Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2016) Volume 6, Issue 1
Agave inulin is non-digestible/fermentable carbohydrates capable of counteracting metabolic related alterations through the modification of the gut microbiota. The fructo-oligosaccharide content of agave inulin differs from inulin extracted from chicory root. The aim of this study was to assess the efficacy and safety of agave inulin on the metabolic profile of overweight and obese dyslipidemic patients. An open clinical trial was carried out in 30 overweight and obese subjects, between 30 and 70 years old. All subjects received 15 g/day of inulin in the morning, during 60 days. Biochemical and metabolic profiles before and after pharmacological intervention were performed. After inulin administration, it was statistically significant decrease: fasting glucose levels (83.1 ± 13.4 vs. 76.5 ± 12.6 mg/dl; p=0.006), triglycerides and glucose (TyG) index (3.9 ± 0.1 vs. 3.8 ± 0.2; p=0.021) and urea (31.4 ± 8.6 vs. 26.3 ± 5.4 mg/dl; p=0.001), thus an increase in sodium levels (139.3 ± 3.0 vs.140.4 ± 2.1 mg/dl; p=0.021), was also found. Similarly, eventhough no statistical differences were detected for all cases, the serum concentration decreased 37% for total cholesterol (TC), 23% for LDL -c, 53% for total triglycerides (TG) and 63.3% for HBA1c while HDL-c levels increased. Anthropometric parameters did not change within the group and the soluble fiber intake did not produce any important gastrointestinal adverse effects. In this study, the increased fiber intake of inulin from Agave tequilana Weber blue variety was effective and safe in reducing glucose and urea levels as well as insulin resistance in overweight and obese dyslipidemic patients; however, sodium levels were increased but were not clinically significant.
Keywords: Overweight, Dyslipidemia, Atherosclerosis, Cholesterol, Diabetes, Obesity
Dyslipidemia is a common disorder of an abnormal amount of lipids in the blood which favors atherosclerosis and its consequences, primarily ischemic heart disease. The Mexican National Health and Nutrition Survey [1] estimated for 2012 in Mexican adults 20 years or older, the prevalence of dyslipidemia for Total Cholesterol (TC) ≥ 200 mg/dl was 50.6% and for Triglycerides (TG) ≥ 150 mg/dl, 32.5%. Furthermore, the estimation for overweight was 38.8% (BMI ≥ 25.0-29.9 kg/m2) and for obesity 32.4% (BMI ≥ 25.0-29.9 kg/m2). Finally, a combined prevalence for overweight and obesity was 71.2% [2], considering these last two statistics as the highest observed in the American continent, even higher than the United States of America [3]. Other studies have reported higher mean values for TG and lower values for HDL cholesterol (HDL-c) in the presence of other cardiovascular risk factors such as diabetes, hypertension and obesity [4]. These diseases not only represent a serious public health problem with a social and economic impact, but the prophylaxis and treatment by several specialists is also required [5].
In the administration of hypolipidemic agents, a higher emphasisis placed on reducing cardiovascular risk (secondary prevention) than the management of initial dyslipidemia (primary intervention) [6]. Statins inhibit 3-hydroxy-3-methylglutaryl coenzyme A reductase in the conversion to mevalonate resulting in decreased production of cholesterol de novo, but this mechanism can increase creatine kinase levels, however, a small percentage of patient’s present myalgias and the increase of hepatic enzymes [7]. Furthermore, the cost effectiveness of treatment has a great influence on treatment adherence, mainly in the first primary care level [8]. Consequently, it becomes very important to continue evaluating easy-access therapies at lower cost with less or null collateral effects.
It has been proposed that some carbohydrates, which are fermented in the caeco-colon, might be of particular interest in the field of dyslipidemia and obesity. Fructans are non-digestible and fermentable carbohydrates, which have interesting metabolic effects (decrease in fat mass development, steatosis and glycaemia), by acting through a mechanism different from the common dietary fibers prone to act on lipid metabolism to decrease the hepatic lipogenesis and plasma triacylglycerol concentrations [9], as they exhibit non gel-forming properties. Inulin-type fructans extracted from chicory roots regulate appetite and lipid/glucose metabolism, namely, by promoting glucagon-like peptide-1 (GLP-1) production in the colon [10] (Figure 1).
