Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2016) Volume 6, Issue 1
Background: Both exercise training and diet are recommended to prevent and control primary hypertension (HTN) and overweight/obesity. Aerobic exercise is firmly established as an effective measure for lowering blood pressure (BP) and reducing cardiovascular risk. However, there is no agreement about the optimal dose of frequency, intensity, time and type of exercise. This study is a randomized control trial to investigate the effectiveness of different aerobic exercise programs and diet for reducing BP, for improving body composition, cardiorespiratory fitness, biochemical profile, physical activity and sedentary behavior and health-related quality of life in adults with primary HTN and overweight or obesity.
Methods/Design: One hundred sixty-four overweight or obese participants (18-70 yr old) diagnosed with primary HTN will perform different assessments to evaluate BP, physical, biochemical and nutritional condition, sedentary behavior and quality of life before and after 16-week of follow-up. All participants will receive an energy-hypocaloric diet based on 25% of measured resting metabolic rate and will be randomly assigned to control group (only diet) or exercise groups (diet plus aerobic exercise). Participants assigned to an exercise group will train 2 days/week under supervision (treadmill and bike protocol). There will be three aerobic exercise groups: (1) moderate continuous exercise and high volume (MCT) group, (2) high-intensity interval training and high-volume (HV-HIIT) group, and (3) high-intensity interval training and low-volume (LV-HIIT) group. The measurements used in the protocol will be taken before and after the intervention period (16-weeks), and after a six-month period in all participants (i.e., 6 months with only recommendations and no supervision).
Discussion: The results of this intervention will help to better understand the potential of non-pharmacological treatment for improving the well-being of people with primary HTN and overweight or obesity.
Keywords: Hypertension; Obesity; Interval training; Diet
ABPM: Ambulatory Blood Pressure Monitoring; AC: Attention Control Group; BMI: Body Mass Index; BP: Blood Pressure; CPET: Cardiopulmonary Exercise Test; CT: Continuous exercise Training; CVD: cardiovascular diseases; DASH: Dietary Approaches to Stop Hypertension; DBP: Diastolic Blood Pressure; ECG: Electrocardiogram; ESC: European Society of Cardiology; ESH: European Society of Hypertension; FITT principle: Frequency, Intensity, Time or Volume, and Type or Modality; HDL: High-density Lipoprotein Cholesterol; HTN: Hypertension; HR: Heart Rate; HVHIIT: High-Intensity Interval Training and High-Volume group; IPAQ: International Physical Activity Questionnaire; IT: Interval Training; LDL: Low-density lipoprotein cholesterol; LV-HIIT: High-Intensity Interval Training and Low-Volume group; MAP: Mean Arterial Pressure; MCT: Moderate Continuous Exercise Group; MSWT: Modified Shuttle Walking test; PP: Pulse Pressure; SF-36: Short Form Medical Outcome Questionnaire; SBP: Systolic Blood Pressure; VCO2: Carbon Dioxide Production; VO2: Oxygen Uptake; VO2 peak: Peak Oxygen Uptake; VT: Ventilatory Thresholds; VT1: First Ventilatory Threshold; VT2: Second Ventilatory Threshold
Cardiovascular diseases (CVD) are the leading cause of morbidity and mortality worldwide leading to a huge impact on quality of life and healthcare-related costs [1,2]. The knowledge of risk factors for CVD, especially avoidable risk factors, such as smoking, hypertension (HTN), hyperlipidemia, obesity and physical inactivity is essential and may contribute to a reduction in the incidence of CVD [2]. In this sense, HTN is considered one of the most preventable causes of premature morbidity and mortality worldwide. Primary HTN refers to the majority of people with sustained high blood pressure (BP, approximately 90%) encountered in clinical practice, for which there is no identifiable cause [3]. The prevalence of HTN is strongly influenced by age and lifestyle factors [3,4]. Overweight or obesity and HTN frequently coexist in the same person being additive in terms of cardiovascular risk. Adding to that, it has been shown that people with HTN are less physically active than those without HTN [5]. A sedentary lifestyle associated with low cardiorespiratory fitness, along with higher total cholesterol, body mass index (BMI), and levels of obesity, but lower high-density lipoprotein cholesterol (HDL-c) is common among people with HTN [6].
Hypertension is defined as values >140 mmHg systolic BP (SBP) and/or >90 mmHg diastolic BP (DBP) with classification of BP levels by the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC) [7]. Obesity and being overweight are medical conditions in which excess body fat has accumulated to the extent that it may have a negative effect on health. Body mass index provides the most useful population-level measure of obesity (overweight ≥ 25.0 kg/m2, obesity ≥ 30.0 kg/m2). Nevertheless, BMI does not account for the wide variation in body fat distribution. Therefore, measurement of waist circumference provides a simple and practical method to add to BMI along with additional tools such as measuring body composition (i.e., electrical bioimpedance [8]) or energy intake [9].
