Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2014) Volume 4, Issue 5
Background: There is uncertainty about the prevalence of viral respiratory tract infections in intensive care unit (ICU) patients, and whether these infections contribute to disease severity and final outcome. Furthermore, the pattern of viral shedding during influenza infections in critically ill patients is largely unknown. Objectives: This study will assess prevalence of viral respiratory tract infections in intubated and ventilated ICU patients. Secondary objectives are to assess risk factors for and burden of viral respiratory tract infections, to describe the proportion of these infections missed in routine care, and to describe viral shedding patterns during influenza infection. Design: This is an investigator–initiated national multicenter prospective observational study conducted during one influenza season. Consecutive intubated and ventilated adult critically ill patients are included, regardless of admission diagnosis. Nasopharyngeal swabs and tracheobronchial aspirates are collected daily till patients are weaned of mechanical ventilation. Samples will be tested using multiplex real–time polymerase chain reaction (RT–PCR) for respiratory viruses. In influenza–positive patients, subsequent daily samples will be tested for influenza via RT–PCR until viral clearance. Influenza RT–PCR positive samples will be cultured and influenza subtyping will be performed. The primary endpoint is prevalence of viral respiratory tract infections in ICU patients. Discussion: COURSE will provide insight into the prevalence of, risk factors for, burden of and shedding patterns in viral respiratory tract infections in intubated and ventilated ICU patients during one winter season in the Netherlands. It is the largest prospective observational study thus far, with simultaneous sampling of both upper and lower respiratory tract of consecutive acutely admitted intubated and ventilated ICU patients, regardless of the admission diagnosis. Results of COURSE may guide future allocation and methods of viral diagnostic testing, quarantine practices, and duration of treatment with anti–viral drugs in ICU patients.
Keywords: Respiratory virus, Viral infection, Prevalence, Epidemiology, Risk factors, Burden, Viral shedding, Airway sampling, Intensive care unit, Critically Ill patients, Study protocol, Multicenter prospective Observational study
APACHE: Acute Physiology and Chronic Health Evaluation; ARF: Acute Respiratory Failure; BAL: Broncho Alveolar Lavage; CAP: Community Acquired Pneumonia; CRP: C–Reactive Protein; DTT: Dithiothreitol; HCAP: Health Care-Associated Pneumonia; ICU: Intensive Care Unit; NP: Nasopharyngeal; RTPCR: Real–Time Polymerase Chain Reaction; SAPS: Simplified Acute Physiology Score; SOFA: Sequential Organ Failure Assessment; TA: Tracheal (Bronchial) Aspirate
Recent experiences with ‘Middle East Respiratory Syndrome’ coronavirus and the influenza A (H7N9) and (H1N1) viruses forcefully remind us of the potential causative role of respiratory viruses in severe pneumonia. While influenza is recognized as one of the most prominent viruses associated with severe community–acquired pneumonia [1-3] with an yearly estimated 250.000 to 500.000 deaths due to seasonal influenza [4], there remains a paucity of knowledge regarding epidemiology and burden of infections with other respiratory viruses, especially in intubated and mechanically ventilated Intensive Care Unit (ICU) patients.
Only a handful studies reported on the prevalence of viral respiratory tract infections in ICU patients, which ranged from 9% to as high as 36% in patients admitted with acute respiratory failure and/or a suspected respiratory infection (Table 1) [5-11]. Furthermore, studies on the burden of viral respiratory tract infections in critically ill patients, show conflicting results in associations between the presence of a respiratory tract infection due to a virus and the clinical outcome [5,6,8,10,12]. Also, there is limited data on how and how long ICU patients with influenza infections shed viruses. Consequently guidelines on quarantine of these patients are sparse and at times conflicting.