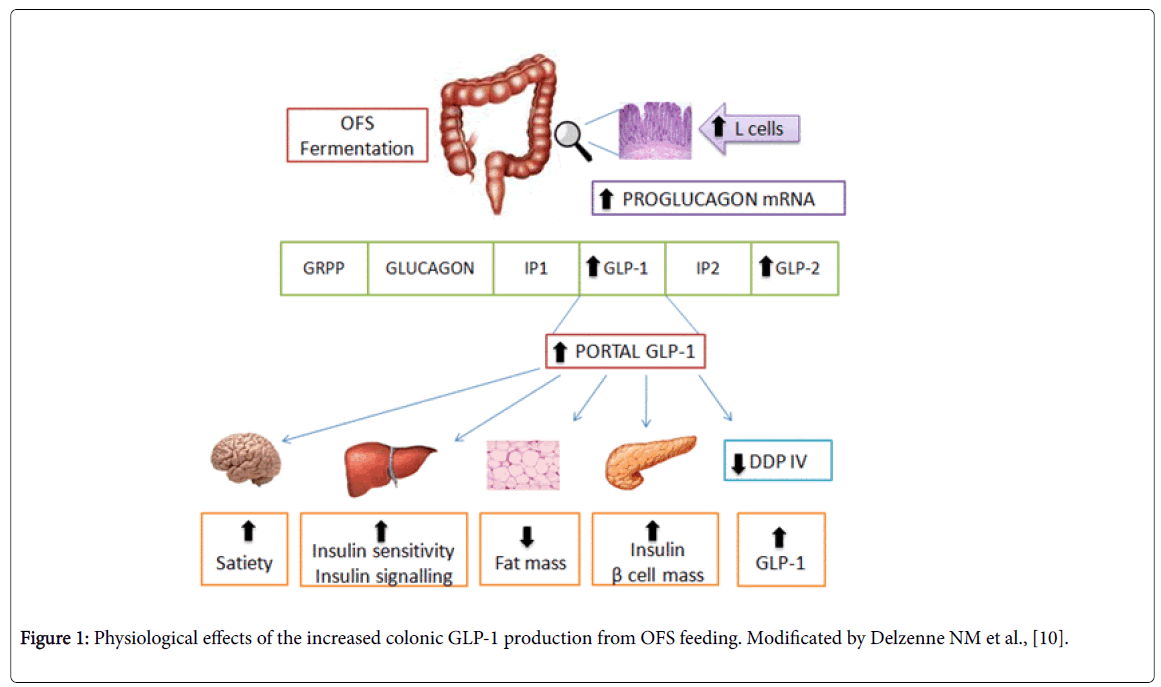
Figure 1: Physiological effects of the increased colonic GLP-1 production from OFS feeding. Modificated by Delzenne NM et al., [10].
Preliminary evidence in animals indicates that administration of inulin extracted from chicory root favorably modifies serum lipid levels and body weight due to their content of fructo-oligosaccharides (FOS) [11]. The FOS from the chicory root contain fructose polymer with β (2-1) glycosidic linkages, unlike FOS from agave inulin containing principally β (2-1) linkages, but also some β (2-6), highly ramified, and with terminal or internal glucose [12] with a probable higher hypolipidemic effect.
