Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2012) Volume 2, Issue 3
Background: Organizational-level recruitment strategies have not been well detailed in the literature. This manuscript compares three methods of organizational level recruitment of beauty salons into a large community based cancer prevention intervention trial called The North Carolina BEAUTY and Health Project. Methods: Three recruitment methods (e.g. phone call prior to visit, drop-in visit or referral plus visit) were applied to a random sample of 100 salons per group to identify the most effective recruitment approach. Salons were considered eligible when they signed a study agreement form. The goal was to recruit at least 60 salons from which 40 would be selected to participate in the trial. Here we report salon recruitment procedures, sub-study results by method, and related recruitment costs. Results: Of the 62 salons which signed study agreement forms, 13/318 (4.1%) were recruited via the phone call prior to visit method; 32/222 (14.4%) via the drop-in visit method; and 17/34 (50%) via the referral method. The costs per salon recruited by each method were determined as well. Conclusions: The referral method, made possible due to the community-based participatory research approach, provided the best recruitment yield overall; yet available time, personnel, resources and costs must also be considered when selecting among future organizational level recruitment methods.
Keywords: Organizational recruitment; Community-based interventions; Beauty salons
Developing innovative strategies to reach and engage with African American populations who are at increased risk of a number of preventable diseases is an important and challenging public health undertaking. Community-based participatory research (CBPR) methods are believed to be an effective approach for addressing individuals and groups who suffer disparities in health [1-3], but very little attention has been paid to the effects of CBPR on organizationallevel recruitment. In fact, recruitment procedures and results at the organizational level are highly under-reported [4]. Despite this, it is clear that organizational recruitment is instrumental to the successful recruitment of individuals [5]. Moreover, organizations are key contextual settings that directly impact intervention effectiveness [6]. Historically, a number of CBPR-based studies have targeted African Americans within church settings [7,8]. And while targeting church settings has proved effective for reaching a segment of African Americans, not all are church-goers [9]. Thus, new settings for reaching and engaging with African Americans are needed if we are to address key disparities in health.
Beauty salons are becoming increasingly recognized as an important setting for reaching large numbers of women with health promotion messages [10]. There have been several previous salon based programs that successfully recruited underrepresented women into health screening and education programs (e.g., hypertension, CVD, mammography, cervical screening, HIV/STD screening, and smoking cessation) [10-15]. Beauty salons can be found in virtually all communities. In the U.S., there are over 629,000 salons and spas with 800,000 stylists [16]; while North Carolina alone has over 13,600 salons [17]. Beauty salon customers are typically loyal, consistent, recurrent patrons. Most relevant for potential public health interventions, beauty salons also represent a place where beauty and health-related issues are regularly discussed [18]. While targeting beauty salons provides access to many types of women from various racial, ethnic, and economic backgrounds, there is evidence that these settings are particularly promising for reaching African American women given the cultural, economic and political history that beauty salons have with this population [19].
The North Carolina BEAUTY (Bringing Education and Understanding to You) and Health Project were designed to evaluate the effectiveness of beauty salons as a setting for delivering lifesaving health and cancer prevention information to African American women. This community-based participatory research study utilized three different organizational level recruitment strategies to enroll 40 African American beauty salons into the trial [20]. This paper will focus on the organization (salon)-level recruitment results. Given the growing interest in this setting for reaching African American women, a description of the recruitment sub-study procedures, results, costs and lessons learned will fill an important gap in the literature.
Initial salon-level recruitment protocol
Since salons are small businesses, we developed our initial salon recruitment approach based on worksite-level recruitment strategies [21-23]. The draft protocol and materials were vetted through The North Carolina BEAUTY and Health Advisory Board, whose members helped the research team develop all final salon and customer-level recruitment materials and strategies [20].
Figure 1 summarizes the overall recruitment strategy. Eligible salons were located within a 75-mile radius of Chapel Hill, not part of a franchise, and served at least 75 customers who were primarily African Americans [24,25]. Project staff obtained a list of all licensed beauty salons from the North Carolina State Board of Cosmetic Art Examiners [26]. Out of 12,319 licensed salons, a total of 5,119 were located within a 75-mile radius of Chapel Hill. Salons known to be part of a franchise were excluded, leaving a total of 4,462 potentially eligible salons. After matching phone numbers of the remaining licensed salons to confirmed telephone listings, staff identified 2,628 potentially eligible salons. This group was further divided into two recruitment phases based on distance to Chapel Hill: n=1,413 salons for phase 1 (closest to Chapel Hill) and n=1,215 salons for phase 2 (further from Chapel Hill). Since the recruitment goal was met with the phase 1 group, we did not approach any phase 2 salons. From phase 1 salons, 200 were randomly selected to complete a pilot “run-in” salon recruitment effort over a two-month period which tested the initial recruitment approach and gave the research team an estimate for how long it would take to recruit 60 salons.