| author [ref] | admission diagnosis | N | sample site | virus-positive (%)* | influenza virus (%) | parainfluenza virus (%) | adenovirus (%) | respiratory syncytial virus (%) | coronavirus (%) | rhinovirus (%) | enterovirus (%) | metapneumovirus (%) | bocavirus (%) | cytomegalovirus (%) | herpes simplex virus (%) | varicella zoster virus (%) | comments |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Carrat, [5] |
ARF | 122 | nose | 17 | 7 | - | - | 5 | 1 | 3 | - | 2 | - | - | - | - | no inclusions during weekend |
| Daubin [6] |
ARF | 187 | lung | 22 | 4 | 1 | 1 | 1 | 1 | 10 | 1 | 0 | - | 1 | 5 | 1 | virus detection method differed between samples |
| Cillóniz [7] |
CAP | 362 | nose and/or lung | 9 | ? | ? | ? | ? | ? | ? | ? | - | - | - | - | - | nose samples obtained in 50%, BAL in 23% of patients |
| Choi [8] |
CAP or HAP | 198 | nose and/or lung | 36 | 6 | 8 | 1 | 5 | 2 | 9 | 1 | 7 | 0 | 4 | - | - | nose samples obtained in 69%, BAL in 49% of patients |
| Wiemken[9] | CAP | 393 | nose | 23 | 10 | ? | ? | ? | - | 8 | - | 3 | - | - | - | - | |
| Østby [10] | CAP or HAP | 122 | throat | 16 | 8 | 0 | 1 | 2 | 2 | 1 | - | 1 | - | - | - | 25% of samples obtained after ≥ 4 days of admission | |
| Ong [11] |
ARF | 158 | nose | 18 | 15 | - | - | - | - | 4 | - | - | - | - | - | - | |
| *,a patient with an infection with more than one virus counts as 1 virus-positive patient; all causative viruses are presented; –, not tested; ?, not reported. Abbrevations: ARF, Acute Respiratory Failure; BAL, Bronchoalveolar Lavage; CAP, Community–Acquired Pneumonia; HAP: Healthcare–Associated Pneumonia | |||||||||||||||||
Table 1: Prospective observational studies reporting viral respiratory infections in adult ICU patients.
The aim of the ‘Prevalence and Clinical Outcomes of, and viral Shedding patterns during viral infections in intubated intensive care unit–patients’ study (COURSE) is to assess the prevalence of viral respiratory tract infections in acutely admitted intubated and ventilated ICU patients, regardless of the admission diagnosis. COURSE will seek for risk factors for viral respiratory tract infections. COURSE will also allow us to determine how frequent viral respiratory tract infections are missed, by comparing positive diagnostic tests obtained for COURSE and those obtained in daily routine. Also, COURSE could provide insights in the burden of viral respiratory tract infection in acutely admitted intubated and ventilated ICU patients, by determining the associated morbidity and mortality of respiratory tract infections with viruses. Finally, COURSE provides insights in viral shedding patterns of ICU patients with an influenza infection.
Study design
COURSE is a national, investigator–initiated, multi–center, prospective observational study conducted in the ICU departments of five Dutch hospitals, all serving a mixed surgical–medical population. COURSE is registered at the Dutch Trial Register (http://www. trialregister.nl), trial identification number NTR4102. CONSORT diagram in Figure 1 shows the CONSORT diagram of COURSE.
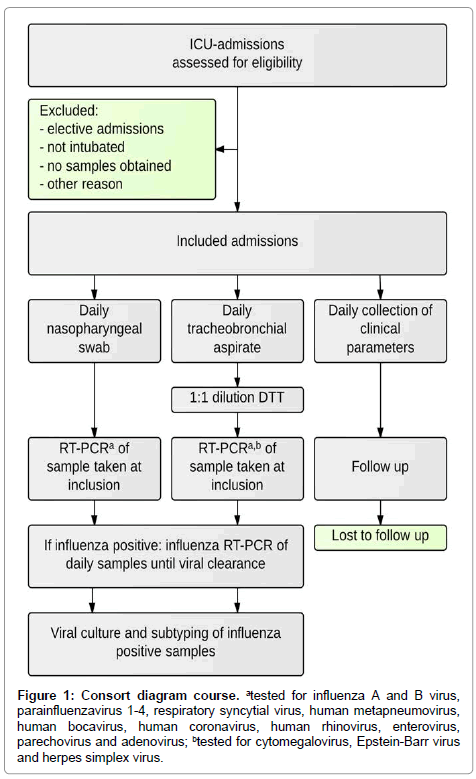
Figure 1: Consort diagram course. atested for influenza A and B virus, parainfluenzavirus 1-4, respiratory syncytial virus, human metapneumovirus, human bocavirus, human coronavirus, human rhinovirus, enterovirus, parechovirus and adenovirus; btested for cytomegalovirus, Epstein-Barr virus and herpes simplex virus.
Study population
Consecutive acutely admitted intubated and ventilated ICU patients, aged ≥ 18 years, are included regardless of admission diagnosis and reasons for intubation and ventilation. Excluded are patients whose admission to the ICU is planned (e.g., patients after elective surgery). Patients are included from September 1, 2013 until April 30, 2014, to encompass the annual influenza season in the Netherlands.