An open clinical trial was carried out by non-probability consecutive sampling in 30 dyslipidemic, overweight and obese subjects of both genders between 30 and 70 years old. Pregnant or lactating women as well as participants taking any drug with an effect on the metabolic profile or insulin were excluded from the study. Study subjects were classified as dyslipidemic according to the adult treatment panel III (ATP III) guidelines and the cut-off values considered to determine dyslipidemia were: [HDL-c (men <40 mg/dl; women <50 mg/dl); hypertriglyceridemia (≥ 150 mg/dl), hypercholesterolemia (≥ 200 mg/dl), LDL cholesterol (≥ 100 mg/dl)], overweight or grade I-II obesity by body mass index (BMI) [calculated as body weight (kg)/height (m2)] and according to the World Health Organization classification as: (18.5-24.9 (normal), 25.0-29.9 (overweight), 30.0-39.9 obesity grade I and II). Blood pressure was determined according to the Joint National Committee categories for systolic blood pressure: Normal blood pressure values for systolic blood pressure: (SBP) <120 and diastolic blood pressure (DBP) <80 mmHg, for normal-high blood pressure (prehypertension): SBP ≥ 120 to ≤ 139 and DBP ≥ 80 to ≤ 89 mmHg, and for hypertension: SBP ≥ 140 y DBP de ≥ 90 mmHg [13,14]. To determine IR we used the triglyceride/glucose index (TyG) [(Ln TG (mg/dl) × FG (mg/dl))/2] as a surrogate measure that has high sensitivity and specificity to recognize IR [15], and HOMA-IR (glucose x insulin)/22.5.
Due to the known adverse gastrointestinal events (abdominal pain, diarrhea, bloating, flatulence and rumbling) by pre-biotics [16], the gradual administration of these fibers increases their safety and tolerance. For this reason, the pharmacological administration of agave inulin powder was dissolved in any beverage or food (standard diet) and divided in two parts. The first part consisted of a gradual threeweek forced-titration of 5 g per day of agave inulin powder during the first week, 10 g for the second week and 15 g for the third week. The second part involved the administration of 15 g per day of agave inulin powder during 60 days. Inulin was obtained by certified process from the Tequila industry “Foundation Jalisco Produce” and the agave process was provided by the company “El Triufo de Milpillas SPR de R.L”. All volunteers maintained a stable body weight during 3 months before the study with an isocaloric diet containing approximately 250 g/d of carbohydrates 3 days before the test and study subjects were required to avoid exercise at least 72 h before the study; none of participants received changes in nutritional habits and all patients were monitored for the presence of adverse events throughout the study.
The study protocol was reviewed and approved by the local ethics committee of the University of Guadalajara, and written informed consent was obtained from all volunteers. Subjects were selected from the metropolitan area of Guadalajara, Jalisco, Mexico living in the same residential area and of similar socioeconomic status. The study was performed at 8:00 A.M. after a 10-12 hour overnight fast. For all participants, a clinical history was performed using the following determinations: height and weight were recorded with the subjects wearing light clothing without shoes (TANITA TBF 300A® scale, Arlington Heights, Il). The waist circumference was measured at its smallest point with a relaxed abdomen and hip measurement was taken from the widest point. For both measurements we used a flexible tape measure,the waist/hip ratio (WHR) was calculated as waist measurement divided by hip measurement, systolic blood pressure systolic (SBP), diastolic blood pressure (DBP) and heart rate (HR), were recorded simultaneously using a fully automated device (OMRON HEM-781INT), followed by laboratory tests in blood samples to determine serum glucose using the glucose-oxidase technique (Boehringer Mannheim GmbH, Mannheim, Germany), with an intra- and interassay coefficient of variation of <3%. For determination of HbA1c levels, ion-exchange high-performance liquid chromatography was carried out (Bio-Rad Laboratories, Hercules, CA) with an intraassay coefficient of variation of 2.8% and 3.5% and inter assay coefficient of variation of <3.0%. Creatinine and lipid profile (TC, HDL-c, TG) were measured enzymatically (Ortho-Clinical Diagnostics, Johnson & Johnson Company, Rochester, NY, USA) with an intra- and interassay coefficient of variation of <2%, LDL cholesterol (LDL-c) was estimated by the Friedewald formula (LDLc= TC-HDL-c-TG/5) and VLDL cholesterol (VLDL-c) with the TG/5 equation. Insulin concentrations were measured using the microparticle enzyme immunoassay method (Abbott Diagnostics Division, Japan Co. Ltd.) with an intra- andinterassay coefficient of variation of 3.3 and 3.8%, respectively.