Drug therapy remains the mainstay of HTN management. However, because antihypertensive drugs are not without their side effects, present guidelines strongly recommend appropiate lifestyle changes for the prevention and treatment of HTN [7,10]. Thus, intervening simultaneously by adressing smoking cessation, and weightloss through dietary treament and increased exercise, safely and effectively delays or prevents HTN in non-hypertensives [11].
In the last two decades, various studies have shown the effectiveness of adherence to a dietary pattern known as the DASH diet (dietary approaches to stop hypertension) in reducing both SBP and DBP, improving health and quality of life, prevention of cardiovascular disease, metabolic syndrome, diabetes and mortality from all causes in different populations [12,13]. It has also been shown that in patients with elevated BP, compared to DASH diet alone, the combination of the DASH diet with exercise and weight loss resulted in greater reduction of BP and improved cardiovascular biomarkers [14].
Regular exercise is highly recommended for both prevention and treatment of HTN and for lowering cardiovascular risk and mortality [7]. However, there is a substantial lack of evidence on many issues surrounding BP treatment and management in adults with HTN, including exercise prescription and its design. The components of the FITT principle (i.e., frequency, intensity, time or volume, and type or modality) constitute the exercise dose needed to improve health, in a way similar to a pharmacologic intervention, making it mandatory for it to be designed in a systematic and individualized manner by an exercise specialist [15]. The intensity and modality of aerobic exercise has also been presented in different guidelines and associations [7,15]. There appears to be a general consensus for recommending moderateto high intensity continuous exercise training (CT) as antihypertensive therapy. Nonetheless, the American Heart Association, ESH and ESC also endorse high-to severe intensity exercise through interval training (IT). In contrast with the CT protocol, IT alternates short bouts of high-to severe intensity exercise with a few minutes of light-to moderate exercise in the intervening periods [6,7,15,16]. Based on the results of previous studies, both CT and IT programs are effective adjunct, non-pharmacological management of chronic essential HTN [10,17,18]. Adding to that, health-related adaptations to low-volume and high intensity interval training have been presented. This type of training is characterized by sessions that involve a relatively small total amount of exercise at high-intensity (i.e., ≤ 10 min).
On the other hand, the long term detraining effect [19] has not been studied enough in the primary hypertensive population. Despite the evidence of physiological decline during detraining, there is a scarcity of data in assessing how functional fitness or control of BP changes following the cessation of exercise supervision. Further, it would be very interesting to observe whether the rehabilitation strategy for people with HTN and overweight is persistent with the changes in dietary habits, exercise behaviors, body weight and BP after the intervention with no supervision and only recommendations. No data is available regarding the influence of no supervision effects after different types of intensity and volume exercise in this population.
Considering all the above mentioned in HTN population: (1) the combination of the DASH diet with exercise seems critical in greater reduction of BP and improved cardiovascular biomarkers, and (2) there is no agreement in exercise design and best physical activityrecommendations from professional organizations, and given that (3) no previous studies have compared the effects of a combined dietary treatment specific to HTN with exercise training at different intensities and modalities (i.e., CT and IT) and volumes (i.e., high- and lowvolume) in overweight and primary hypertension population; EXERDIET-HTA study is designed to investigate what effect different 16-week aerobic EXERcise programs with nutritional intervention (hypocaloric DIET) will have in primary hypertensive and overweight/ obese adults during an extended unsupervised period.
We hypothesize that: (1) diet and aerobic exercise treatment will be more effective for reducing BP, and improving body composition, biological markers, health-related quality of life and cardiorespiratory fitness than only dietary treatment, in adults with overweight or obesity with primary HTN, (2) high-intensity interval training will get superior improvements in cardiovascular health than moderate training, (3) a high-intensity and low-volume exercise program will get similar results compared to high-intensity and high volume exercise program, and 4) beneficial effects of diet and exercise intervention will be sustained in some degree after six-month period with no supervision.
Therefore, the primary objectives of the EXERDIET-HTA (HTA is the acronym for arterial hypertension in Spanish) study are: (1) to assess the changes in selected parameters of BP, cardiorespiratory fitness, body composition and biological markers brought about by a 16-week period of different aerobic exercise programs with hypocaloric diet for overweight or obesity and primary hypertensive adults, and (2) to examine the effect of six months with no supervision subsequent to intervention. The secondary objectives are to examine the additional effect of the intervention on physical activity behavior and health-related quality of life.
Study design
The present study is a randomized controlled trial (ClinicalTrials.gov ID: NCT02283047). The Ethics Committee of the University of the Basque Country (UPV/EHU, CEISH/279/2014) and the Ethics Committee of Clinical Investigation of Araba University Hospital (2015-030) have approved the study design, study protocols and informed consent procedure.
All participants have to provide written informed consent. After baseline measurements, they will be randomly allocated to one of the four intervention groups. The participants will be followed for 16 weeks, as well as after six months of unsupervised period. All followup examinations will be performed in the same laboratory setting and by the same researchers as in the baseline measurements.