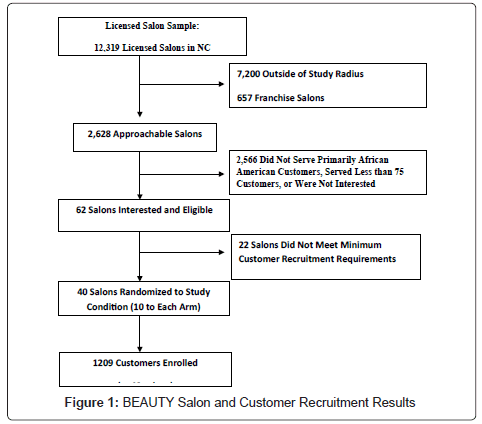
Figure 1: BEAUTY Salon and Customer Recruitment Results
The run-in pre-test of the salon recruitment protocol consisted of three basic steps. First, potential salons were called to inform salon representatives about the study and determine initial eligibility. If the salon met initial eligibility over the phone, the salon owner received a BEAUTY Project information fact sheet and cover letter by mail. Next, each salon received a follow-up phone call with the goal of scheduling a salon visit. During the visit, salon owners were introduced to project staff and shown a 10-minute recruitment video “It’s More Than Just About Hair” which featured several Advisory Board members and members of the research team, encouraging salon owners to join the study. Project staff confirmed eligibility, answered questions and provided further detail about the study, stylist roles/responsibilities and customer recruitment. Enrollment was finalized when the salon owner signed a study agreement form, which included informed consent. During the run-in, 16% (32/200) of salons met eligibility criteria and advanced through the next stage in the recruitment process. Forty percent (87/200) of the sample did not meet eligibility criteria; 22% of the sample refused to participate (43/200) and another 16% could not be reached either due to non-response (22/200), wrong numbers (3/200), or disconnected numbers (8/200). Of the 32 salons that met initial eligibility criteria, 14 were not interested in participating and another three could not be reached after at least 8 phone calls, leaving 10 interested salons. After a total of two months of this run-in recruitment test, 10 interested/eligible salon owners were visited and 8 enrolled in the study. However, the research team quickly realized that we would not have sufficient time to complete enrollment of at least 60 salons using this approach in the time available for the study. Thus, the research team designed a sub-study to compare the success (e.g. yield) and costs of three different salon-level recruitment methods to determine which method would optimize the time, outcome (yield) and cost-effectiveness of salon-level recruitment efforts. No previous studies had undertaken this type of sub-study. We expected to learn which method could help accelerate the salon recruitment process, and to gather valuable data to inform future salon-based recruitment efforts.
Recruitment sub-study design and description
The organizational recruitment sub-study (Figure 2) compared the “yield” or signed agreements obtained from three recruitment approaches (1) Referrals from project advisory board members; (2) In-person visits or “drop-ins” to salons; and (3) Phone calls to salons (e.g. similar process to the run-in protocol where project staff contacted salon owners to verify eligibility prior to a visit). Recruitment costs (staffing, travel and materials) were also computed for each method.
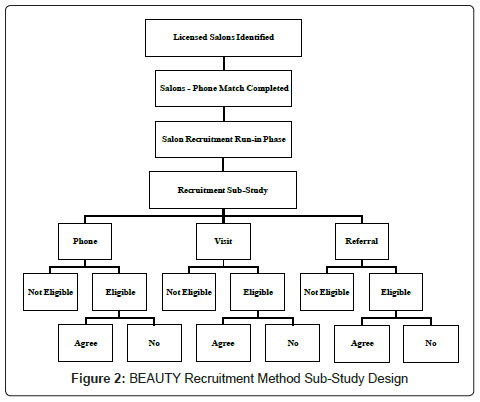
Figure 2: BEAUTY Recruitment Method Sub-Study Design
Replicate samples of approximately 100 salons each were randomly selected from the original phase 1 sample of licensed salons. Each replicate sample (100 salons) was then randomly assigned to either the drop-in visit or phone call recruitment methods. The recruitment method was applied to all 100 salons in that replicate sample and the plan was to continue recruiting until our quota of at least 60 salons was achieved, while exhausting each replicate sample so that we would have a comparison across methods. Although each of the recruitment approaches began with a phone call to assess initial eligibility (e.g., Do you serve primarily African-American? and do you have at least 75 customers?), once potential eligibility was established, one of two recruitment methods were applied based on assignment. The third method (referral) is described further below.