Statistical analysis
Sample size was calculated by mean of a formula for clinical trials [17] with a statistical confidence of 95%, statistical power of 80%, SD for TC of 30.5 mg/dl [18], and an expected difference of at least one SD of TC into the group, obtaining a total of 15 patients that included 20% of expected loss. Data are expressed as mean ± standard deviation (SD) for quantitative variables and frequencies for qualitative variables. The inference analysis was performed with Chi-squared test. Intra-group differences were tested with the Wilcoxon signed-rank test. Data were analyzed with SPSS-20.0 software (SPSS Inc. Chicago, IL) and a pvalue ≤ 0.05 was considered statistically significant.
The selection and screening of patients with the opportunity to meet the inclusion criteria was conducted, thirty patients were recruited for this study as shown in Figure 2, of which 73.3% (n=22) were female and 26.7% (n=8) were male and the average age was 55.3 ± 8.4 years. Statistical analyses revealed no significant differences with anthropometric parameters and clinical measurements (Table 1). However, we did find statistical differences for the following parameters: fasting glucose (83.1 ± 13.4 vs. 76.5 ± 12.6 mg/dl; p=0.006), triglycerides and glucose (TyG) index (3.9 ± 0.1 vs. 3.8 ± 0.2; p=0.021), sodium (139.3 ± 3.0 vs. 140.4 ± 2.1 meqL; p=0.043) and urea (31.4 ± 8.6 vs. 26.3 ± 5.4 mg/dl; p=0.001). In addition, a trend for increased insulin concentrations (10.6 ± 4.5 vs. 13.1 ± 7.0 uUmmoL; p=0.057) (Table 2) was also found.
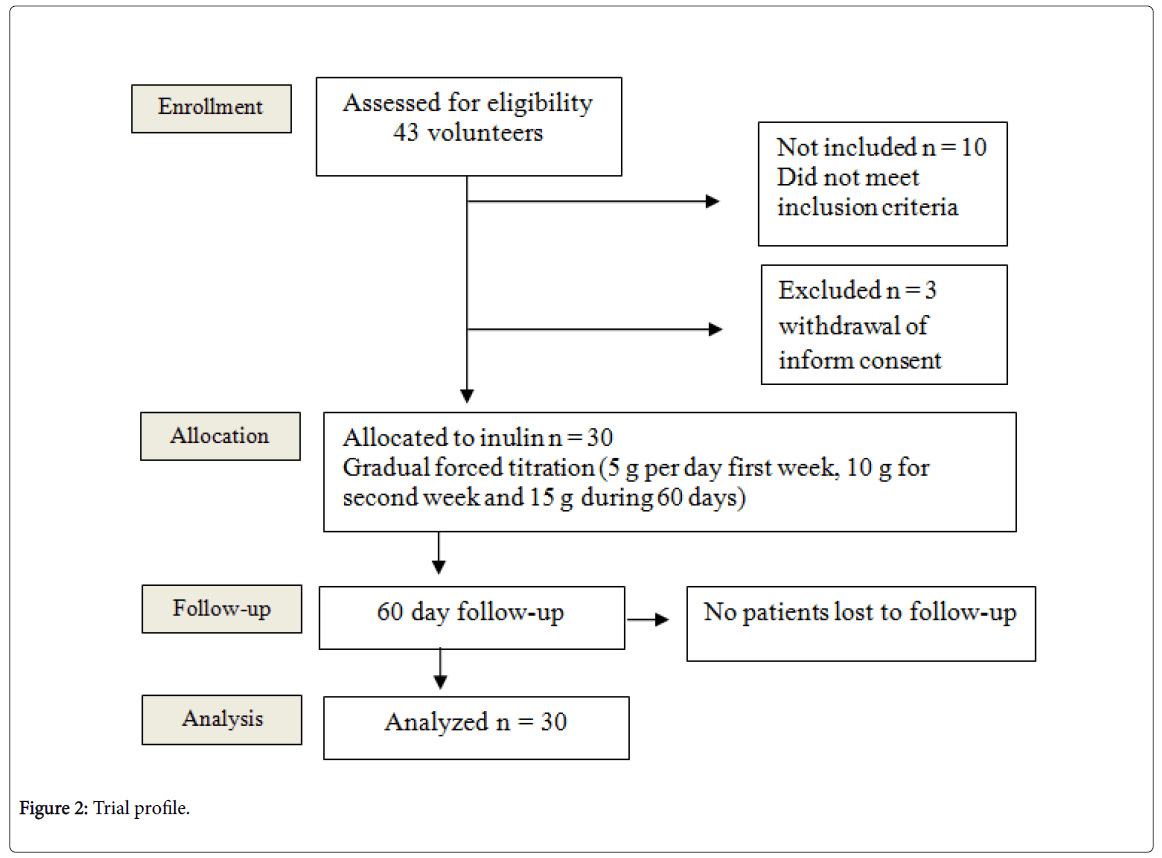
Figure 2: Trial profile.