Participants and selection criteria
EXERDIET-HTA participants will include 164 adults with primary HTN and overweight or obesity recruited from the cardiology services from the physician specialist and from local media. Interested individuals will be invited to contact the research team. Before starting the study, a screening will be performed of all candidates. After completion of the informed consent process, participants will undergo anthropometric screening (stature, total body mass, waist and hip circumferences) and will be selected for inclusion if they are classified as overweight or obese. Likewise, sedentary behavior will be determined through the International Physical Activity Questionnaire (IPAQ) to ensure personal compliance with "Global Recommendations on Physical Activity for Health" by the World Health Organization [20]. Moreover, all participants will be assessed with a 12-lead electrocardiogram (ECG) in order to detect a left ventricular hypertrophy or any other predictor of cardiovascular events. Echocardiography will be indicated by the cardiologist when more sensitive diagnosis is needed for the inclusion. Participants taking medication with beta-blockers are eligible only if the treatment will allow a peak cardiopulmonary test at baseline. Otherwise, the cardiologist will advise the most suitable pharmacological treatment. Participants with no diagnosis of HTN will be assessed with ambulatory blood pressure monitoring (ABPM) to confirm the HTN status by the cardiologist. The inclusion and exclusion criteria for EXERDIET-HTA study are shown in Table 1.
| Inclusion criteria | Age: 18-70 years old |
| Diagnosis of primary HTN, 1-2 stage defined as SBP 140-179 mmHg and / or DBP of 90-109 mmHg | |
| Overweight or obese (BMI ≥ 25 kg/m2) | |
| Sedentary lifestyle according to IPAQ scale | |
| Time availability (90 min, two days a week for 16 weeks) to carry out the exercise program | |
| Exclusion criteria | Secondary HTN |
| Left ventricular hypertrophy (estimated left ventricular mass up to 103 g/m2 for men and up to 89 g/m2 for women) [21] | |
| The presence of one severe or, uncontrolled, cardiovascular risk factor, or diabetes mellitus more than 10 years since diagnosis, or with associated organopathy | |
| Other significant medical conditions: Including but not limited to chronic or recurrent respiratory, gastrointestinal, neuromuscular, neurological, or psychiatric conditions; musculoskeletal problems interfering with exercise; autoimmune or collagen vascular diseases; immunodeficiency diseases or a positive HIV test; anemias, bleeding disorders, chronic thrombotic disorders, or hypercoagulable states; malignancies in the past 5 years, with the exception of skin cancer therapeutically controlled; endocrine and metabolic disorders, including type 1 diabetes; any other medical condition or disease that is life-threatening or that can interfere with or be aggravated by exercise | |
| Pregnancy or breast-feeding | |
| Plans to be out of the city more than 2 weeks | |
| To have participated in a diet-weight-loss program during the last year |
Table 1: Inclusion and exclusion criteria for EXERDIET-HTA study.
Measurements
The measurements used in the protocol will be taken before and after the intervention period (16-weeks), and after a six-month period in all participants (Figure 1). The post intervention test will be scheduled the following week after finishing the 16-week intervention period, and six months later. The primary outcome variable is BP. The secondary outcome variables include physical fitness, body composition, biochemical profile, physical activity level, and health related quality of life (Table 2). Both the baseline and follow-up measurements will be divided into four sessions (Table 2).
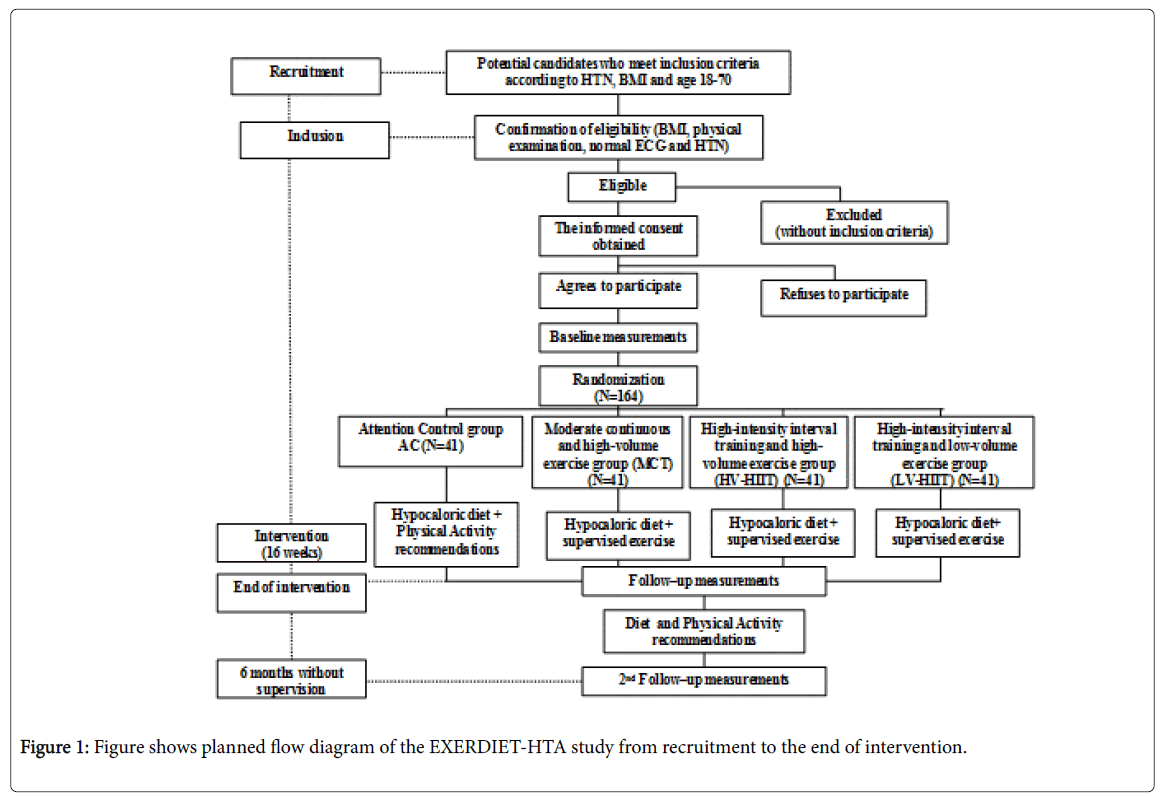
Figure 1: Figure shows planned flow diagram of the EXERDIET-HTA study from recruitment to the end of intervention.