For the phone method, procedures were generally consistent with the previously discussed run-in procedures. In the visit method, following the initial eligibility call, project staff made “drop-ins” to targeted salons when research team members were in a specific town/geographic location. If it was not a convenient time to do the recruitment visit then, research team members scheduled a better time to return. This method put a “face” to the research team (vs. a straight phone or cold call approach). In the referral method, Advisory Board members provided contact information (name/location) for salons they thought might be interested and/or suitable for the study. During the phone call to determine initial eligibility, research staff members stated that a particular Advisory Board member had recommended that we contact this salon. Once eligibility and initial interest was determined, the same recruitment visit and protocol was done with all three recruitment methods (e.g. share materials, show video, describe study, obtain informed consent and signed study agreement form which signified a salon was enrolled).
In addition to enrollment in the study, referred to as recruitment “yield”, we also determined the cost of recruiting salons into the study by method of recruitment. There were shared costs which included the cost of developing the video, print materials describing the project, software for identifying salons, and portable TV/VCRs to play the video in the salons. The total for shared costs was $5910; and it was apportioned to recruitment method based on the size of each sample. We added recruitment method-specific costs (e.g. phone, travel and personnel costs) to the shared cost for each recruitment method. Next, we calculated two types of recruitment costs. First, we divided by the total number of salons in each recruitment sample to determine the cost per salon if we were 100% successful at recruiting salon using each method. Next, we divided by the number of enrolled salons to determine the actual recruitment cost per enrolled salon. Together, these values provide useful insights about the costs associated with recruitment.
Salon-level recruitment by method
Overall, the combination of recruitment methods (including the pre-test which yielded 8 salons) resulted in a pool of 62 interested and eligible salons. Figure 3 shows the number of salons by recruitment method and the number which were determined to be eligible and interested in the study. For the phone method, we randomly selected 318 salons (e.g. just over 3 replicate samples of 100 salons). Of those, 56 (17%) were determined to be eligible and interested in the study. Of the 318 where we applied the phone recruitment method, 40% of salons (n=127) were not eligible, 22% (n=70) were not interested in participating, and 13% (n=41) were not reachable by phone to verify eligibility with at least 8 attempts. From the 56 determined to be eligible, 32% (n=18) agreed to a visit and 23% (n=13) signed an agreement. Thus, from the overall sample of 318 salons, the phone method had a recruitment yield of 4.1% (13 signed agreements from 318 in the sample). The 13 signed agreements also represent 23.2% (13/56) of eligible salons and 72.2% (13/18) of the salons that were visited.
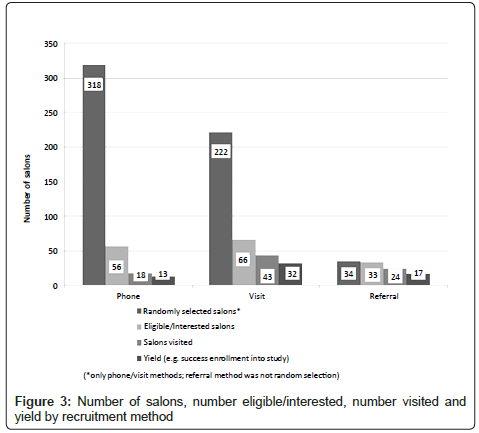
Figure 3: Number of salons, number eligible/interested, number visited and yield by recruitment method
For the visit method, just over 2 replicate samples (n=222 salons) were randomly selected and the “drop-in” visit recruitment method was applied to them. Of those, 66 (29.8%) were determined to be eligible and interested in the study. Of the 222 where we applied the visit method, 49% (n=109) were not eligible, 5% (n=11) were not interested in participating, 5% (n=11) were interested but could not participate for other reasons (e.g. planned to move locations, close business, ownership change, etc.), and 5% (n=11) were not reachable by initial phone contact to verify eligibility with at least 8 attempts. From the 66 eligible/interested salons, 65% (n=43) were visited and 48% (n=32) signed an agreement. Thus, from the sample of 222 salons, the visit method had an overall recruitment yield of 14.4% (32 signed agreements/222 in the sample) or 48.5% of salons that were eligible (32/66). The yield of 32 signed agreements represents 74.4% of those who received a visit.
