Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Case Report - (2014) Volume 4, Issue 6
We describe the case of a 10 year old child with Leigh Syndrome. From 6 months of age, he developed eyelid, right upper limb clonus, sleep apneas, drooling, and hyperlactatemia, absence of the cough reflex, divergent strabismus, diffuse muscle wasting and dystonia. The MRI showed multiple lesions involving the lenticular nuclei, the thalami and cerebral peduncles and the periaqueductal front seat. The child has been undergoing since 2010, in the Department of Physical Medicine and Rehabilitation, “University ‘G. D’Annunzio” of Chieti, Italy, a specific rehabilitation project in order to maintain residual functionality, improve performance and tissue elasticity, stabilize metabolism and prevent the disease related complications.
Leigh syndrome was described by Denis Leigh in 1951 in a child who had a subacute neurological dysfunction characterized by sub-acute necrotizing encephalomyopathy [1]. Leigh syndrome is a mitochondrial disease. Mitochondrial diseases are a complex, heterogeneous and multisystem group of metabolic diseases that depend on mutations in the mitochondria or in the genes that control the oxidative phosphorylation [2]. In literature, mitochondrial diseases are identified by the maxim: “Tissue and Any Signs at Any Age” [3] since the organ damage usually affects multiple organs and systems at any age.
In particular, Leigh Syndrome, defined as subacute necrotizing encephalopathy, is considered the most common mitochondrial disease in childhood [4]. The estimated incidence of Leigh Syndrome is equal to 1:40,000 newborns [5].
Leigh’s disease is associated with mutations of the mitochondrial genome or nuclear dysfunction of the respiratory chain (especially complex I, II, III, IV or V) or, coenzyme Q, or the makers of the pyruvate dehydrogenase complex deficiency ATP production, increase of metabolic intermediates of the Krebs cycle, increased production of ROS and, therefore, ultimately organ damage for necrosis [6-8].
Diagnosis of Leigh syndrome is complex and takes place on the basis of the clinical history, instrumental analysis, laboratory and genetic data, and molecular biopsy. The most important clinical manifestations occur in the CNS with psychomotor retardation, nystagmus, ophthalmoparesis, optic atrophy, ataxia, dysphagia, hypotonia, marked fatigue, respiratory distress.
Pyramidal signs may coexist with increased muscle tone and ROT, retinitis pigmentosa, deafness. Alterations affecting the peripheral nervous system are common and occur with polyneuropathy and myopathy. There is also frequent impairment of organs requiring high metabolism energy with hypertrophic cardiomyopathy, liver disease with infiltration of fats, degeneration of the renal tubules. In the blood and CSF there is an increase in the levels of lactate and/or pyruvate, hyperlactatemia, increased lactate/pyruvate ratio.
In urine, there is an increase in the levels of lactate and specific metabolites of Krebs cycle.
In MRI, T2 hyperintensity is an evident signal in the basal ganglia, thalamus, substancia nigra, red nucleus, cerebellar cortex, white matter of the brain and spinal cord. Unifocal or multifocal areas of infarction, cortical atrophy with ventricular dilatation can coexist [9-13].
The life expectancy of these patients is extremely low, in many cases less than 5 years 6 to 14. Although numerous experimental studies for an appropriate pharmacological treatment for the disease are being researched, so far there are no pharmacological treatments and standardized rehabilitation of proven effect [14-17]. The aim of our study is to present a complex rehabilitation program in a case of Leigh syndrome in order to maintain the residual functionality, to improve performance and tissue elasticity, to stabilize the metabolism and prevent potential complications related to the disease.
We present the case of a child 10 years, suffering from Leigh syndrome in treatment for thirty-nine months at the Department of Physical Medicine and Rehabilitation, University G. D’Annunzio (Chieti-Pescara-Italy). Only child of healthy non-consanguineous parents, born at term, auxological parameters at birth were normal. At 6 months, paroxysmal episodes in the wake of the eyelid and right upper limb clonus first appeared. At 9 months, the child showed short sleep apnea episodes, drooling, and mild dysphagia.