| Session | Measurement | Methodology |
|---|---|---|
| DAY 1 | Physical Measurements | |
| Stature (cm) | Stadiometer | |
| Body mass (kg) | Scale | |
| Waist and hip circumferences (cm) | Non-elastic tape | |
| Fat free mass, fat mass, total body water | Bioelectrical impedance | |
| Systolic and diastolic blood pressure | Oscillometric monitor device | |
| Rest electrocardiogram | 12-lead electrocardiogram | |
| Physical Activity & Sedentary Behaviour | ||
| International Physical Activity Questionnaire | Questionnaire | |
| Accelerometry (1 week) | Accelerometer | |
| DAY 2 | Blood pressure assessment | |
| Mean systolic and diastolic blood pressures, mean arterial pressure, pulse pressure (24 h) | Ambulatory blood pressure monitor | |
| DAY 3 | Physical fitness | |
| Cardiorespiratory fitness | Modified Shuttle Walking Test | |
| Cardiopulmonary exercise test (bike) | ||
| Health related quality of life | SF-36 questionnaire | |
| Dietary assessment | 24 h recalls and food frequency questionnaires | |
| DAY 4 | Biochemical Measures | |
| Glucose (mg/dl) | Enzymatic spectrophotometry | |
| Insulin | Immuno assay chemiluminescent | |
| Haemoglobin A1c (%) | High-performance liquid chromatrography ion exchange (HPLC) | |
| Total-, HDL- and LDL-cholesterol (mg/dl) | Enzymatic spectrophotometry | |
| Tryglicerides (mg/dl) | Enzymatic spectrophotometry | |
| Alanine aminotransferase (U/L) | Enzymatic spectrophotometry | |
| Aspartate aminotrnsferase (U/L) | Enzymatic spectrophotometry | |
| C-reactive protein (g/dl) | Enzyme immuno assay | |
| Uric acid (mg/dl) | Enzymatic spectrophotometry | |
Table 2: Overview of the assessment schedule at baseline and follow-up in the EXERDIET-HTA study.
Blood pressure
Ambulatory BP monitoring will be performed with an oscillometric ABPM 6100 recorder (Welch Allyn, New York, USA) [22]. We will follow the report’s recommendations by the ESH/ESC guidelines [7] to ensure the best methodology. The device will measure BP at 30-minute intervals during the daytime and at 60-minute intervals during night-time. Participants will have previously self-disclosed their typical bedtime and wake up time, and it will be used to define the assessments per 30 min intervals, and the beginning per 60 min intervals. Recorded data will be downloaded with participant’s attendance in order to correct the actual bed-time and wake-up time in case of change. The recording will be accepted if at least 75% of the recordings are obtained. If the ABP fails to measure the BP, another ABP will be performed. The values used for statistical analyses will be mean systolic and diastolic blood pressures, mean daytime and nighttime values, mean arterial pressure (MAP) calculated as [DBP + 0.333 x (SBP-DBP)], double product (heart rate x SBP) and pulse pressure (PP).
Physical fitness
Physical fitness includes the Modified Shuttle Walking test (MSWT) and a peak, symptom-limited cardiopulmonary exercise test (CPET).