| Before (n=30) | After (n=30) | p | |
|---|---|---|---|
| Weight (kg) | 78.6 ± 11.2 | 77.9 ± 11.3 | 0.13 |
| BMI (kg/m2) | 30.8 ± 3.8 | 30.5 ± 4.9 | 0.133 |
| Waist (cm) | 99.6 ± 10.6 | 98.4 ± 9.7 | 0.124 |
| Hip (cm) | 109.6 ± 11.5 | 109.2 ± 11.3 | 0.602 |
| Waist/hip ratio | 0.9 ± 0.05 | 0.9 ± 0.05 | 0.71 |
| BPS (mm/Hg) | 121.4 ± 14.8 | 121.3 ± 17.3 | 0.713 |
| BPD (mm/Hg) | 78.7 ± 11.4 | 78.3 ± 11 | 0.418 |
| HR (bpm) | 69.8 ± 8.2 | 69.7 ± 9.4 | 0.853 |
Table 1: The effect of agave inulin on anthropometric and clinical determinations. Patient parameters (means ± SD) at baseline and after 60 days of the intervention. BMI: body mass index; BPS: blood pressure systolic; BPD: blood pressure diastolic; HR: heart rate. All intragroup measurement has a p ≥ 0.05.
| Before (n=30) | After (n=30) | P | |
|---|---|---|---|
| Glucose (mg/dl) | 83.1 ± 13.4 | 76.5 ± 12.6 | -0.006* |
| HbA1c (%) | 5.8 ± 0.4 | 5.7 ± 0.3 | 0.189 |
| Urea (mg/dl) | 31.4 ± 8.6 | 26.3 ± 5.4 | -0.001* |
| Creatinine (mg/dl) | 0.87 ± 0.17 | 0.83 ± 0.17 | 0.263 |
| HDL-cholesterol (mg/dl) | 52.9 ± 9.2 | 53.5 ± 13.5 | 0.69 |
| LDL-cholesterol (mg/dl) | 122.5 ± 40.6 | 125.7 ± 32.6 | 0.285 |
| VLDL (mg/dl) | 38.3 ± 14.6 | 36.6 ± 16.3 | 0.465 |
| Cholesterol total (mg/dl) | 213.7 ± 37.5 | 215.9 ± 34.6 | 0.382 |
| Triglycerides (mg/dl) | 194.3 ± 70.8 | 183.1 ± 81.6 | 0.323 |
| Insulin (uUmmol) | 10.6 ± 4.5 | 13.1 ± 7 | 0.057 |
| HOMA-IR | 2.2 ± 1 | 2.5 ± 1.6 | 0.221 |
| TyGindex | 3.9 ± 0.1 | 3.8 ± 0.2 | -0.021* |
| Sodium (meql) | 139.3 ± 3 | 140.4 ± 2.1 | -0.043* |
| Potassium (meql) | 4 ± 0.4 | 4.2 ± 0.4 | 0.059 |
Table 2: The effect agave inulin on laboratory determinations in study patients. Patient parameters (means ± SD) at baseline and after 60 days of the intervention. HDL: High-density lipoprotein; LDL: low-density lipoprotein; VLDL: very low-density lipoprotein, TyG index=[(Ln TG (mg/dl) × FG (mg/dl))/2]. *p<0.05.