At 10 months, laboratory tests showed hyperlactatemia and, in MRI multiple hyperintense lesions were observed in T2 and hypointense in T1, effecting the lenticular nuclei, partially the thalamus, the celebral peduncules and the periaqueductal front seat. The child had hyperreflexia-hypotonic syndrome associated with minimal dystonic signs, impaired extrinsic ocular motility of nuclear-internuclear type, hypotonia of oro-mandibular district with drooling, significant impairment of postural control. As for the electroencephalographic examination, the EEG pattern was of the kind theta 6-7 c/s, irregular, symmetrical in the two hemispheres, poorly organized, sequences of slow cusp wave of medium-voltage in the areas of the contralateral hemisphere united in bilateral discharges during the stages of lighter sleep. The diagnostic confirmation was obtained with the histological examination of muscle tissue and skin cells in culture and genetic analyzes. Diagnostic testing revealed a defect of complex I (NADH ubiquinone - oxidoreductase) of the respiratory chain associated with a mutation of mitochondrial DNA (t 14487 c). When the child reached one year of age, he showed absence of the cough reflex, dysphagia for not liquid food, increased salivation, increased muscle fatigue and cramps, excessive sweating, increased number of apneas and greater use of accessory respiratory muscles, respiratory failure by altering the control of the central nervous system requiring tracheotomy removed 13 months after.
Ultrasound examination showed a dilated cardiomyopathy. At 2 years of age, the swallowing process was impaired and, therefore, a PEG tube has been applied.
From the age of 6, the child has been followed at the Department of Physical Medicine and Rehabilitation, University G. D’Annunzio. In our department, at the age of 6 years, the child had spastic quadriplegia more expressed to the right side, dystonic components prevalent in the upper limbs, poor head control, widespread muscle wasting, ocular motility inter-supranuclear disorder, drooling and frequent episodes of vomiting. The language production was absent. The child was able to turn around from the supine to the left, but not to the right, could not roll, and was not able to sit up unaided.
The XR of the spine and pelvis showed wide-ranging right-convex scoliosis, back injury, bilateral coxa valga and dislocated right hip joint. Echocardiography showed a systolic murmur from mitral regurgitation (1-2/6). The child used, as aids, wheelchair with anatomical chair, the Ormesa dynamic walker with the support and bib pant.
The drugs taken by the child at the entrance in our department for the treatment were: Lucen (Esomeprazole 40 mg), Mnesis (Idebenone 45 mg), as supplements creatine, glutathione, quinone Q10, carnitine, n-acetylcysteine, folina, riboflavin, and amminometionina tiobec.
As for the clinical and functional picture presented by the child, he has been prescribed a complex rehabilitation project in order to maintain the residual functionality, to improve performance and tissue elasticity, to stabilize the metabolism and to prevent potential complications related to the disease.
The rehabilitation project carried out with the written and signed consent of the parents has been thus articulated:
• BIORESONANCE CYCLOTRON (technology QUEC Phisis- Prometheus Ltd) [18,19] with specific programs for enzymatic dysfunction and neuro-vegetative dystonia, of anergic kind (2 times a week for 10 months per year);
• VISS system (VISSMAN, Italy): high intensity focused acoustic waves system, 200 Hz, high-yield reduction with spastic hypertonus [20,21] (2 times a week for 10 months per year);
• Manual therapy [22] (1 time per week in the first year of therapy);
• Neuromotor rehabilitation in microgravity aquatic environment [23] (2 times a week for 10 months per year);
• Focused Extracorporeal Shock Wave Therapy [24-26] (Dermagold, HMT, Italy) for inhibition, bilaterally, in the spasticity of the thigh adductor and flexor muscles. (Once per week for 6 weeks, to be repeated every 6 months).
The results of the rehabilitation project have been analyzed at T0 (beginning of the rehabilitation-February 2010) and at time T1 (May 2013). Clinical parameters chosen for the analysis of the data, considering the complexity of the case, are:
• Laboratory tests (Tables 1 and 2)
| Exam Result | Normal Range | |
|---|---|---|
| Lactate | 13 | 6- 22 |
| GSH | 137 umol/l | da 500 a 1.500.00 |
| PH | 7,40 | 7,32-7,48 |
| PCO2 | 28 | 32-48 |
| PO2 | 96 | 83-108 |
Table 1: Laboratory tests T0 (2010).
| Exam Result | Normal Range | |
|---|---|---|
| Lactate | 10,3 | 6- 22 |
| Ph | 7,38 | 7,32-7,48 |
| PCO2 | 34,5 | 32-48 |
| PO2 | 98 | 83- 108 |
| HCO3 | 20,1 mmol /L | 19-27 |
| NA+ | 133,6 mmol /L | 135-148 |
| K+ | 3,32 mmol /L | 3,5- 5,3 |
| CA++ | 0,68 mmol/L | 1,12-1,32 |
| Glucose | 81 mmol/L | 60-110 |
| CPK | 137 UI /L | 32-296 |
| LDH | 345 UI /L | 230-470 |
| SGPT | 24 UI /L | 5-40 |
Table 2: Laboratory tests T1 (2013).