The MSWT will require the participant to walk up and down a 10 m course and it will be performed as previously described by Singh et al. [23]. Participants will walk along a flat, indoor 10 m course marked by two cones placed 0.5 m in from each end of the course. A shuttle refers to one 10 m lap. Standardized prerecorded instructions for the test will be played from a digital recording immediately prior to beginning the test. The test will be externally paced, with signal beeps at regular intervals to indicate when the participant should be turning around the cone to commence the next shuttle. A triple beep will signal the next level and an increase in walking speed. Participants will commence the test at a walking speed of 0.5 m/s (level 1), allowing the participant 20 seconds to complete each of the three shuttles in level 1. There is a speed increment of 0.17 m/seconds each minute for a maximum of 15 minutes. The test will be stopped when the participant can no longer maintain the required pace or is more than 0.5 m from the cone before the signal beep after one opportunity to catch up or if the test is completed. Additional criteria for early termination of the test will include patient distress, dizziness, angina, or onset of severe musculoskeletal pain, failure of the heart rate (HR) to increase with exercise or attainment of 85% of the maximum HR. The number of shuttles completed will be recorded at the completion of each test and converted to the distance walked. Prior to commencing the test, with the participant in a seated position, baseline HR and BP will be recorded. Heart rate and Borg scale (6 to 20) will be monitored throughout the test, and BP and HR will continue to be recorded five more minutes after completion of the test [24,25].
Participants will be allowed a 30 minute rest break prior to commencing the CPET test in order to get baseline HR and BP values.
The CPET will be performed in the upright position on an electronically braked Lode Excalibur Sport Cycle Ergometer (Groningen, The Netherlands). Testing protocol will start with 40 W with gradual increments of 10 W every minute to exhaustion with continuous ECG monitoring. Each participant’s bike setup (i.e., saddle height, reach, and handle bar height) will be recorded and registered to replicate at follow-up. The test will not be preceded by any type of warm-up, and participants will cycle at least at 70 rpm. During the test, participants will be encouraged verbally by the laboratory technician and medical doctor. Expired gas analysis will be conducted using a commercially available system (Ergo CardMedi-soft S.S, Belgium Ref. USM001 V1.0) that will be calibrated before each test with a standard gas of known concentration and volume. Breath-by-breath gas exchange data will be measured continuously during exercise and averaged every 60 seconds. Peak oxygen uptake is defined as the highest oxygen uptake (VO2 peak) value attained toward the end of the test. Achievement of true peak effort can be assumed in the presence of two or more of the following criteria: 1) volitional fatigue (>18 on BORG scale), 2) peak respiratory exchange ratio (VCO2/VO2) ≥ 1.1, 3) achieving >85% of age predicted HRmax, and 4) failure of VO2 and/or HR to increase with further increases in work rate [26].
A self-reported Borg rating of perceived exertion (6 to 20 scale) will be recorded at the end of each stage. Blood pressure will be measured every two minutes throughout the test. Ventilatory thresholds (i.e. VT1 and VT2) will be assessed by standardized methods using the V-slope and ventilatory equivalents. First ventilatory threshold (VT1) can be identified as the point of transition in the carbon dioxide production (VCO2) vs. VO2 slope from less than 1 to greater than 1, or VT1 is also identifiable as the nadir of the ventilatory equivalent (VE) of VO2 vs work rate relationship. Second ventilatory threshold (VT2) is identifiable as the nadir of the VE/VCO2 vs work rate relationship [26]. After completion of the test, participants will remain on the bike five more minutes for recovery with ECG and BP monitoring. Absolute and relative indications for terminating the exercise test will be taken into account [27]. The identification of the two VT will determine the three different exercise intensity domains or ranges for exercise design (R1, R2, R3): R1) light to moderate exercise intensity with HR values below VT1; R2) moderate to high or vigorous exercise intensity with HR values between VT1 and VT2, and R3) high to severe intensity exercise intensity with HR values up to VT2 to peak intensity. When it is not possible to identify the VT2, exercise intensity domains are established taking into account percentages of HR reserve, i.e., moderate intensity is defined between 50-75% of HR reserve, high intensity from ≥ 76% to <95% of HR reserve [26].
Anthropometry and body composition
Anthropometry will include stature (SECA 213), total body mass (SECA 869), body mass index calculated as [total body mass (kg)/ stature (m2)], and waist and hip circumferences (SECA 200) to calculate waist to hip ratio. All measurements will be taken in accordance with guidelines from International Society for the Advancement of Kinanthropometry [28]. Furthermore, fat free mass, total body water and fat mass will be estimated with bioelectrical impedance analysis (Tanita, BF 350).
Biochemical profile
Morning fasting blood samples will be obtained from each participant by experienced nursing staff in the Clinical Trials Unit of Tecnalia (HUA, Vitoria-Gasteiz). This procedure will permit measurements of glucose, insulin, haemoglobin A1c (HbA1c), lipid profile (total-, high-density lipoprotein (HDL)- and low-density lipoprotein (LDL)-cholesterol, and triglycerides), liver enzymes (ALT, AST), C-reactive protein and uric acid. Insulin resistance will be determined by the homeostasis model assessment for insulin resistance (HOMA-IR) [29].
Physical activity and sedentary behavior
Physical activity and sedentary behavior will be objectively (i.e. accelerometry) and subjectively (i.e. questionnaires) assessed.
