmes and also increased awareness of the medical staff. Guidelines adherence was demonstrated to occur also spontaneously, in the absence of any specialized intervention [8].
CHF diagnosis, management and treatment are made based on evidence obtained from clinical, cohort, epidemiological or observational studies as well as physicians’ clinical experience. Treatment guidelines of the European Society of Cardiology summarize relevant evidence regarding risks and benefits of certain therapeutic interventions, and are meant to support physicians of any specialty in decision making regarding the management of this condition [9,10].
In 2008, the European Society of Cardiology published the Guidelines for the diagnosis and treatment of acute and chronic cardiac failure, a review of previous guidelines published in 2005.
Both guidelines underline the importance of implementing the guidelines in the clinical practice in order to increase survival, improve morbidity and quality of life. The physicians adherence to treatment guidelines as well as the patients compliance are compulsory [9,11].
Within this context, this study proposes to investigate cardiologists adherence to the Guidelines for diagnosis and treatment of heart failure issued by the European Society of Cardiology in patients admitted to the Cardiology Department of the Rehabilitation Hospital of Cluj-Napoca, Romania, and analyze dynamics changes in guidelines implementation in the clinical practice between 2006 (ESC Guidelines 2005) and 2009 (ESC Guidelines 2008), analyzing by comparison the results obtained in the two years. It is expected to notice that the natural course of the guidelines implementation over the past few years was followed, since no special awareness measures, such as programmes for increasing medical staff awareness, or programmes designed to improve patients compliance and consequently improving quality of life were applied within this time frame.
This study was retrospective, observational. Two cohorts were investigated. The first cohort included 415 patients - 179 females (representing 43.1% of the patients), 236 men (representing 56.9% of the patients), aged between 32-92 years, mean age of 67.07±10.59, who were admitted with a diagnosis of chronic heart failure (CHF), NYHA class II-IV, to the Cardiology Department of the Rehabilitation Hospital of Cluj-Napoca, over a year, between January 2006 and December 2006.
The second cohort comprised 500 patients, 274 men (representing 54.8%) and 226 women (representing 45.2% of the patients), between 27 and 94 years of age, mean age 67.31±11.27, admitted with a diagnosis chronic heart failure (CHF) NYHA functional class II-IV to the same hospital, over one year- January 2009 to December 2009.
Data were gathered from patients’ charts and discharge recommendations/ medication list. In all patients, the drug treatment prescribed during admission and upon discharge was followed and compared with the recommendations made by the ESC Guidelines for diagnosis and treatment of CHF published in 2005 and 2008 respectively. Additionally, treatment and guidelines adherence were compared between the two years – 2006 and 2009.
Statistical analysis was performed by using SPSS 16.0 for Windows, Medcalc 10.3.0.0. The χ2 test was used in the analysis of differences between qualitative variables. Normal distribution of continuous numerical variables was checked by the Kolmogorov-Smirnov test. Differences among continuous qualitative variables were assessed with the aid of Student’s t-test (unpaired and paired), while for distribution variables noncomplying with the normal condition, non-parametric tests (Mann-Whitney U) were used. The logistic regression was applied to identify independent prediction factors. A value of p<0.05 was deemed statistically significant.
The comparative features of the patients for the two years are showed in Table 1.
| Features | 2006 | 2009 | p |
| PATIENTS’ NUMBER | 415 | 500 | |
| MEAN AGE | 67.08±10.59 | 67.31±11.27 | NS |
| Mean age females | 67.71±10.42 | 69.91±9.96 | p<0.05 |
| Mean age men | 66.6±10.72 | 65.17±11.85 | NS |
| MEAN EF (%) | 56.09±14.83 | 58.91±15.41 | NS |
| Mean EF females (%) | 60.49±13.41 | 64.42±13.79 | p<0.05 |
| EF men (%) | 52.75±15.02 | 54.37±15.23 | NS |
| NYHA Class II | 43 (10.4%) | 37 (7.4%) | NS |
| NYHA Class III | 293 (70.6%) | 359 (71.8%) | NS |
| NYHA Class IV | 79 (19%) | 104 (20.8%) | NS |
| HTA | 235(56.6%) | 289(57.8%) | NS |
| DIABETES | 116 (27.9%) | 155 (31%) | NS |
| ATRIAL FIBRILLATION | 209 (50.4%) | 239 (47.8%) | NS |
| VENTRICULAR ARRITHMYAS | 72 (17.39 %) | 99 (19.8%). | NS |
| PULMONARY DISEASES (COPD, ASTHMA, CHRONIC BRONCHITIS) |
69(16.6%) | 44 (8.8%) | p<0.05 |
| RENAL FUNCTION | |||
| Median creatinine value | 1.04 | 1.09 | NS |
| Median urea value | 45 | 51 | NS |
Table 1: Comparative features of patients for the two years.
