Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2013) Volume 1, Issue 2
Background: Nasal extranodal natural killer (NK)/T-cell lymphoma are highly aggressive diseases with a poor outcome. Several studies have shown the interest of L-asparaginase in salvage therapy and first-line L-asparaginase combination therapy for advanced stage extranodal NK/T-cell lymphoma should be tested in prospective trials. We report the first experience of treatment with L-asparaginase in salvage therapy and front-line based- regimen in localized nasal NK/T-cell lymphoma.
Patients and methods: We reviewed 13 consecutive localized stages I/II nasal NK/T cell lymphomas, treated in our institution over a 6 years period. 8 patients were treated with CHOP (cyclophosphamide, doxorubicin, oncovin and prednisone) regimen in first-line chemotherapy and with L-asparaginase-based regimen in salvage therapy. Five patients were treated with first-line chemotherapy, including L-asparaginase-based treatment. We report our results in a single retrospective study of these patients with localized stage NK/T-cell lymphoma.
Results: The overall response was 70% and the OS was 54% at 52 months. Conclusion: These data confirm the efficacy of L-asparaginase-containing regimens in extranodal nasal NK/Tcell lymphoma.
Keywords: L-asparaginase; NK/T-cell lymphoma; Nasal type; Localized stage
Extranodal NK/T cell lymphoma, a nasal type lymphoma, is a distinct entity by the WHO classification of lymphomas [1], with a frequency of less than 1% of all non Hodgkin lymphoma (NHL) in the West [2] and in the North of Africa [3] and an increased incidence in Asia [4]. NK/T-cell lymphoma characterized by a CD3e phenotype, with no surface CD3 or T-cell receptor expression, an activated cytotoxic profile with perforin, granzyme B expression, and common expression of CD56 [5-7]. There is no consensual treatment. In stage I/II nasal extranodal NK/T-cell lymphoma, radiotherapy alone is initially effective but final outcome is unsatisfactory because of frequent systemic progression or relapse [8-13].
In contrast, patients who have extensive disease or who relapse after radiotherapy have a very poor outcome [14].
From January 2006 to December 2012, 13 patients with localized stage primary extranodal NK/T-cell lymphoma nasal type, were diagnosed at the Institution University Hospital, 1st November 1954, Oran, Algeria. Eight patients were treated with anthracycline-based regimens (CHOP) in first-line and 6 of them were treated with L-asparaginase-based chemotherapy salvage therapy. Five patients were treated with L-asparaginase front-line therapy and were analyzed in this study.
All patients were informed of the nature and possible adverse reactions of these protocols.
The patients would be included, if they met the following criteria: diagnosis of NK/T-cell lymphoma on primary biopsy of the nasopharyngeal region with a panel of monoclonal antibodies (CD3c, CD20, CD4, CD8, CD56, TIA-1, CD30, LMP-1) CD3e+, CD202 phenotype and markers of EBV (Epstein Bar Virus). Staging consisted of a complete history taking and physical examination, routine blood tests and serum chemistry before treatment. Computed tomography (CT) of the head, neck, thorax, and abdomen was always used to determine the extent of the primary lesion. All patients received protocols with L-asparaginase 6000 U/m2 (Kidrolase-, OPI,Lyon, France) either i.v. on days 2, 4, 6, and 8 combined with methotrexate 3 g/m2 on day 1 before the first asparaginase infusion at each cycle, with folinic acid rescue and dexamethasone 40 mg for 4 days, at the beginning of each cycle. All patients received consolidation radiotherapy (30 Gy) after completion with asparaginase therapy.
Asparaginase toxicity was monitored by complete blood cell count, coagulation tests, antithrombine, amylase, glycemia, bilirubin, aspartate aminotransferase, and alanine aminotransferase measurements.
Response criteri
The treatment responses were assessed using adapted Cheson’s standard criteria [15].
Complete response (CR) was defined as no evidence of residual disease; a partial response as at least a 50% reduction in tumor burden compared with the beginning of treatment; and no response as less than a 50% reduction in tumor burden or disease progression. Responses were assessed from clinical, radiological and laboratory studies prescribed by the individual clinicians.
Baseline characteristics
The characteristics of the patients are shown in table 1. Median age was 42 years (range 21-63 years). 7 patients were female and 6 were males. At diagnosis, the nasal cavity was involved in all patients and systemic B symptoms were present in nine patients. Patients were staged according to the Ann Arbor classification and all were in stage I-II. The median of follow-up was 14 months (5-52 months). According to the IPI classification, 4 patients were IPI=0, 3 patients with IPI=1 and 6 patients with IPI=2.
| Number of Patients (n) | |
|---|---|
| Total | 13 |
| International Pronostic Index (IPI): 0 1 2 |
4 3 6 |
| Staging Stage I and II Stage A Stage B |
13 4 9 |
Table 1: Patients’ characteristics.