Accelerometry: Participants will be asked to wear a triaxial accelerometer (ActiGraph GT3X+, Pensacola, Florida,US) on their non-dominant wrist for eight consecutive days at all times, except during water-based activities. In the analyses bouts of 60 continuous minutes of 0 activity intensity counts will be excluded, considering these periods as non-wearing time. Monitor wearing time will be calculated by subtracting the non-wearing time and the sleeping time (recorded through a diary) from the total registered time for the entire day (typically 1,440 min). Detailed information on the ActiGraph accelerometer can be found elsewhere [30]. Estimates for moderate-tovigorous physical activity will be summarized in 1-min time intervals. An activity count below 100 counts per minute (i.e., 0 to 99 cpm) will be used to classify sedentary behavior; activity counts between 100 and 2019 cpm will be used to classify time spent in light-intensity physical activity; activity counts between 2020 and 5998 cpm will be used to classify time spent at moderate-intensity and activity counts at or greater than 5999 cpm will used to classify time spent at vigorous intensity [31,32]. Regarding light-intensity physical activity, two separate cut-off points will be used to differentiate low-light (100-750 cpm) vs high-light (750-2019 cpm) [33]. Participants will be classified as sedentary if they do not engage in at least 150-min of moderate intensity or 75-min of vigorous-intensity physical activity per week.
The international physical activity questionnaires (IPAQ): The short version of IPAQ will be used to assess sedentary behavior. This questionnaire is an instrument developed to enable the estimation of the level of physical activity in populations across different countries. The short version is composed of eight questions that are used to estimate the time spent per week performing different physical activity intensities. The short IPAQ will record the activity at four intensity levels: (1) vigorous-intensity, (2) moderate-intensity, (3) walking or light activity and (4) sitting. For all intensity levels, the participants will be asked how many days per week and minutes per day they performed the activity for ≥ 10-min continually [34]. To quantify the physical activity levels, the product of the duration (min/day) and frequency (days/week) will be used to estimate light, moderate-tovigorous and total physical activity.
Health-related quality of life
Participants’ health-related quality of life will be determined using the 36-item Short Form Medical Outcome Questionnaire (SF-36) [35]. It is a 36-item questionnaire that measures eight multi-item dimensions of health: physical functioning, social functioning, role limitations due to physical problems, and role limitations due to emotional problems, mental health, energy/vitality, body pain, and general health perception. Scores will be coded, summed, and converted onto a scale from 0 (worst possible health state) to 100 (best possible health state) for each dimension item.
Dietary assessment
Habitual food consumption and nutrient intake will be evaluated using three questionnaires: dietary history, food frequency questionnaire and 24h recall questionnaire.
After baseline testing, participants will be randomized to one of the four intervention groups (AC, MCT, HV-HIIT, LV-HIIT) stratified by gender, SBP, BMI and age using a time-blocked computerized randomization program. Medical staff will be blinded to participant randomization assignment.
Attention control group (AC)
The AC group will receive treatment only with hypocaloric diet and also standard recommendation for patients with primary HTN, including regular physical exercise. In this sense, hypertensive patients will be advised to participate, without supervision, in at least 30 min of moderate-intensity dynamic aerobic exercise (walking, jogging, cycling or swimming) 5-7 days per week. Aerobic interval training including high intensity exercise and dynamic resistance exercise (force development associated with movement) will also be recommended [7]. Participants will receive information related to HR values regarding moderate and high exercise intensity domains for the selfmonitoring of exercise intensity.
Exercise groups will receive double treatment (i.e. hypocaloric diet + supervised exercise):
• MCT group: Moderate (HR values between VT1 and VT2 or 50-75% of HR reserve) continuous exercise and high volume increasing gradually from 20 to 45 min;
• HV-HIIT group: high-intensity (HR values up to VT2 to peak intensity or ≥76% to <95% of HR reserve) interval training and high-volume increasing gradually from 20 to 45 min and alternating high and moderate intensities at different protocols; and
• LV-HIIT group: high-intensity interval training and low-volume (20 min) alternating high and moderate intensities at different protocols.
Exercise intervention program
The participants will exercise two nonconsecutive days per week for 16 weeks under supervision by exercise specialists. All the exercise sessions will start and finish with BP monitoring and training intensity will be controlled by HR monitoring (Polar Electro, Kempele, Finland) and through the rate of perceived exertion using the Borg’s original scale (6-20 point). Each session will include a 10 min warm-up with joint mobility and coordination exercises with continuous leg movement to facilitate venous return and a 10 min cool-down period with basic core strengthening exercises and passive stretching exercises on the floor to ensure a progressive return to the resting values of both HR and BP. The main portion of the training session will consist of aerobic exercises (i.e., one day of the week on the treadmill, and the second one on the bike) developing progressively both the volume (i.e., 20 to 45 min in MCT and HV-HIIT, whereas in LV-HIIT the duration will be always of 20 min) and intensity. Intensity will be individually tailored to HR at moderate or vigorous intensities, adjusting the speed and incline of the treadmill or the power and speed on the bike, to achieve the planned target HR (Tables 3-5). The exercise specialists will keep detailed records of all the exercise sessions reporting the HR and Borg scale values of every interval. The importance of targeting moderate and high intensity will be emphasized.