Renin angiotensin inhibitors were prescribed to the majority of patients, the percentage being 74.4% in 2006 and 77.20% in 2009, respectively. There was registered a significant decrease in ACEI use (71.3% vs 65.2%; p<0.01) along with a very important (fourfold) increase of ARBs use (3.1% vs 12.20 % p<0.01). Beta-blockers prescription increased from 51.8% in 2006 to 69.2 % in 2009. Even in patients with a concomitant diagnosis of COPD, the use of betablockers increased from 28.6% to 34.10 %, p<0.05. The use of loop diuretics slightly decreased in 2009 (89.4 % vs 85% %; p>0.05), as well as the use of aldosterone antagonists (80.2% vs 67.8%; p<0.05). Digoxin was less prescribed in 2009 (57.10% vs 42.60%) even if the percentage of patients carrying a diagnosis of atrial fibrillation was approximately the same, of almost 50 %. The use of antiplatelet drugs increased in 2009. The comparison between the treatments recommended in the two years is summarized in Figure 1.
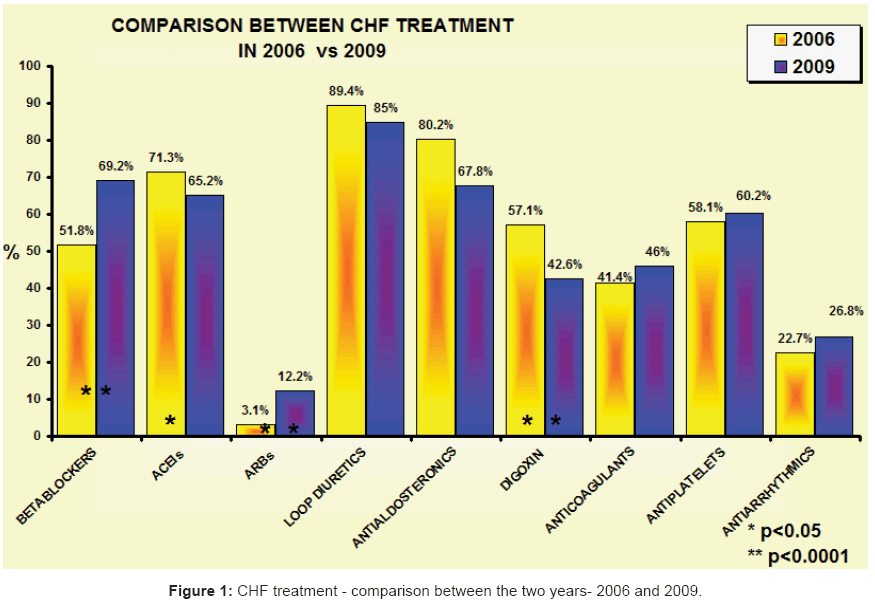
Figure 1: CHF treatment - comparison between the two years- 2006 and 2009.
From certain points of view, the CHF treatment in women improved in 2009 in comparison to 2006. Beta-blockers and ARBs were administered in more frequently- p<0.05. The prescription rate of loop diuretics decreased - p<0.05, along with the use of digoxin and aldosterone antagonists, p<0.01. There was no difference regarding the use of ACEIs and antiplatelet medication.
Men were also more frequently prescribed beta-blockers and ARBs – p<0.01, yet they received significantly less ACEIs, digoxin- p<0.01 and aldosterone antagonists p<0.05. No differences were registered in the prescription of antiplatlets and loop diuretics.