Patient outcomes
Among the 8 patients who treated with CHOP regimen, two of them achieved complete remission (CR) and six patients were refractory to their first treatment (CHOP) (Table 2). 2 (25%) of them had CR after the asparaginase-based regimen. In this group, the overall survival (OS) was 37.5% at 52 months and the median of OS was 10 months (4.5-15.5 months. Five patients received the Asparaginase-containing regimen as first-line treatment and 4 of them (80%) achieved CR (Table 2). The OS was 80% at 30 months and the median of OS was not reached (Figure 1). In all patients, the overall response (CR+PR) was 70% and the OS was 54% at 52 months.
| Protocole | CR | PR | Progression | Alive/died | OS |
|---|---|---|---|---|---|
| CHOP (n=8) | 2 | 0 | 6 | 8/0 | - |
| CH CHOP/Aspa(n=6) | 2 | 1 | 3 | 3/3 | 38% at 52 months |
| Aspa (n=5) | 4 | 0 | 1 | 5/0 | 80% at 30 months |
| Total (n=13) | 8 | 1 | 4 | 10/3 | 54% at 52 months |
Table 2: Outcomes according the treatment with CHOP, CHOP/Aspa and Aspa.
The responses were usually very rapid and rapid responses were also seen after only one course of asparaginase-containing regimen.
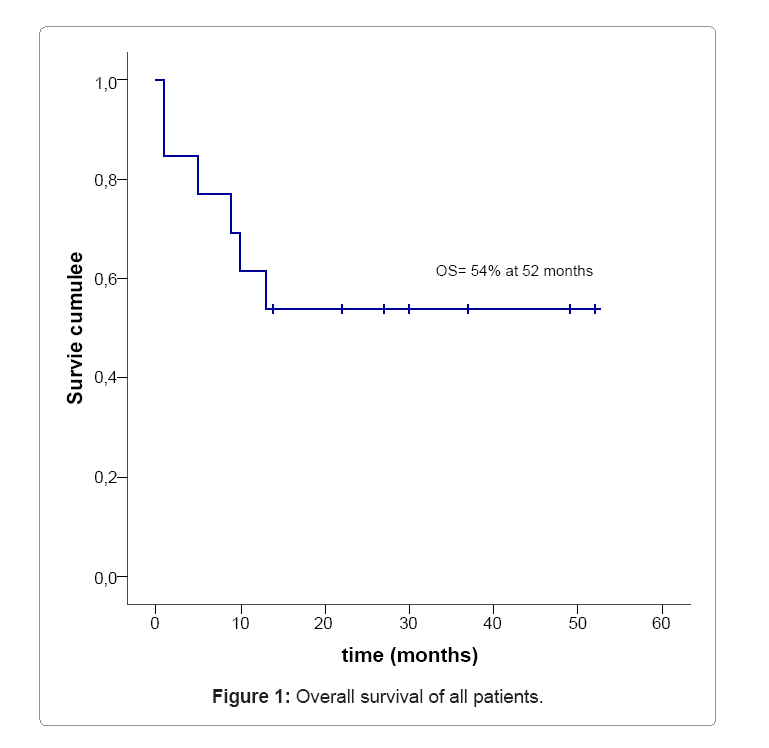
Figure 1: Overall survival of all patients.
Toxicity
No documented thromboembolic event was reported. Hematopoietic toxicity was mild, neutropenia of grades 3 and 4 occurred in two patients. No diabetes or pancreatitis was observed. Three patients died and two of them (refractory to their first treatment) died from sepsis one month after the last course of asparaginase, without detectable disease.
In stage I/II nasal NK/T-cell lymphoma, radiotherapy alone is initially effective but final outcome is unsatisfactory because of frequent systemic progression or relapse (CR rate: 60-70%, 5-year OS: 40-60%) [16-18]. It has therefore been suggested that systemic treatment should be combined with radiation in localized nasal NK/T-cell lymphoma and some researchers have reported promising results with radiotherapy followed by combination chemotherapy (5-year OS: 75-87%) [18,19].
Six patients were refractory to their first treatment with anthracycline-based regimens (CHOP). After the salvage therapy with L-asparaginase-based chemotherapy, three patients achieved CR.
The anthracycline-based chemotherapy produced a CR rate of 36%, a median DFS of 10 months and a median OS of 19 months [20]. These results were still inferior to the results of the L-Asparaginase-based regimen in nasal NK/T cell lymphoma salvage therapy [21-26].
Our study also showed a better CR rate (33%) after salvage therapy with asparaginase than those containing anthracycline-based (Table 2). The overall response with asparaginase-based chemotherapy was (CR+PR) 80%.
After the results obtained with L-Asparaginase salvage therapy in patients with refractory NK/T-cell lymphoma in our institution, we started in March 2010, the study in localized stage nasal NK/Tcell lymphoma with the patients who received the Asparaginasecontaining regimen in first-line therapy. At the time to 31 December, five patients were included and the overall results obtained, showed that L-asparaginase-based chemotherapy as first-line treatment produced a CR rate of 80% in all patients in stage I/II nasal NK/T-cell lymphoma and all of them remained in complete remission with an OS=80% at 30 months. All of the five patients responded nicely and the tumor regressed after the first cycle.
In our study, the L-asparaginase-based chemotherapy produced a CR rate of 80 % in first-line therapy and 33% in the salvage therapy, a median OS in all 13 patients was not reached with 54% of survival in 52 months. In conclusion, our study showed that asparaginase administered in patients with stage I/II nasal NK/T-cell lymphoma is effective and should be explored further.
The authors of this manuscript are grateful to all the participants: Miss Mehalli Samira, and Miss Benmir Imene.
We are indebted to the following pathologists for sending cases: J. Audouin (Hôpital Hôtel Dieu, Paris), F. Benali (EHU 1st November, Oran), F. Hacene (EHU 1st November, Oran). All authors participated in the study conception and/or acquisition of data. The manuscript was approved by all authors.