Ethical considerations
The Institutional Review Board of the participating centers approved the study protocol and provided a waiver from the Medical Research Involving Human Subjects Act in Dutch law, due to the noninvasiveness of study procedures. Patients and their legal representatives are provided with an information folder at ICU admission, and can withdraw participation from this study via the opt–out procedure.
Collection of clinical data
Baseline patient characteristics are collected on admission, and include gender, age, medical history, smoking status, alcohol status, previous medication including recent use of antibiotic or antiviral medication, microbiology test results as ordered by attending medical staff from 10 days prior to intubation, date of hospital and ICU admission, diagnosis at ICU admission and after 24 hours of ICU admission, presence of influenza–like illness prior to admission, admission type, referring specialty, the Acute Physiology and Chronic Health Evaluation (APACHE) II score and the Simplified Acute Physiology Score (SAPS) II.
Clinical and laboratory data from routine care are collected daily until successful weaning from mechanical ventilation (defined as ≥ 24 hours free from mechanical ventilation), death, or transfer to another hospital while intubated and ventilated, whatever comes first. These include ventilation characteristics, use of antibiotic and antiviral medication, microbiology test results as ordered by attending medical staff, blood leukocytes and C–reactive protein (CRP), highest and lowest body temperature, use of active cooling, chest X–ray results, Lung Injury Scores, and the Sequential Organ Failure Assessment (SOFA) scores.
The following outcome measures are collected: transfer to another hospital, the number of ventilation–free days and alive at day 28, length of ICU stay, length of hospital stay, and 28–, 90– and 180–day overall mortality.
Microbiologic procedures
Daily sampling of the nasopharynx with a flocked swab in virus transport medium (Copan Diagnostics, Brescia, Italy), and tracheobronchial aspirate in a sterile container (Medisize BV, Hillegom, the Netherlands) is performed until successful weaning from mechanical ventilation, death, or transfer to another hospital while intubated and ventilated.
Samples are transported to the laboratory of the Academic Medical Center (Amsterdam, The Netherlands) and stored at -80ºC. Tracheobronchial aspirates are diluted 1:1 with 1,54 mg/ml Dithiothreitol (DTT) prior to processing. DTT is diluted in 1:1 distilled water and DTT-buffer (100 mM NaHCO3, 50 mM Hepes, 77 mM normal saline). Nucleic extractions are performed using the Roche MagNA Pure Total Nucleic Acid Kit on a MagNA Pure 96 instrument (Roche Diagnostics, Penzberg, Germany), using 200 μL of sample.
Nasopharyngeal swabs and tracheobronchial aspirates obtained within 48 hours of intubation will be considered as samples taken at inclusion. On these samples, semi–quantitative multiplex RT–PCR will be performed with the LightCycler 480 (Roche Diagnostics, Penzberg, Germany), using a validated protocol [13] for the following targets: influenza A and B virus, parainfluenzavirus 1-4, respiratory syncytial virus, human metapneumovirus, human bocavirus, human coronavirus, human rhinovirus, enterovirus, parechovirus and adenovirus. Viral load is estimated using crossing–point values obtained by RT–PCR. In addition, tracheobronchial aspirates will be tested for cytomegalovirus, Epstein-Barr virus, and herpes simplex viruses. Follow–up samples of influenza positive patients will be tested with quantitative RT–PCR for influenza, until viral clearance (defined as at least 2 consecutive samples with crossing–point values > 40). On influenza positive samples, influenza subtyping will be performed, as well as quantitative viral culture on Madin-Darby canine kidney cells, by limiting dilution and calculation of a tissue culture infective dose of 50% using the Reed–Muench method [14].
Study endpoints
The primary endpoint of COURSE is the prevalence of viral respiratory tract infections in acutely admitted intubated and ventilated ICU patients. Secondary endpoints are (a) the proportion of viral infections that were missed by attending physicians due to not performing diagnostic tests in routine care, (b) risk factors for viral respiratory tract infections, (c) the morbidity and mortality associated with viral respiratory tract infections, and (d) qualitative and quantitative shedding patterns in influenza virus–positive ICU patients.
Sample size
COURSE is an observational study within a set period of time, without a pre–determined sample size calculation. However, based on the ICU admission rates of critically ill intubated and ventilated patients in the participating centers, COURSE is expected to include 1,300 to 1,700 patients. For the primary outcome, an expected 17 to 22% of the inclusions will be tested virus–positive, based on smaller sampling studies including ICU patients with acute respiratory failure [5,6,11].