The treatment evolution of CHF patients younger than 64 years was characterised by a significant increase in the prescription of ARBs (3.5% vs 11.1%), beta-blockers (59.7% vs 74.2%), and antiplatelets (45.8% vs 60.1%), p<0.01. Digoxin was less recommended in 2009 (54.9% vs 39.4%), p<0.01. No significant differences were reported regarding the treatment with ACE-inhibitors (66.7% vs 63.1%), loop diuretics (84.7% vs 80.3%), aldosterone antagonists (75.7% vs 68.7%) and antiarrhythmic drugs (27.1% vs 29.8%).
Regarding women under the age of 64, the only statistically significant differences were noticed in the prescription of digoxin, which decreased from 54.2% in 2006 to 35.5% in 2009- p< 0.05, and antiplatelets, which were more frequently recommended in 2009 - 56.5% compared to 32.2% in 2006, p<0.01.
Treatment of male patients included in this age group, improved significantly in 2009. Men were more frequently prescribed ARBs (p<0.01) and beta-blockers and less frequently digoxin - p<0.05.
In 2009, several medications were more frequently administered to the patients between 65-75 years of age, such as ARBs 2.5% vs 11.7% and beta-blockers (49.4% vs 72.4%), p<0.0001. Other medications were less frequently prescribed in this age group in 2009- loop diuretics (91.4% vs 82.8%), digoxin (56.2% vs 41.4%), p<0.01 and aldosterone antagonists (82.1% vs 63.4%), p< 0.0001.
Prescription of beta-blockers in both sexes between 65-74 years of age was reduced in 2009, yet in females, differences were more significant than in men (p=0.003 vs p=0.02). ARBs and nitrates were less frequently recommended in 2009, yet in this case, a statistically significant difference (p=0.02) was registered only in men. Diuretics and aldosterone antagonists were less frequently recommended in females in 2009 (p<0.001), with no changes in men.
In patients over 75 years old, the only significant differences was reported in the administration of beta-blockers (46.9% vs 66.2%) and ARBs (0 % vs 6.2%), in which there was a significant increase in the prescription rates in 2009, p< 0.05.
For 2009, it was noted a higher prescription rate for ARBs (p<0.005) in females over 75 years old and an increased prescription rate for betablockers (p<0.005) in men.
In 2006, digoxin was more frequently used than in 2009, when the prescription rate of beta-blockers and amiodarone increased – Figure 1. In 2009, no patients were treated with propafenone.
In 2009, patients with ventricular arrhythmias and CHF benefited were treated more frequently with beta-blockers (p=0.01) - Figure 1. 2% of the patients received sotalol, compared to 2006, when it was not recommended.
Beta-blockers were also administered more often to patients with pulmonary obstructive diseases in 2009 - 34.10%, compared to 28.6% in 2006, yet they remain underused in this subgroup of patients.
We have analyzed the differences between CHF therapies in these two years, depending on ejection fraction - Figure 2. In 2009, there was an increase of 12.9% in the use of ARB’s, especially in patients with an ejection fraction > 45%. Betablockers have been prescribed more frequently in 2009, especially in patients with a low EF. Spironolactone and digoxin use has decreased, but more significantly in CHF with a preserved EF.
