Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Short Communication - (2016) Volume 6, Issue 2
Keywords: Endobronchial ultrasound; Transbronchial needle aspiration
The advent of convex-probe endobronchial ultrasound (CP-EBUS) technology at the beginning of the 21st century dramatically changed the world of bronchoscopy. EBUS-guided transbronchial needle aspiration (EBUS-TBNA) has rapidly become the cornerstone for staging lung cancer and for the diagnosis of mediastinal and hilar lymphadenopathies. The first clinical trial on EBUS-TBNA was published approximately a decade ago, and since then, the body of literature has grown exponentially [1]. In this article after a brief historical review of TBNA, we assess the evolution of the body of literature on EBUS-TBNA, the current status of this technique, and its future directions.
In 1949, Dr. Eduardo Schieppati published the first report of TBNA in “Revista de la Asociacion Medica Argentina” (Journal of the Argentinean Medical Association) [2]. Unfortunately, this data did not make it to the English literature until a decade later [3]. His original work involved the use of a rigid needle passed through the rigid bronchoscope which allowed sampling of large subcarinal and paratracheal masses with a high diagnostic yield. TBNA was reintroduced in the era of flexible bronchoscopy by Dr. Ko Pen Wang, who introduced the use of a flexible needle in the early 1980’s. In experienced hands conventional TBNA proved to be an accurate means of diagnosing mediastinal and hilar lymphadenopathies [4] and this became the standard technique for TBNA over the next two decades. The main limitation of conventional TBNA was that the estimation of the needle entry point into the airway wall was based on pre-procedure evaluation of static computed tomography (CT) images and a survey by Dasgupta and Mehta showed that this technique was profoundly underutilized, probably due to its wide-ranging diagnostic yield [5]. In the late 1990’s Dr. Heinrich Becker and Dr. Felix Herth described the use of radial-probe EBUS, which allowed bronchoscopists to visualize lymph nodes or masses through the airway wall in order to more precisely select the needle entry point [6,7]. The limitation of this technique was that the catheter-based ultrasound probe had to be removed from the working channel in order to deploy the needle used for sampling. Convex Probe EBUS on the other hand integrated the ultrasound transducer into the bronchoscope itself, allowing for needle deployment through the working channel without loss of the ultrasound image. In 2004, the initial clinical trial describing CP-EBUS was published by Dr. Kazuhiro Yasufuku [1] and, for the first time, bronchoscopists could utilize real-time ultrasound images that allowed for simultaneous visualization of the needle and its target. The remaining of this article refers exclusively to CP-EBUS.
In order to review the evolution of the body of literature of EBUSTBNA over the last decade, we performed a search in PubMed with the term “endobronchial ultrasound” from January 1st 2005 to December 31st 2014. We analyzed all publications that referred exclusively to CPEBUS- TBNA in the English literature. As shown in Figure 1, the number of publications grew rapidly, reaching a total of 878 per our analysis. Not surprisingly, publications on EBUS were mostly focused on three diseases: lung cancer, sarcoidosis, and lymphoma. There is a clear predominance of literature on EBUS and lung cancer, and this trend has remained stable throughout the years (Figure 2).
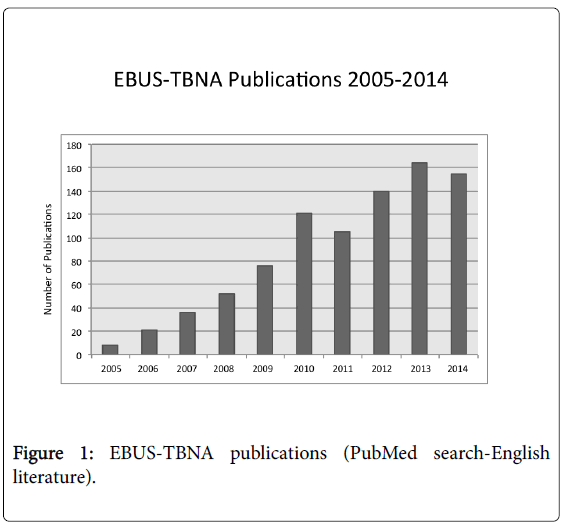
Figure 1: EBUS-TBNA publications (PubMed search-English literature).