For the referral method, 34 salons were recommended to the research team by advisory board members. Of these, all but one (33/34) were determined to be eligible after an initial phone contact. From the 33 eligible/interested salons 73% (n=24) were visited and 52% (n=17) signed an agreement. Thus, from the sample of 34 salons, the referral method had an overall recruitment yield of 50% (17 signed agreements from 34 in the sample). The 17 signed agreements also represent 51.5% of those eligible (17/33) and 78% of those who received a visit.
Recruitment costs
For the phone method, the total cost if we had been successful in recruiting 100% of the salons in the sample of 318 was $13.29/salon based on $951 (personnel costs)+$3274 (portion of shared cost=$4225/318). Because we successfully enrolled just 13 salons using the phone method, the actual recruitment cost was $4225/13 or $325/salon for the phone method. For the visit method the total cost to recruit 100% of the salons in the sample of 222 was $27.80/salon based on $793 (personnel costs)+$538 (travel costs)+$2286 (portion of shared costs)=$3888/222. Because we successfully enrolled 32 salons using the visit method, the actual recruitment cost was $3888/32 or $121.50/salon for the visit method. For the referral method, the total cost to recruit 100% of the salons in the sample of 34 was $52.44/salon based on $793 (personnel costs+$350 (travel costs)+$640 (portion of shared costs=$1783/34. Because we successfully enrolled 17 salons with the referral method, the actual recruitment cost was $1783/17 or $104.88/salon for the referral method. Thus, recruiting salons using the referral method cost the lowest ($105/salon), followed by visit method ($122/salon), then phone method ($325/salon).
Organizational level recruitment efforts are critically important to the success of community-based research studies, yet are often not reported in the literature. This paper describes procedures associated with an organizational recruitment approach, and specific sub-study results associated with three different recruitment methods (phone, visit and referral) used to recruit beauty salons into the North Carolina BEAUTY and Health research study, a community-based participatory research study testing different ways to promote cancer prevention information in African American beauty salons. Results were used to make decisions about which recruitment method was most expedient and cost-efficient; and can be used to inform future recruitment efforts.
The phone recruitment method achieved signed agreements for 13 salons (4.1% of the initial sample of 318 salons; 23% of eligible salons; and 72.2% of visited salons) and the visit recruitment method achieved signed agreements for 32 salons (14.4% of 222 salons; 29.8% of eligible salons; and 74.4% of visited salons). Thus, overall, the visit recruitment method yielded more than twice the number (and 3 times the percentage) of salons compared with the phone method. The referral recruitment method was consistent with community-based participatory research principles. For the referral method, we obtained 17 signed agreements (50% of 34 salons; 73% of eligible salons; and 78% of visited salons). Clearly, the referral method yielded a significantly higher percentage of agreements than either the phone or visit method. In addition, the referral method was associated with nearly all (33/34) salons being eligible while just 40% of salons from the phone method and 49% of salons from the visit method were not eligible for the study. Additional time and resources are expended to determine that salons are not eligible; thus, the referral method provided a distinct advantage for identifying eligible salons.
Despite the apparent advantages of the referral recruitment method, these sub-study results make it clear that trade-offs exist and “one size does not fit all” in making decisions about which recruitment method is most appropriate. The referral method demonstrated a significantly higher overall yield, but this method is reliant on using the advice of an engaged Advisory Board like the one established for the NC BEAUTY and Health project. The BEAUTY Advisory Board members included licensed cosmetologists, beauty product distributors, a health department representative, two beauty school directors, licensed stylists, and several health professionals. This Board had been in existence for at least four years when this study was undertaken so members made excellent referrals based on a good working knowledge of what type of salons might be eligible and interested in working with us on this study. While the strengths of CBPR principles have been lauded in many ways, no previous studies have focused on the advantage of CBPR for organizational recruitment. This study clearly demonstrates the value of Advisory Board member referrals to overall recruitment efforts and the comparative advantage of CBPR-based approaches over traditional phone or visit recruitment methods.
In this study we also learned that one must take into account the time available for recruitment, the number and type of personnel available to do recruitment, and the complexity of the study that a given organization is being recruited into. The pilot run-in using the phone method was only successful in recruiting 8.7% (8/91) of eligible salons. When we decided to conduct the sub-study, our research team learned that the phone method was more time intensive because it took much longer to identify eligible salons, and salons were more than four times more likely to say they were not interested and three times more likely to have unreturned calls than salons recruited with the visit method.