Analysis plan
The primary endpoint, prevalence of viral infections, will be expressed in the total number of cases per total number of inclusions. It will be categorized by virus type (influenza A and B virus, parainfluenza virus 1-4, respiratory syncytial virus, human metapneumovirus, human bocavirus, human coronavirus, human rhinovirus, enterovirus, parechovirus, adenovirus, cytomegalovirus, Epstein–Barr virus, and herpes simplex virus) with their corresponding crossing-point value, by period (month), by location (hospital), and by co–infection with other viruses and/or bacteria. Baseline characteristics of virus–positive and virus–negative patients will be described. A patient is defined virus–positive if at least one sample is positive, for at least one of the viruses tested. Description of co–infection with bacteria is based on culture results as performed by routine care during ICU admission.
The secondary endpoints – to describe the proportion of virus infections that are missed by attending medical staff during ICU admission, the results obtained from virus diagnostics on samples tested in routine care will be compared to test results of samples obtained in this study.
To determine which patient factors are associated with the presence of a viral respiratory tract infection, a statistical model is used to find the most valid subset of available predictors and the corresponding best fitting regression model for describing the relationship between virus–positive patients at intubation and those relevant predictors. Pre–defined predictors for this model are patient age, medical history (including immunosuppression and medication), smoking and alcohol status, month of ICU admission, presence of influenza–like illness prior to admission, diagnosis at ICU admission, APACHE II, SAPS II and SOFA score at admission, body temperature and laboratory results at inclusion (including leukocytes and CRP) and chest X–ray results at inclusion. Further subgroup analysis will be performed, but will depend on the prevalence found for different viruses. At least 2 predefined subgroups are patients positive for herpes viridae (cytomegalovirus, Epstein–Barr virus, and herpes simplex virus), and patients positive for the other tested viruses.
We will compare outcome parameters between virus–positive and virus–negative patients. These outcome parameters include mechanical ventilator–free days and alive at day 28, the maximum SOFA score, ICU length of stay and hospital length of stay, and 28–, 90–, and 180– day mortality.
Viral shedding is quantified as the viral load per day, per sampling site (nasopharyngeal swab vs. tracheobronchial aspirate). In virus– positive patients, sensitivity of virus detection will be compared between sampling sites. Duration of influenza positivity per day will be compared between sampling site, between immunosuppressed and immune competent patients, and per assay method (RT–PCR vs. viral culture).
Continuous normally distributed variables will be expressed by their mean and standard deviation or when not normally distributed as medians and their interquartile ranges. Categorical variables will be expressed as n (%). To test groups Student’s t test will be used, if continuous data is not normally distributed the Mann–Whitney U test will be used. Categorical variables will be compared with the Chi–square test or Fisher’s exact tests. Where appropriate, statistical uncertainty will be expressed by 95% confidence levels.
For the prediction model, a multiple logistic regression model is used with forward selection (by hand) of predictors. The model is improved if adding a conceptual relevant predictor, results in a significant reduction (Chi square test) of the -2-log-likelihood. Risk factors will be pre–selected by their univariate association with the dependent variable (p<0.10). The goodness of fit of the models is expressed by the Hosmer–Lemeshow test.
For comparing mortality and ventilator free days and alive at day 28 between patients with and without a viral respiratory infection, a proportional hazard model proposed by Fine and Gray will be used [15]. Mortality and ventilator–free days at day 28 are considered competing risks. The model will include adjustment for predefined covariates. We will use a forward approach adding covariates on the basis of their significance. Model assumptions (i.e. proportional hazards) will be tested with Schoenfeld residuals.
Statistical significance is considered to be at a p–value of ≤ 0.05. Analysis of repeated measurements will be corrected for multiple testing. Statistical analysis will be computed in R, version 3.1 [16].
The rationale behind COURSE is that knowledge on viral respiratory tract infections in critically ill patients is limited in several ways: the prevalence of these infections in these patients is largely unknown, the burden of viral respiratory tract infections is uncertain, and it is unclear how and for how long viral shedding occurs in patients with influenza infections. COURSE will provide useful insights in all these issues. This may have implications for future allocation and methods of virus testing, and duration of anti-viral treatment and ICU infection prevention measures. In addition, COURSE may aid information on predictors for virus–positivity. Quantitative shedding parameters may also provide clinical endpoints for future studies with new antiviral therapies.
There is increasing awareness of the risks and burden of viral respiratory tract infections in ICU patients. Most respiratory viruses are highly contagious via aerosols and fomites, and have high infection rates during seasonal epidemics in the general population. Although viral infection usually leads to mild and self–limiting symptoms in the majority of infected patients, some patients may develop severe viral pneumonia with multi–organ failure [17]. Furthermore, respiratory viruses are also known causes of exacerbations of chronic lung disease [18-20].