• Modified Asworth Scale (MAS) for spasticity (Table 3)
| MAS T0 (Febbraio 2010) | MAS T1 (Maggio 2013) | |
|---|---|---|
| Hip | 2 | 1 |
| Knee | 2 | 1 |
| Ankle | 2 | 1 |
Table 3: Modified Scale Asworth at T0 (February 2010) and T1 (May 2013).
• Bioelectrical resistance values (through the tissues and fluids) and reactance (through cell membranes) developed by QUEC Phisis technology (Prometheus Ltd.) (Table 4) (Figure 1).
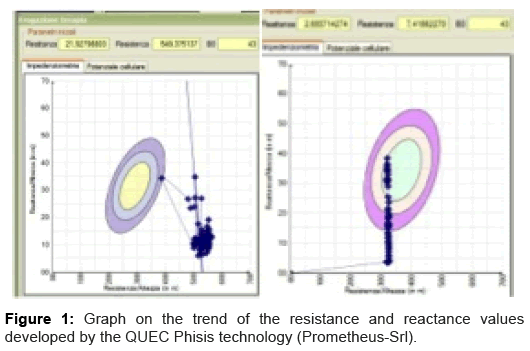
Figure 1: Graph on the trend of the resistance and reactance values developed by the QUEC Phisis technology (Prometheus-Srl).
| To | T1 | |
|---|---|---|
| Resistance | 549,37 | 2,69 |
| Reactance | 21,92 | 7,41 |
Table 4: Bioelectrical resistance and reactance values processed by the technology QUEC Phisis (Prometheus-Srl).
• Echocardiogram
• Reactivity of the patient to light stimuli and music.
The laboratory tests results show stabilization in the metabolic and normal values and acid-base balance within the normal range.
Bioelectrical resistance and reactance values, that are the expression of a better body homeostasis and less energy expenditure of the body, improved significantly between T0 and T1.
Echocardiogram 2010: systolic murmur from mitral regurgitation (1-2/6).
Echocardiogram 2013: normal size and ventricular contractility, normal valve function.
The reactivity to visual stimuli and music was calculated as a time of response latency in seconds using a specific scale for cases of mitochondrial diseases drawn up c/o the Department of Physical Medicine and Rehabilitation, University “G. D’Annunzio “(Table 5).
| Visual Stimulus | Musical Stimulus | |
|---|---|---|
| Minimum Time to Reaction | 1 second | 1 second |
| Maximum Time of Reactions | 10 seconds | 10 seconds |
Table 5: Reaction to the visual and music stimuli scale in mitochondrial disorders.
The visual stimulus was obtained with a flashlight briefly turned on each eye by covering the eye not being stimulated. The test was performed in a dark and quiet room. The response was calculated for each eye.
The response to musical stimulus was obtained through a CD player reproducing a song familiar to the child.
At T0 the time of reaction to the visual stimulation was equal to 8 seconds for the right eye and 10 seconds for the left eye. At T1, the time of reaction to the visual cue was equal to 3 seconds for the right eye and 6 seconds for the left eye.
At T0 the time of reaction to music cue was equal to 9 seconds. At T1, the time of reaction to music was 4 seconds.
An examination of the literature showed that the objectives pursued in clinical trials in the field of mitochondrial disease are common and aimed at improving the quality of life, keeping the remaining functionality, reducing the risk of complications and increasing the life expectancy.
The rehabilitation techniques most often used to achieve the objectives mentioned above are based on adequate nutritional support [16], on the respiratory function rehabilitation [27-30], cardiac rehabilitation, speech therapy, neuromotor rehabilitation (Vojta method, Kabat, Bobath), physiotherapy [31], proprioceptive rieducation of posture, neuromuscular facilitation techniques, neurocognitive rehabilitation [23], hydrokinesitherapy, occupational therapy and physical energies therapies.
An analysis of the literature shows a lack of guidelines and a lack of studies on rehabilitative protocols that have effect on the pathophysiological mechanism that is the cause of the disease. Even though, many pathophysiological mechanisms are still under investigation, it has been determined that the reduced ATP production and the consequent increase in ROS is the cause of the organ damage by necrosis. On the basis of these considerations, we have defined a comprehensive and case-specific rehabilitation protocol.
Since cells communication with each other is mainly of chemical type but also electromagnetic, we therefore applied, in order to optimize the cellular metabolism, the principle of Ion Cyclotron Resonance.