| MCT | ||
|---|---|---|
| Weeks | Total Volume (min) | INTENSITY (%HR res) |
| 1-2 | 20 | 50% |
| 3-4 | 25 | 60% |
| 5-6 | 30 | 65% |
| 7-8 | 35 | 70% |
| 9-10 | 40 | 75% |
| 11-12 | 45 | 75% |
| 13-16 | 45 | 75% |
Table 3: Intervention program for Moderate Continuous Training (MCT) group. Volume and intensity progression.
| HV-HIIT | LV-HIIT | |||||||
|---|---|---|---|---|---|---|---|---|
| HIGH-INTENSITY INTERVAL | MODERATE INTENSITY INTERVAL | HIGH-INTENSITY INTERVAL | MODERATE INTENSITY INTERVAL | |||||
| Weeks | Volume (min) | Intensity (%HRres) | Volume (min) | Intensity (%HRres) | Volume (min) | Intensity (%HRres) | Volume (min) | Intensity (%HRres) |
| 1-2 | 8 | 80 | 12 | 60 | 8 | 80 | 12 | 60 |
| 3-4 | 12 | 80 | 13 | 60 | 8 | 80 | 12 | 60 |
| 5-6 | 16 | 85 | 14 | 65 | 8 | 85 | 12 | 65 |
| 7-8 | 16 | 85 | 19 | 65 | 8 | 85 | 12 | 65 |
| 9-10 | 16 | 95 | 24 | 70 | 8 | 95 | 12 | 70 |
| 11-12 | 16 | 95 | 29 | 70 | 8 | 95 | 12 | 70 |
| 13-16 | 16 | 95 | 29 | 70 | 8 | 95 | 12 | 70 |
Table 4: Intervention program for High-Volume High-Intensity (HV-HIIT) and Low-Volume High-Intensity (LV-HIIT) groups on the treadmill. Volume and intensity progression.
| HV-HIIT | LV-HIIT | |||||||
|---|---|---|---|---|---|---|---|---|
| HIGH-INTENSITY INTERVAL | MODERATE INTENSITY INTERVAL | HIGH-INTENSITY INTERVAL | MODERATE INTENSITY INTERVAL | |||||
| Weeks | Volume (min) | Intensity (%HRres) | Volume (min) | Intensity (%HRres) | Volume (min) | Intensity (%HRres) | Volume (min) | Intensity (%HRres) |
| 1-2 | 2 | 80 | 18 | 60 | 2 | 80 | 18 | 60 |
| 3-4 | 3 | 80 | 22 | 60 | 3 | 80 | 17 | 60 |
| 5-6 | 4 | 85 | 26 | 65 | 4 | 85 | 16 | 65 |
| 7-8 | 5 | 85 | 30 | 65 | 4:30 | 85 | 15:30 | 65 |
| 9-10 | 6 | 95 | 34 | 70 | 4:30 | 95 | 15:30 | 70 |
| 11-12 | 7 | 95 | 38 | 70 | 4:30 | 95 | 15:30 | 70 |
| 13-16 | 9 | 95 | 37 | 70 | 4:30 | 95 | 15:30 | 70 |
Table 5: Intervention program for High-Volume High-Intensity (HV-HIIT) and Low-Volume High-Intensity (LV-HIIT) groups on the bike. Volume and intensity progression.
Several strategies will be implemented to maximize adherence, including music in all sessions, individualized attention at the intervention sessions and telephone calls following missed sessions.
High-intensity interval training protocol on the treadmill
The high intensity aerobic exercise groups will carry out a 5-min warm-up period at a moderate-intensity (i.e., HR values between VT1 and VT2 or 50-75% of HR reserve) on the treadmill, before walking two intervals of 4 min at high-intensity (i.e., HR values up to VT2 to peak intensity or ≥ 76% to <95% of HR reserve). The participants will exercise at the lower intensity limit for the first two weeks of the training period before increasing the intensity towards the upper limit. Between the high-intensity intervals 3 min of walking at moderateintensity will be conducted. The training session will end with a 1-4 min cool-down period at moderate-intensity [36]. This will give a total exercise time of 20 min. Meanwhile this protocol will be kept in the LV-HIIT group; every two weeks the HV-HIIT will progress to four intervals of 4 min at high intensity and 45 min of total volume (Table 4).
High-intensity interval training protocol on the bike
The high intensity aerobic exercise groups will carry out a 10-min warm-up period on the bike for the high-volume group and 5-10 minutes for the low-volume group. After that participants will cycle for 30 s at high-intensity (i.e., HR values up to VT2 to peak intensity or ≥ 76% to <95% of HR reserve) followed by 60 s at moderate-intensity (i.e., HR values between VT1 and VT2 or 50-75% of HR reserve). Four repetitions (1rep=30 s high-intensity followed by 60 s moderateintensity) will be initially performed in both groups and gradually increased to 18 repetitions in the high-volume group, while 9 repetitions will be completed (Table 5) in the low-volume group. The training session will end with a 5-10 min cool-down period at moderate-intensity.