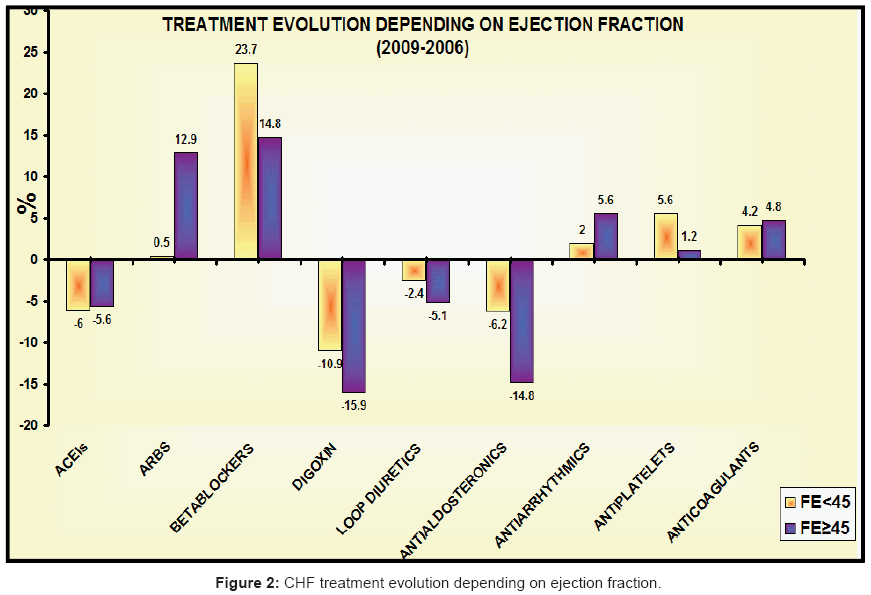
Figure 2: CHF treatment evolution depending on ejection fraction.
19.3% of women with CHF with preserved ejection fraction received ARB’s in 2009, in comparison with 2006 when only 5% of female patients received the same medication (p<0.0001). Aldosterone antagonists, digoxin and diuretics were less recommended in 2009 to women with diastolic heart failure (p<0.0001, p<0.0001 and p<0.05 respectively) - Figure 3. Use of ACEIs decreased in male patients in 2009 (p<0.05), but increased the use of ARB’s. Betablockers were less prescribed in 2006 (p<0.001). Digoxin was also less recommended in men with heart failure with preserved ejection fraction (p<0.01) - Figure 3.
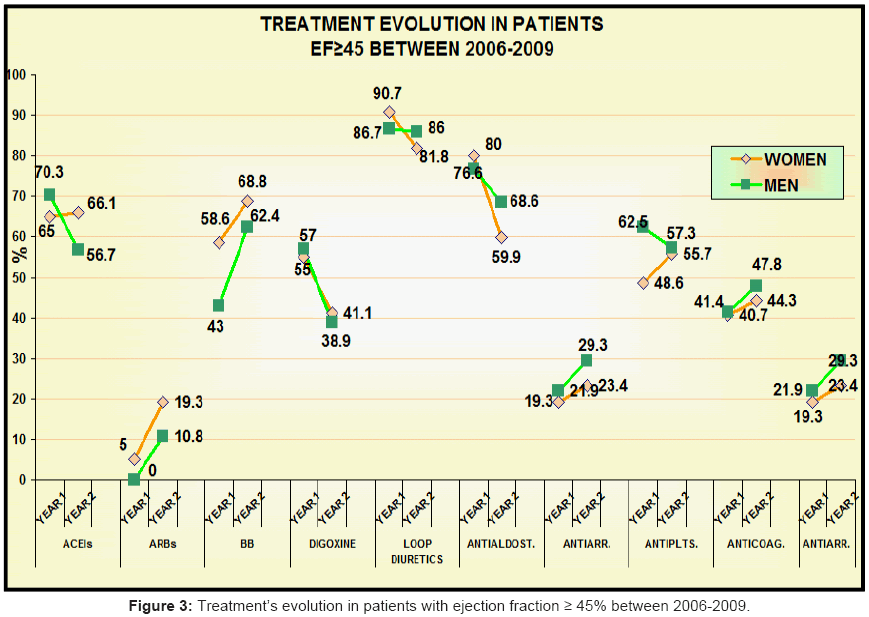
Figure 3: CHF treatment evolution depending on ejection fraction.
As regarding the therapy of patients with low ejection fraction, in men there was a significant increase in the use of betablockers, from 50% in 2006 to 78.6% in 2009 (p<0.0001). In women with systolic heart failure, we found no significant differences regarding the classes of medication that was used- Figure 4.