By analyzing differences between the basal and final results, a significant decrease in glucose levels was confirmed in 21/30 (70%) of all cases with an average reduction of -12.2 mg/dl (-41.0 to 1.0 mg/dl) and a percent difference of -13.7 (-40.6 /-1.4) p=0.006. On the other hand, in 19 cases (63.3%), the glycosylated hemoglobin was reduced by -0.4% (-0.9 to -0.1%). In addition, the TyG index was reduced significantly-0.16 (-0.34 to -0.01) with a percent difference of -4.14 (-8.36 to -0.27) p=0.021.
Similarly, in 37% of all cases, TC serum concentration was reduced -35.5 mg/dl (-105 to -1 mg/dl) without a significant decrease and a percent difference of -14.3 (-36.0 to -0.4). In reference to LDL-c, in 23% of all cases, there was a reduction of 33.0 mg/dl (-97.0 a -3.0 mg/dl) with a percent difference of -21.6 (-55.3 to -1.8) and for TG, 53% of all cases showed a reduction of -55.6 mg/dl (-150.0 to -7.0 mg/dl) and a percent difference of -26.5 (-50.0 to -5.0) (Figure 3). We must point out that in 19/30 patients (63%) we found increased HDL-c levels by 9.0 mg/dl (1.0-20.0 mg/dl) with a percent difference of 19.0 (2.0-37.0), p=0.690. We did not observe significant differences in weight 1.6 kg (-7.7 a -0.1 kg) with a percent difference of -2.1 (-8 a -0.1) p=0.130, after an 8-week administration of 15 g of agave inulin blue variety.
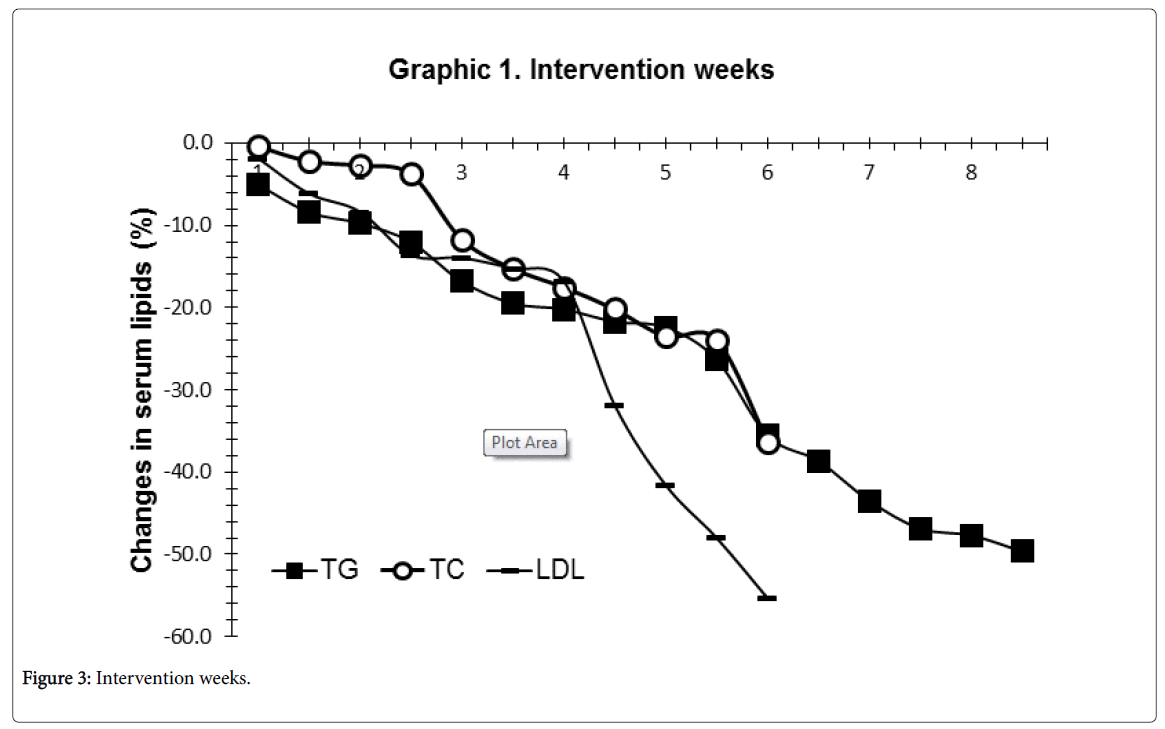
Figure 3: Intervention weeks.