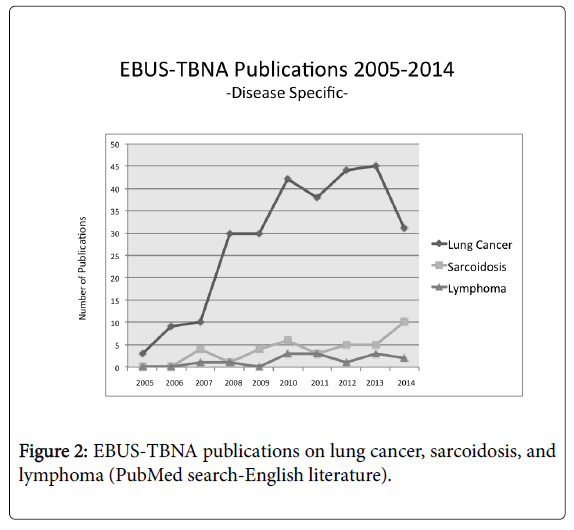
Figure 2: EBUS-TBNA publications on lung cancer, sarcoidosis, and lymphoma (PubMed search-English literature).
We divided publications in three groups: “effectiveness”, “technical aspects”, and “education”. We considered “effectiveness” studies to be those that focused on the yield of EBUS for diagnostic or staging purposes. The “technical aspects” group included those studies evaluating the influence of technical factors on the success of the procedure. These included such things as the number of passes, needle size and type, use of forceps, use of suction, on-site cytology, cytology techniques, techniques for molecular markers, type of sedation, and scope insertion route, and others. The “education” group involved studies on the learning curve for EBUS as well as different learning and evaluation strategies (i.e. virtual simulators, wet-lab, EBUS-STAT). As shown in Figure 3, during the initial five years most publications belonged to the “effectiveness” group, with an inflection point around 2009 after which there was a rapid increase in the number of publications from the other two groups and a plateau followed by a decline in the number of publications from the “effectiveness” group. We might therefore describe two phases over the last decade of research on EBUS-TBNA. In the initial phase (2005-2009) the scientific community evaluated the effectiveness of EBUS-TBNA for diagnosis of mediastinal and hilar lymphadenopathies and for lung cancer staging. Once EBUS-TBNA’s effectiveness was proven and widely accepted, a second phase followed (2010-2014) in which scientists focused on technical aspects that could potentially influence the yield of EBUS-TBNA as well as on different educational strategies. While the “effectiveness” group comprised 80% or more of the publications during the initial phase, it made up less than 50% of articles in the second phase. More recently, in the last two years the proportion of articles from the “effectiveness group” has even been less than 20%, with the remaining two groups clearly dominating the field (Figure 4).
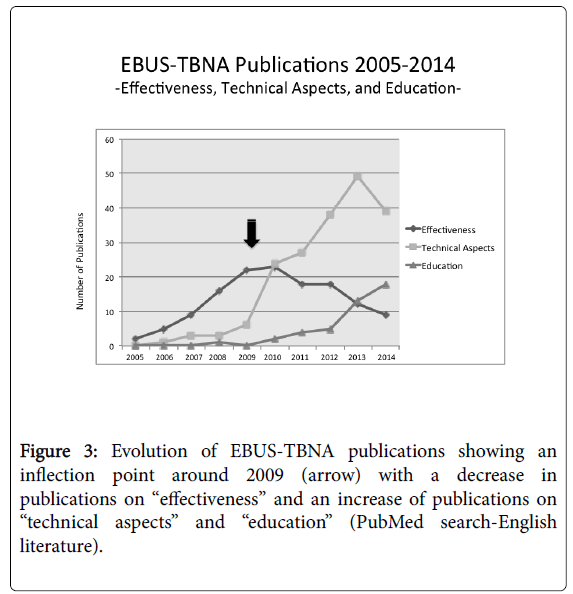
Figure 3: Evolution of EBUS-TBNA publications showing an inflection point around 2009 (arrow) with a decrease in publications on “effectiveness” and an increase of publications on “technical aspects” and “education” (PubMed search-English literature).