Viral respiratory tract infections have an impact on infection prevention and control measures in the hospital. Over the past decade, advances in molecular diagnostics have provided highly sensitive, rapid and quantitative detection methods for viral pathogens, such as RT–PCR. However, despite these diagnostic tools systematic testing for respiratory viruses is not common practice in the ICU setting, as the impact of the diagnosis is often unknown and clear guidelines for testing remain lacking.
Prevalence of virus infections in the respiratory tract of ICU patients may be as high as 36% in patients with acute respiratory failure and/or a suspicion of a respiratory tract infection [5-11]. Studies reporting on the prevalence, however, suffered from several limitations. Selection of patients at high risk of viral infection in these studies may have led to overestimation of the prevalence of respiratory viruses. Vice versa, there may have been an underestimation because of selective inclusion, missing samples and/or incomplete analysis of samples. By systematic sampling of unselected acutely admitted critically ill patients, in both upper and lower airways, with uniform analysis using RT–PCR, COURSE will provide more robust data on the prevalence of viral infections in ICU patients. Furthermore, comparing study results (i.e., results from tests only performed because of COURSE) with standard of care test results (i.e., results from tests ordered by attending physicians) will provide a better insight in the proportion of respiratory viruses that normally stay undetected on the ICU. Notably, the attending physicians in the participating ICUs were not involved in COURSE, and were stimulated not to change their practice (i.e., tests were ordered when deemed clinically necessary). With respect to reporting bacterial co-infections, this study is limited by reliance on microbiology test results from samples obtained in routine care. While it could be argued that this may lead to an underestimation of reported bacterial infections, we actually think this is not a problem. In case of a suspected respiratory infection, without exception the attending physicians order microbiology tests in blood, sputum, and frequently also in tracheal aspirates or bronchoalveolar lavage fluids.
Respiratory viruses may play a significant role in clinical course and outcome of the critically ill. A large retrospective study reported an independent association between infection with respiratory viruses (influenza, respiratory syncytial virus, cytomegalovirus and herpes simplex virus) and adverse outcomes in critically ill patients, including acute respiratory distress syndrome, septic shock, multi system organ failure and death [12]. However, in prospective studies, viral infections in ICU patients admitted with a suspected respiratory infection show both positive as negative associations with disease severity and/or survival [5,6,8,10]. Furthermore, detection of viruses in the samples from the respiratory tract of critically ill patients does not necessarily mean that the viral infection actively contributes to disease. The distinction between asymptomatic or subclinical infections with respiratory viruses, virus–associated respiratory disorders, and virus induced respiratory disorders remains difficult to make with molecular diagnostic tools [6,21], although a quantitative analysis may improve the diagnostic accuracy [22,23]. Indeed, there are several studies indicating an association between viral load in nasopharyngeal samples and disease severity in adult and pediatric patients with viral infections [24-27], however there are also studies showing no correlations [28-30]. COURSE will provide quantitative measures of viruses present in both upper and lower respiratory tract samples of adult critically ill patients, and aims to provide useful estimations of burden of viral infections by exploring associations between infection, viral load and outcome in a large prospective cohort.
Viral shedding patterns in ICU patients remain to be explored, as parameters such as initial viral load and days to viral clearance are as yet poorly characterized [31]. Prolonged viral shedding has been described following infection with influenza virus and respiratory syncytial virus, especially in immunocompromised patients [32,33]. Knowledge on the duration of viral shedding may have implications for duration of antiviral therapy and infection prevention procedures. Also, it may provide valuable information for future studies on duration of antiviral therapy. Furthermore, the optimal diagnostic sampling site for viral detection remains to be determined. Some studies suggest that upper and lower airway sampling should be combined when performing virus diagnostics in critically ill patients [8,34,35]. These studies are however small and/or non–systematic. In COURSE both the upper and lower airways will be sampled and compared.
In conclusion, COURSE will be the largest prospective multicenter study that systematically assesses the prevalence, risk factors for, and burden of infection with respiratory viruses in intubated critically ill patients. Furthermore, COURSE will provide insight in viral shedding patterns in ICU patients with influenza infections.
Crucell Holland BV (Leiden, The Netherlands) and the Academic Medical Center (Amsterdam, The Netherlands) support COURSE financially.
The sponsors have no role in study design; collection, management, analysis and interpretation of the data; preparation, review and decision to submit scientific manuscripts.