Finally, by analyzing the percentages of our study group regarding the diagnostic models for this study (hypertriglyceridemia, hypercholesterolemia, combined dyslipidemia, overweight, obesity grade I- II and prehypertension) before and after the intervention, we found that 16.7% (p=0.025) of patients showed normal blood lipid levels, reversing the diagnosis of hypercholesterolemia by 6.7% (p=0.042), 13.3% showed hypertriglyceridemia (p=0.003), and 6.6% had a combined dyslipidemia (p=0.043). Furthermore, 23.3% (p=0.008) of pre-hypertensive patients normalized their blood pressure levels (Table 3). It is noteworthy that the analysis in terms of the percentage difference refers only to the patients who had a reduction in lipid levels; also, the benefit was greater in those with combined dyslipidemia.
| % (n) basal | % (n) final | p | |
|---|---|---|---|
| Normal lipids | 0 (0) | 16.7 (5) | 0.025* |
| Hypercholesterolemia | 70.0 (21) | 63.3 (19) | 0.042* |
| Hypertriglyceridemia | 73.3 (22) | 60.0 (18) | 0.003** |
| Combined Dyslipidemia | 46.6 (14) | 40.0 (12) | 0.043* |
| Normal weight | 0 (0) | 6.6 (2) | 0.157 |
| Overweight | 46.7 (14) | 50.0 (15) | 0.317 |
| Obesity | 53.3 (16) | 43.3 (13) | 0.317 |
| Normotensive | 33.3 (10) | 56.7 (17) | 0.008** |
| Prehypertension | 66.6 (20) | 43.3 (13) | 0.008** |
Table 3: Percentage comparison of clinical diagnoses. Values expressed in frequencies. *p<0.05, **p<0.01.
In relation to adverse reactions, only two patients reported slight gastrointestinal problems (diarrhea and abdominal distention) that could be associated with a low fiber consumption diet, but in general all fiber supplementation was well tolerated by all patients and no patients failed to complete the study due to adverse reactions.
The controversy over the effect of using derivatives inulin fructans has remained dormant for at least one decade. Functions of inulin fructans have been linked to changes that enhance the metabolic status of patients including weight loss, reduced blood lipid levels and serum glucose and even a possible reduced cardiovascular risk. In this study, the addition of agave inulin was aimed to evaluate the metabolic profile and risk factors in dyslipidemic patients with an overweight and obesity diagnosis.
A reduction in fasting glucose levels was found at the end of the intervention and is consistent with previous studies that have sustained that the supplementation with agave fructans induces a higher concentration of GLP-1 and its precursor, proglucagon mRNA in the different colonic segments which are able to promote the production of satietogenic/incretin peptides in the lower part of the gut, with promising effects on glucose metabolism. On the otherhand, the main function of peptides GLP-1 and GIP is the stimulation of post-prandial secretion of insulin by pancreatic β-cells, mechanism that could explain the association of fructans with the slight increase of insulin levels in our patients [10].
The aim of our study was to substantiate the effect of agave fructans on the serum lipid profile and weight loss in overweight and obese patients with dyslipidemia, based on previous reports with other fructans which demonstrated increased satiety by regulating the secretion of gastrointestinal hormones like glucagon-like peptide-1 and glucagon-like peptide-2 and decreasing the level of ghrelin, and thus, an active participation in reducing serum lipids. This reduction has been attributed to a decrease in the gene expression of hepatic enzymes responsible for de novo synthesis of lipids, increased muscle lipoprotein lipase (LPL) enzyme activity; as well as by the increased population of Bifidobacteria and the production of short chain fatty acid (SCFA); butyrate which stimulates the differentiation of crypt cells in enteroendocrine L cells, increasing the production of fatty acid synthase, LPL, SCFA [19].
Several works have studied the effects of prebiotics, however, results are controversial; in some studies there was no reported effect on the serum reduction of TC, TG and LDL cholesterol, nonetheless in others of them a significant reduction was found: 12.7% for TC and two studies reported a 16.4% reduction for TG and 16.2% for LDL-c. In a study with inulin, a significant reduction in TG, TC, LDL-c and VLDLc serum levels was observed following a 4-week ingestion of 7 g of inulin powder previously dissolved in juice, milk or water [20].