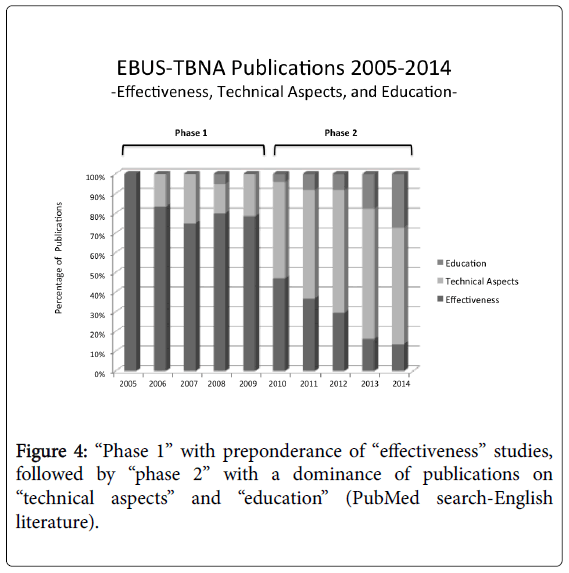
Figure 4: “Phase 1” with preponderance of “effectiveness” studies, followed by “phase 2” with a dominance of publications on “technical aspects” and “education” (PubMed search-English literature).
In order to globally ascertain the quality of the available literature over this past decade, we further divided publications into 6 major groups: clinical trials, retrospective studies, meta-analysis, case reports, review articles, and clinical guidelines. Clinical trials included prospective studies (with prospective enrollment of patients) regardless their sample size and the presence or absence of randomization. Other publication types such as editorials, letters to the editors, and errata were not included in this analysis (6 major groups described above) despite their relatively large number. Unfortunately, the vast majority of EBUS literature is comprised of retrospective studies, case reports and review articles (Figure 5). While there has been a steady increase in the number of clinical trials, retrospective studies and case reports continue to be the predominant form of publication (Figure 6). In addition, most studies grouped under clinical trial category in our analysis were non-randomized and had a relatively small sample-size. Nevertheless, the rapidly growing body of literature has led to the publication of a few meta-analyses as well as the first set of clinical guidelines developed by the WABIP in 2014 [8]. While outside of the period we analyzed, we cannot fail to mention a second set of guidelines more recently published by the ACCP in 2015 [9].
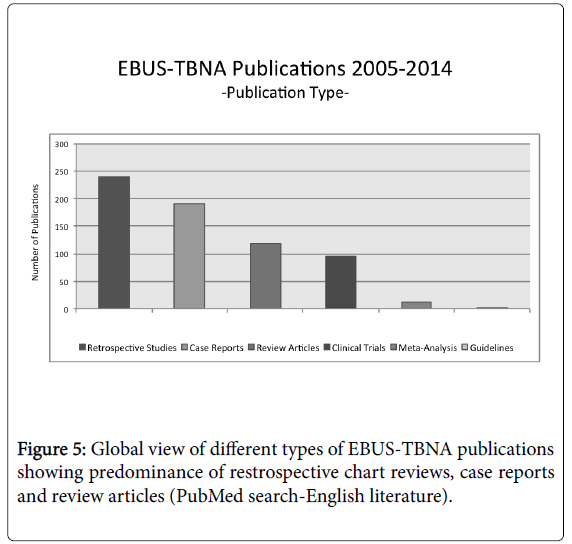
Figure 5: Global view of different types of EBUS-TBNA publications showing predominance of restrospective chart reviews, case reports and review articles (PubMed search-English literature).