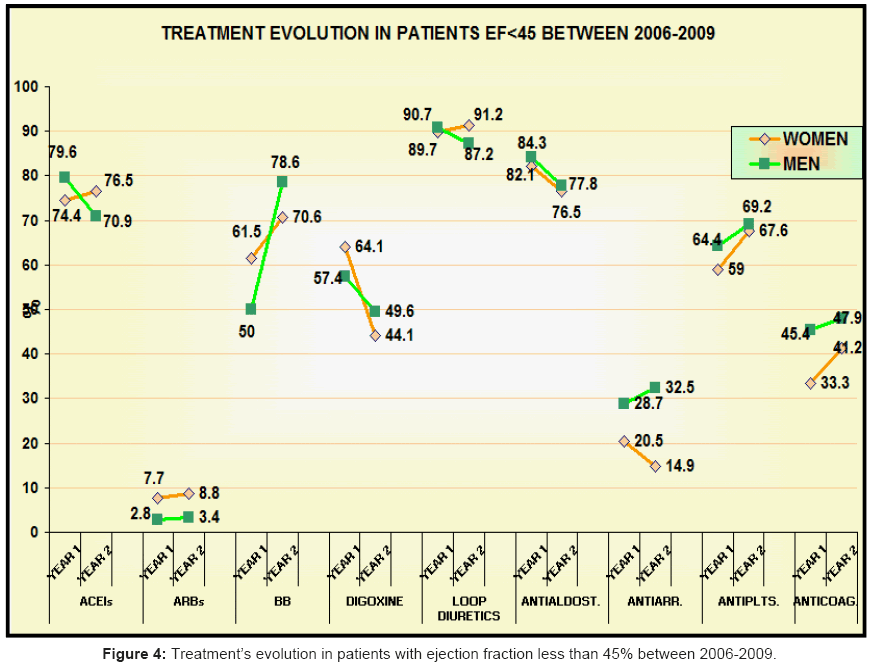
Figure 4: Treatment’s evolution in patients with ejection fraction less than 45% between 2006-2009.
In this study, there were compared the characteristics and the modality of treatment in CHF patients discharged from a General Romanian Hospital in 2009 (after the 2008 ESC guidelines were published) , with those of an analogous patient population observed three years earlier, in 2006 (after the 2006 ESC guidelines were published). It was noted that there were several statistically significant differences between the two years, and overall CHF treatment improved over time.
Beta-blockers are in class of recommendation IA, level of evidence A, in both guidelines- 2005 and 2008 [9,11-14] Studies have confirmed that their use improves morbidity and mortality in CHF patients. In our study, beta-blockers were more commonly used in 2009, irrespective the patients’ sex, CHF etiology or age. Overall the use of beta-blockers increased in 2009, independent of NYHA functional class and CHF type (systolic or diastolic), the most significant differences being obtained in patients NYHA class IV and in those with EF < 45%. Although the administration of selective beta-blockers is no longer contraindicated in patients with COPD [15,16], some physicians take this into account, others do not, hence although beta-blockers were recommended to these patients in higher percentages in 2009 compared to 2006, their prescription rate is still low.
Frankenstein and colleagues monitored the evolution treatment adherence to guidelines between 1994-2000 and 2001-2007 and have established that the use level of ACE inhibitors and ARBs decreased, being though associated with an increase in beta-blockers and aldosterone antagonists prescription [8]. In our study, ARBs were much more frequently administered in 2009, especially in patients with preserved ejection fraction and hypertension. In the 2008 guidelines ARBs have a class of recommendation and level of evidence IA, in comparison to the 2005 guidelines-class of recommendation and level of evidence IB, being recommended in all patients with CHF and low ejection fraction, symptomatic already treated with beta-blockers and ACEIs, unless they are treated with aldosterone antagonists [9,11]. However, concurrent administration of the three RAAS inhibitors - ACEI, ARBs and aldosterone antagonists is not encouraged [11]. Thus, guidelines recommend that aldosterone antagonists should be administered especially in patients with low EF, NYHA functional classes III-IV [11]. Recent studies (ALDO-HF- Aldosterone Receptor Blockade in Diastolic Heart Failure and TOP-CAT- Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist) suggest that spironolactone and eplerenone could also be used in patients with less severe congestive syndrome, NYHA classes II-III, as it is well known that they have anti-fibrotic effect, improving cardiac remodelling in CHF [17]. In our study, administration of aldosterone antagonists was reduced in 2009 compared to 2006.