Diet intervention
Diet will be calibrated with the Easy Diet program (www.easydiet.es) by the Spanish Foundation of dieticians and nutritionists) obtaining caloric intake and macronutrient distribution. The resting energy expenditure will be calculated by the Mifflin St Jeor equation to be the most appropriate for individuals who are overweight or obese [37,38] and the coefficient of 1.5 corresponds to the factor of physical activity for light physical activity level or sedentary individuals. All participants will be treated with a diet designed to provide 25% less energy than their daily energy expenditure. Approximately 30% of their energy intake will come from fat, 15% from protein, and 55% from carbohydrates designed to achieve a weekly loss of body mass between 0.5 and 1.0 kg in accordance with the recommendations of the American Diabetes Association and the Spanish Society for the Study of Obesity [39,40]. From a qualitative point of view, the diet will be designed following the proportions and amounts of foods/food groups recommended by the dietary pattern of the DASH diet [13]. In addition, participants will receive nutritional advice regarding the restriction of foods high in sodium according to the recommendations of the European Societies of Hypertension and Cardiology [7]. The diet will also be accompanied by guidance menus and the most appropriated culinary techniques to facilitate compliance and dietary adherence. Participants will be encouraged, weighed and receive advice and nutritional counseling every two weeks to help in their compliance with the dietary recommendations and requirements.
Six-month period with no supervision after intervention
After the 16-week intervention the participants will receive diet and exercise recommendations for the following six months, but no further intervention or attention from any of the research staff. Regarding physical activity, they will be advised with the same recommendations that the AC group received at the beginning of the intervention, including regular physical exercise. Participants will also receive information related to HR values regarding moderate and high exercise intensity domains for self-monitoring of exercise intensity. They will be asked to try to have similar dietary intakes during this period and to follow the recommendations by the Spanish Society of Dietetics and Food Sciences and the Spanish Society of Community Nutrition.
Data analysis
The required sample size was determined for the primary outcome variable, i.e. mean BP. It was identified that adequate power (i.e., 0.95) to evaluate differences in our design consisting in four experimental groups would be achieved with 164 people (41 each group, α=0.05, effect size f=0.4). Previous studies have reported losses to follow-up between 4-17%. Assuming a maximum loss of follow-up of 20%, the plan will be to recruit a total of 196 hypertensive and overweight people. The statistical analysis will be performed using IBM SPSS Statistics, Version 22.0. Armonk, NY: IBM Corp. Two parametric tests will be performed, after all assumptions for each test are met. For comparisons between groups at baseline (attention control group vs. exercise groups) one-way analysis of variance or the non-parametric method of Kruskall-Wallis and Chi-square test will be used. The ttest for dependent samples will compare the baseline and follow-up mean values of all the independent variables. The general Lineal Model will be used to assess training effects [time (pre-post 16-week intervention) x group interaction] on the primary and secondary study outcomes. The differences between drop-outs and participants who remain in the study will be examined, and the data will be analysed according to the intention-to-treat principle [40]. For each outcome variable the effect size and the level of significance corresponding to the main group (between-subjects), time (within-subjects) and interaction (group x time) will be reported. To prevent type I error, post hoc comparisons (pre vs. post by group) will be performed when a significant interaction effect is present. The same tests will be performed to assess the effect after the six-month unsupervised period. Values will be expressed as mean ± SD. The significance level will be set at 95% (α=0.05).
Currently, at epidemiological level, developed countries are in a stage called “the age of delayed degenerative diseases”. Although CVD are the major causes of morbidity and mortality, a better treatment and prevention would help avoid deaths among these with disease and delay primary events [2].
In 2013 the ESH and ESC published the new guidelines on HTN. Among treatment strategies appropriate lifestyle changes continue being the cornerstone for the prevention and reduction of HTN, as well as adding the control of other cardiovascular risk factors and clinical conditions. Both diet (including, salt restriction, moderation of alcohol consumption, and high consumption of vegetables and fruits and low-fat) and regular physical exercise (including aerobic exercise training at different intensities) are highly recommended [7]. However, based on the review of the literature, several issues are still open to question and would benefit from further investigation:
Does high intensity interval aerobic exercise provide more benefits to lower BP over traditional moderate continuous aerobic exercise?
Could we say “less is more” with lower-volume exercise training in primary hypertension and overweight/obese people?
Which combination of treatment (diet vs. diet+exercise) is most valuable in reducing cardiovascular risk in primary hypertension?
Results of this intervention will help to better understand the potential of non-pharmacological treatment for improving the wellbeing of people with primary HTN and overweight or obesity by implementing an individualized aerobic exercise and hypocaloric diet program.
The authors have declared that no competing interest exists
The study is supported by the University of the Basque Country (GIU14/21 and EHU14/08) and by the Government of the Basque Country (SAIOTEK, SAI12/217). Our special thanks to Ignacio Camacho-Azkargorta, the cardiologist who began to move forward this project and Jessica Werdenberg for reviewing the manuscript.
NCT02283047