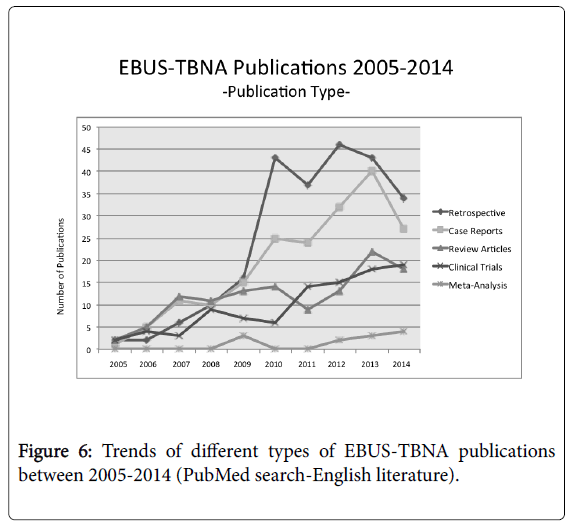
Figure 6: Trends of different types of EBUS-TBNA publications between 2005-2014 (PubMed search-English literature).
Supported by the large body of evidence described above, EBUSTBNA is now a well-established and mature technique. It has had a marked impact on mediastinal staging of lung cancer, where it has been shown to provide greater sensitivity and specificity than imaging modalities and to be as effective as mediastinoscopy with a more favorable safety profile [10-14]. This impact is reflected in the most recent lung cancer guidelines, which now recommend a needletechnique such as EBUS-TBNA as initial method of choice for sampling of the mediastinum [15,16]. Multiple prospective trials have shown EBUS-TBNA to be superior to “conventional” TBNA for the diagnosis of stages I-II of sarcoidosis [17-19]. Although the data of EBUS-TBNA for lymphoma is less robust, it is still suggested as the initial diagnostic tool due to its favorable safety profile with negative results requiring corroboration with surgical techniques [20-22]. Despite being pioneered by interventional pulmonogists, it is not surprising then that EBUS-TBNA is now being taught to most pulmonary fellows during their basic training [23].
The recent advent of clinical guidelines has helped us identify areas where better quality evidence is needed and research should be directed in the future. The need for the bronchoscopy community to work together in a more organized fashion to develop multicenter clinical trials has become more urgent. The potential lack of generalizability of the results of some well-designed studies resides on the fact that they were typically conducted in one or few institutions by highly experienced operators. With the exponential spread of this technique, it is therefore imperative to focus future work on establishing appropriate EBUS teaching curricula and developing quality metrics for proficiency testing. Although the bar has been set high, advances in technology that attempt to improve the performance of this technique even further should not cease. Needle modifications, reduced scope diameter, and added features such as elastography (measure of tissue compressibility) may prove beneficial in the near future.
We live in an era of precision medicine and individualized therapy for lung cancer and a rapid expansion in our knowledge of the genetic and immunologic basis of this disease. It is time for us to look “beyond the microscope” and partner with our scientific colleagues in different translational research efforts that could leverage these exciting new discoveries. EBUS-TBNA can obtain adequate material for genetic analysis, and provides safe and convenient access to the local immune system “stations”, the lymph nodes.
In summary, endobronchial ultrasound has become one of the most valuable tools for bronchoscopists, and our scientific community has proven this with a myriad of publications in this past decade. We consider ourselves fortunate to have been part of this revolution in the field of bronchoscopy, but our job is by no means over. This is only an exciting start.
Roberto F Casal has received research grants from Spiration and he is a consultant for Olympus America Inc.
Kazuhiro Yasufuku has received educational and research grants from Olympus Medical Systems Corp., and he is a consultant for Olympus America Inc., Intuitive Surgical Inc., Covidien, and Johnson and Johnson.