The 2005 and also the 2008 ESC guidelines recommended loop diuretics for improving dyspnea – class of recommendation Ia, level of evidence A, for improving the congestive syndrome in patients with moderate-severe CHF [9,11]. The level of recommendation of loop diuretics also decreased in 2009, but the difference was not statistically significant.
Digoxin recommendation changed also from class of recommendation IIa, level of evidence A in 2005 to class of recommendation IIa, level of evidence B in 2008. [9,11]. In our study, digoxin was often recommended, especially in 2006, when its level of prescription exceeded that of beta-blockers. The percentage of patients who were recommended digoxin was though lower in 2009. Increased administration of digoxin may be explained by the fact that atrial fibrillation was commonly present in our patients. Other studies report an AFib percentage of approximately 25-30% [19-21]. More than two thirds of the patients taking digoxin were diagnosed with atrial fibrillation, yet, more than half of the patients in sinus rhythm that were also treated with digoxin, had an EF ≥ 45%, which does not justify this treatment.
The rate of prescription for antiplatlets did not significantly change overall, except in women younger than 64 years of age, in whom their use increased in 2009. In addition atiplatelet agents other than aspirin, such as clopidogrel, dipyridamole and triflusal were used. It is well known than in CHF patients, thromboembolic complications and stroke are relatively common, regardless of atrial fibrillation presence. In this context, the chronic administration of antiplatelets leads to reduced morbidity and mortality and improved quality of life in CHF patients [22].
The treatment of both females and the elderly improved in 2009 in comparison to 2006, having a similar course to the global treatment, with increased in ARBs and beta-blockers and decrease in diuretics, aldosterone antagonists and cardiotonics prescription. These data are not concordant to those reported by Frankenstein and collaborators in 2010, who argue that the female sex and advanced age associate with poor adherence to guidelines [8].
When compared to men, females seem to be protected by ischemia, most likely due to hormonal differences between the two sexes [23]. The mean ejection fraction of the patients included in the study was over 45%, especially in the females, who were more frequently diagnosed with heart failure with preserved ejection fraction. Most of the trials performed, investigating the efficiency of various drug therapies in CHF patients included mainly patients with systolic CHF [24]. In our study, in 2009, the percentage of females with preserved ejection fraction was higher than in 2006, which could be explained by the larger number of females over 75 years of age considered in the study, being common knowledge that females and advanced age are characterized by diastolic CHF [25,26].
Furthermore, we revised recommendations for ventricular resynchronization therapy. Ventricular resynchronization devices are currently recommended to symptomatic patients, with EF <35%, whereas in 2005, they were recommended to patients with an EF<30- 35% and are demonstrated to improve survival and reduce morbidity [8,11]. The recommendation class and level of evidence remained unchanged - IA [8,11]. No recommendations are made for patients with low EF, yet asymptomatic. In the Cardiology Department of the Rehabilitation Hospital of Cluj-Napoca, the resynchronization therapy was not used in 2006 in any patient, while in 2009 only one patient was underwent resynchronization therapy, which was done in another medical center. Two defibrillators were implanted in 2009 and another three in the beginning of 2010. The major issue is yet the lack of subsidized devices, their costs being prohibitive; hence the majority of patients cannot afford them. The study published by Merkley and colleagues in 2010 in Europace analyzed resynchronization therapy recommendation in several European countries between 2006 and 2008. In Romania it has been reported rate of CRT devices implantation of approximately 9.9 devices/year [27].
Our study was different than other types of trials like for instance IMPACT-RECO, which used educational activities meant to increase guidelines adherence [28]. It has been demonstrated that, to a certain extent, improvement of CHF management is made spontaneously, even in the absence of specialized programmes. It cannot be totally excluded the role of multiple studies published after the 2005 ESC issue of the Guidelines for the diagnosis and treatment of CHF, which have confirmed the underuse of recommended medication to these patients.
The adherence to guidelines improved during a three- year period in Romania. Renin-angiotensin inhibitors, beta-blockers and diuretics are used according to the guidelines recommendations, however antiplatelet drugs remain underused. Gender and age did not significantly influence treatment.