The cost of recruiting organizations into community-based intervention trials is important but has not been well-documented [27]. Results of this study revealed that if each salon in our phone method sample were successfully enrolled, it would have cost $13.29/salon; however, because we actually enrolled 13/318, the actual cost was $325/salon recruited. Thus, the phone method was nearly three times the cost when similarly compared to the visit method ($121.50/salon) or referral method ($52.44/salon). It takes personnel time (and thus money) to pursue a long list of ineligible or uninterested salons that one must do if the phone method is employed; thus the referral method is simply more efficient.
No matter which recruitment method we used, our results indicated that if we were effective in getting to a salon visit, it was likely to lead to a signed agreement. Specifically, 72.2% of eligible phone method salons that agreed to a visit signed an agreement form, compared with 74.4% of visit method salons and 78% of referral method salons. Thus, no matter which method was initially used to identify eligible salons, once a research team member was able to get an in-salon visit, a very high percentage of salons signed the agreement form. What is the explanation for the success rate when visits were held?
First, our research team was highly skilled interpersonally so they developed a good rapport with the salon representatives. Second, if a salon agreed to a visit, one can assume they were at least somewhat interested in the study. Third, our team had the opportunity to try out and refine the visit protocol as part of the run-in recruitment test. Fourth, we used the same approach during each salon visit and it included a highly effective video as part of the recruitment protocol. The “It’s More than Just About Hair” is a powerful 10 minute video that was shown to all owners during the visit and included the following: 1) An introduction to the overall goals of the study; 2) messages from several licensed stylists and owners who had participated in a previous salon-based study [28]; 3) encouragement from two BEAUTY Advisory Board members to join the study, including the President of the NC Cosmetology Association. This video provided a visual and strong encouragement for salon owners to join the study. They heard from credible sources (e.g. respected Board members and salon owners/stylists) and then were given an opportunity to ask questions of our research team members before being invited to sign the study agreement form. This visit protocol proved highly successful and has been adapted for use in subsequent worksite and barbershop-based research studies with comparable results [29].
Salon owners and stylists are typically very busy and are not able to spend much time on the phone. Our results confirmed that the phone recruitment method proved difficult, and clearly drop-in visit and referral recruitment methods, which include face-to-face meetings, may be necessary to simply get the conversation started when recruiting salons into a research study. When combined with the opportunity to build a partnership with researchers to promote health in their salons, most owners and stylists were interested in hearing more about the research study focused on health promotion. Recruitment procedures that are respectful of the time demands of owners/stylists send the right message about this partnership, which is another reason why community-based participatory research principles may be particularly effective with salon-based recruitment.
Several study limitations are noteworthy. First, despite the fact we could randomly assign replicate samples of 100 salons to phone or visit methods, we were not able randomly assign salons to the referral method approach. That is, Board members provided the names of 34 salons and we approached all of them to determine eligibility and then visit those who were interested (and eligible). As a result, we have a randomized trial providing a very strong comparison of the phone and visit recruitment methods, but a select group of salons to compare using the referral method. While a limitation, it is also strength of this study that we had the opportunity to compare phone and visit methods to a community-based participatory research approach (e.g. referrals from Board members) which has not been done previously in the literature. Three additional strengths of this study include: 1) a run-in test of the initial recruitment procedures; 2) use of CBPR approach to inform all aspects of the recruitment effort; and 3) takes advantage of opportunity to provide an estimate of the recruitment costs if all salons in a particular method were recruited; and the costs per actual enrollment comparing three recruitment methods.
In summary, our recruitment efforts successfully enrolled 62 beauty salons into North Carolina BEAUTY and Health research study. The referral method had the best yield, followed by visit and phone methods. We believe these results represent the first attempt to test different recruitment methods to enroll beauty salons into a community-based intervention trial. As such, it will provide very useful guidance about salon recruitment for other researchers who intend to conduct beauty salon or barbershop studies in the future. Moreover, these results provide additional important information about costs associated with different types of organizational-level recruitment into a community-based intervention trial, which has been missing from previous recruitment studies but helpful in considering important trade-offs of multiple approaches for both practice and future research studies.
The authors thank co-investigators Alice Ammerman, Peggy Bentley, Andrea Biddle, research team members Veronica Carlisle, Kacey Hanson, Katrina Debnam, all participating beauty salon owners/stylists, and members of the North Carolina BEAUTY and Health Advisory Board, especially Morris Boswell and Joyce Thomas, for their invaluable assistance on this study. In addition, we thank Ms. Carolyn Naseer for her assistance in getting the manuscript ready for submission.