In recent decades, studies in biophysics have shown that, thanks to Ion Cyclotron Resonance, it is possible to stimulate the passage of ions across the membranes of living cells. The device is able to generate ELF field on a coil aimed at stimulating the motion of selected ionic species for example (Fe, Ca, Cu, Zn, Mg, K, Na) through the ion resonance effect. This makes it possible to modify the permeability thus enhancing the ion exchange on the two sides of the cell membrane. The increased bioavailability of the ions enhances the efficiency of cellular metabolism [32-34].
The bio-resonance is the form of resonance that occurs at the level of cell membranes using electromagnetic fields at very low intensity and a specific frequency (cyclotron) which is able to influence and stimulate the metabolism of human cells. It regulates the ordered ionselective traffic between the internal and external environment of the cell and stimulates the activity of metal-active enzymes involved in many biological reactions [35-38].
The QUEC Phisis technology generates electromagnetic waves of low intensity and frequency, applying the principle of the cyclotronic bioresonance. It allows, as a consequence, a ionic flow capable of optimizing the intrinsic capacity of maintaining the intra and extracellular potential difference, essential for the cellular metabolism and homeostasis [18,19-39].
This technique has the benefit of not being invasive. It analyzes the passage of very low intensity current through 4 electrodes placed at the ends of the legs and arms that detect bioelectric impedance (the opposition of a biological conductor, in this case the human body) at the passage of a weak alternating current.
During the treatment QUEC Phisis processes the bioelectrical values measured as follows: resistance (through the tissues and fluids) and reactance (across cell membranes).
We also used the manual therapy. It is well known that manual therapy leads to a reduction of the release of inflammatory cytokines such as Tumor Necrosis Factor-α (TNF-α), Interleukin-6 (IL-6) and a reduced phosphorylation of heat shock protein [27] (HSP27), thus relieving the cellular stress caused by injuries on muscle myofibrils, promoting mitochondrial biogenesis [22].
The neuromotor rehabilitation in microgravitary aquatic environment, according to the literature, has been chosen for the well known therapeutic properties of water at an average temperature of 33°/34°.
At these temperatures, the immersion of the body in the water increases muscle vascularization, the elimination of toxic substances, improves the muscles, tendons flexibility and capsular elasticity with consequent reduction of the tone.
There are effects on the renal system to increase diuresis and elimination of toxic substances, effects on the respiratory system to increase ventilatory capacity, effects on the cardiovascular system to increase venous return and cardiac output, peripheral vasodilation and blood pressure reduction. In this specific case, the action on the nervous system is of the utmost importance, due to the increase of exteroceptive, thermal and proprioceptive stimulation, and for relaxing and sedative effect [40-44].
ESWT were used to obtain a rapid inhibition of spasticity. The mechanism by which ESWT inhibit spasticity is still little known [24-26]. The most well-known mechanisms appear to be linked to the release of nitric oxide [45], to the decrease of excitability in the spinal cord [46], to the mechanical action generated on [47] Golgi tendon organs and to the mechanical destruction of chronic fibrosis present in the hypertonic muscle. The ESWT have been applied to the patient with the aim of obtaining a rapid inhibition of spasticity and leading to a rapid normalization of the tone and inhibition of pain.
Unfortunately, ESWT effect is not very durable, so, in order to obtain an improvement in the trophic muscle tone and more stable in time, we included in the rehabilitation plan, the whole-body vibration and high intensity focused acoustic waves (VISS) at 200 Hz with a system VISS (VISSMAN, Italy) [20,21].
This therapy was applied on individual muscle groups of the upper and lower limbs (biceps brachii muscle, the flexor muscles of the forearm, quadriceps femoris muscle, the flexor muscles of the thigh and bilateral twin’s muscles).
It has been suggested that the vibratory stimulus acts on a nervous reflex circuit involving the fibers Ia and the monosynaptic and spinal motor neurons, resulting in muscle contraction of the agonist and relaxation of the antagonist. The stimulus exerted on the Ia afferent fibers of muscle spindles leads to the activation of large amounts of α-motor neurons and to the recruitment of muscle fibers that were not active before [20].
In addition to that, at a specific frequency, the vibratory stimulation seems to affect the rheological properties of the muscle [21] with reduction of the spastic hypertonus [40].
This type of stimulus, however, would result in a longer lasting effect over time when the initial response is lower. Finally, some studies have reported the effectiveness of the energy of vibration on pain control; apparently, for the action carried by the vibration on myelinated fibers of large caliber, with analgesic action at the neural and medullary level [41-43].
We can hypothesize, on the basis of the metabolic and functional stabilization in the case report, that the pharmacological support should be combined with a comprehensive and specific rehabilitation program that is intended to act on the individual and dysfunctional components and aimed at reducing the cellular toxicity due to the increase of oxygen reactive species.