Patients in our study group did not show a significant difference in weight and satiety was not evaluated, so possibly a greater and specific diet control was necessary. However, our interest in not controlling the diet and therefore achieve weight loss, was avoid attributing changes in serum lipids to weight loss. We must also point out that other reports with significant modifications in serum lipids have evaluated patients with severe dyslipidemia more so than with patients with mild to moderate dyslipidemia.
However, the significant percentage reduction we observed in our study, 14.3% for TC, 26.5% for TG and 21.6% for LDL-c, considering this last variable as the most atherogenic and of clinical importance, could be partly attributed to observations by Delzenne [20], considering that if the intrahepatic lipolysis mechanism is not activated with fiber consumption as the activity of the enzyme carnitinepalmitoyltransferase is not altered, an increase in lipid catabolism by the extrahepatic pathway with agave inulin consumption is observed.
Several indirect methods have been incorporated that allow IR estimation. Recently, a new surrogate formula was proposed for estimating IR from triglycerides (TG) and fasting glucose (FG), referred to as the triglyceride/glucose (TyG) index based on the product of the natural logarithm between TG and FG divided by 2, whose formula is TyG=[(Ln TG (mg/dl) × FG (mg/dl))/2], this formula was validated against the HOMA-IR index and the euglycemic-hyperinsulinemic clamp [15]. Furthermore, by evaluating IR, the HOMA-IR index and the TyG index in our study population, we found differences between baseline and final values for the TyG index. These differences could be related to lipoprotein metabolic alterations commonly present in overweight and obese individuals and thus increase lipid serum levels which interfere with muscle glucose metabolism and are in accordance with the hypothesis that the elevation of triglycerides reduces insulin sensitivity. The TyG index measures the triglycerides/glucose [15] product and by decreasing triglycerides with the intervention of inulin, we could interpret that agave fructans improve or enhance IR.
Several studies [21-24] have shown modifications starting at three weeks of consuming products with added probiotics, prebiotics and phytosterols, therefore the intervention period for this study was considered adequate. Longer intervention periods are required to observe changes in colonic fermentation and its effects on weight reduction and cardiovascular risk. As a weakness of our study, a larger sample is required to confirm the dose-effect relationship where a slight tendency to improve TC, TG and LDL-c, with slight increase in HDL-C, and a comparison with the placebo control group was shown.
Moreover, it has been suggested that adding fiber to the diet increases the risk of diarrhea, and thus a decrease in the concentration of electrolytes. However, in patients included in this study we did not observe reduction of these electrolytes by the end of the study. On the contrary, sodium was increased significantly, there is no precise explanation behind this effect, but previous publications describe the large intestine is the best absorption site to various molecules [25], which could be modified by changes in the gut microbiota.
This research is considered pioneer in the study of the effects by agave inulin blue variety on the lipid profile of overweight and obese dyslipidemic patients. Agave tequilana Weber blue variety, produced in our country and characterized by its FOS content, originally proposed as functional food ingredients capable of improving parameters of the metabolic syndrome, blood glucose concentration and lipid metabolism, more recently, it has been hypothesized that agave inulin may have an impact on body weight, possibly by modulation of gastrointestinal hormones [26], although requires further research we believe that it can contribute to improve the health of many patients due to its low cost and inclusive, favor the development of the agave industry.
The use of inulin-type Agave tequilana Weber blue variety in a dose regimen of 15 mg for 60 days in subjects with dyslipidemia diagnosed as overweight and obese significantly reduced fasting glucose as well as the TyG index In addition, this agave inulin was effective in reducing the percentage difference of TC, TG and LDL-c blood levels without a significant change in body weight.
The authors declare no competing interests with any of the mentioned pharmaceutical companies. Financial support was provided by the Instituto de Terapéutica Experimental y Clínica (INTEC), Departamento de Fisiología, Centro Universitario de Ciencias de la Salud, Universidad de Guadalajara, Guadalajara, Jalisco, México.