Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2013) Volume 1, Issue 4
Background and aims: Anti-coagulation is an important component of post-operative Venous-Thombo-Embolic (VTE) prophylaxis but can be associated with significant complications including hemorrhage. Current guidelines favour anti-coagulation for ≥ 14 days with little evidence evaluating the efficacy of anticoagulation <14 days. Our study hypothesizes that short course Low-Molecular-Weight-Heparin (LMWH for 5-7 days) in combination with Calf Compression Device (CCD) is equally effective as standard therapy LMWH (14 days) in preventing VTE and related events amongst patients undergoing Total-Knee-Replacement (TKR).
Methods: Eighty-three patients undergoing TKR were randomly allocated to either: Group 1 short course LMWH (5-7 days) with CCD or Group 2 standard course LMWH only (14 days). Patients were followed up daily for five days post-operative and then at regular intervals for twelve weeks assessing for: deep-vein-thrombosis and pulmonary embolus, bleeding, exaggerated pain, wound infection, leg swelling and need for extended hospitalization beyond 5 days. Incidence comparisons between groups were made using Pearson’s chi-square or Fischer’s Exact tests and an accepted group treatment difference of 15% was selected based on previous studies to calculate equivalence powers.
Results: The incidence of DVT was equal between groups (n=3), 2% (95% CI -13.4, 14.1%). There was a single case of asymptomatic PE in the short course group though the group difference was not significant (p=0.486). Patients in the short course therapy group also demonstrated significantly lower rates of post operative leg swelling (p=0.004). Group comparisons for all other study endpoints did not reach significance.
Conclusions: In this study combined short course therapy was equally effective as standard therapy in preventing DVT and non-fatal PE, and superior to standard therapy in limiting post-operative leg swelling amongst patients undergoing TKR. Trial registered at Australian New Zealand Trial Registry: ACTRN12613000240741.
Keywords: Prevention; Deep-vein-thrombosis; Total-kneereplacement; Calf-compression device; Low-molecular-weightheparin; Short-course; Randomized; Prospective
Venous thromboembolism (VTE) can be associated with significant morbidity and mortality including fatal Pulmonary Embolus (PE), symptomatic Deep Vein Thrombosis (DVT) and PE, increased risk of recurrent VTE and chronic post-thrombotic syndrome [1]. In 2010, around two thousand deaths were reported from VTE and related events in Australia alone, 40% of which occurred in postoperative patients [2]. Preventative measures such as anti-coagulation, intermittent pneumatic compression, anti-embolic stockings and early mobilization have all been shown to significantly reduce the incidence of VTE [2]. There is however risk associated with anticoagulation use, in particular major hemorrhage carrying a significantly high mortality rate [3]. Other complications associated with anti-coagulation use which have the potential to cause considerable morbidity and mortality include injection site erythema, hematoma, Heparin Induced Thrombocytopenia (HIT) and allergy. These effects are amplified when treatment extends beyond fourteen days [4,5], thus alternative approaches to anti-coagulation regimens in the peri-operative period are required.
Current anti-coagulation guidelines for patients undergoing total knee replacement surgery remain controversial and highly variable suggesting thromboprophylaxis with LMWH, vitamin k antagonists, or fondaparinux be continued for at least ten days and upto three weeks post-operatively [6-8]. There is little data evaluating the use of shorter duration anticoagulant therapies for VTE prophylaxis in patients undergoing elective total knee replacement (TKR) surgery. Our study hypothesizes that short course therapy (enoxaparin daily for 5-7 days and pneumatic calf compression for 14 days) is equally effective as standard therapy (enoxaparin daily for 14 days) in limiting post operative morbidity and mortality amongst patients undergoing TKR.
Patients undergoing elective total knee replacement surgery at St George Private Hospital were invited by clinicians at the time of pre-admission to voluntarily participate in the study over a twelve month period by way of a confidential questionnaire (353 patients in total). Willing participants were referred to the trial co-ordinator/ nurse supervisor for enrollment, consent and randomization. Eightythree patients provided written consent to participate in the study (43 female, 34 male, mean age 71.145 years; range 40-91 years). Patient confidentiality was maintained by way of de-identified codes.
The study was double blinded at the time of randomization and patients were assigned by computer matching (no blocking restrictions) to either Group 1 (short course therapy, 42 patients) (enoxaparin 40 mg£ subcutaneous (SC) daily for 5-7 days post-operativelyα1 and automated mobile pneumatic calf compression for 14 days post-operatielyβ) or Group 2 (standard therapy, 42 patients) (enoxaparin 40 mg SC daily for 14 days post-operatively). Once allocated, both patients and clinical staff were made aware of their treatment group.
The following patients were excluded based on results from the questionnaire and pre-operative clinical assessment: known thrombophilic abnormality, morbid obesity (BMI>35), gross lower limb edema (limiting application of calf compression device), active leg ulceration, active malignancy, history of recurrent VTE, current users of anti-coagulation for other reasons, severe mental disorders (MMSE <25 or active psychiatric disorder), non-English speaking without reliable interpreter access and age <18. Major inclusion criteria included age 18-75, English speaking and willing to apply calf compressors appropriately at home and participate in regular follow up as well as no personal or family history of active/inactive thrombophilia, active malignancy, recurrent DVT/VTE, leg ulceration or morbid obesity (BMI>35).
Treatment efficacy was determined by measuring the following primary and secondary study endpoints: Primary: (a) radiologic evidence of DVT using venous Doppler Ultrasound (US) on day 5 post operative (b) Computed Tomography-Pulmonary angiography (CTPA)/ ventilation-perfusion (VQ) scan if patients demonstrated positive DVT US findings or reported any new onset symptoms suggestive of PE in the post operative period (up to 12 weeks post operative); Secondary: a) bleeding (wound site hematoma or need for transfusion products i.e. Hb<80 g/L), b) prolonged hospital stay beyond seven days, c) wound infection d) leg swelling and e) pain requiring additional analgesia.
Patients were discharged on day five, six or seven after excluding wound infection and other factors that may interfere with use of CCD post discharge. Patients were followed up at the same institute as enrollment at regular intervals for twelve weeks post operative (Figure 1). Interval assessment included evaluation for clinical features of DVT/PE and cardio-respiratory symptoms, presence of leg swelling, bruising, hematoma and superficial wound infections. A patient was recorded to have a positive study endpoint if they developed symptoms at any stage during follow up and only results of those patients who completed follow up at week twelve were taken into account for statistical analysis. Between follow up appointments patients were called on a weekly basis by clinical trial nurses and assessed for: device/ therapy compliance and any symptoms suggestive of DVT/PE. Those with positive symptomatology were recalled for immediate assessment and persons from the short course therapy group were instructed to cease usage of the CCD in the setting of significant leg swelling or pain. All patients with positive findings of DVT and or PE completed appropriate anti-coagulation therapy and were followed up at regular intervals with repeat imaging to ensure thrombus resolution. Patients who were non compliant with or unable to continue use of CCD (e.g. due to significant leg swelling) were also discontinued from the trial.
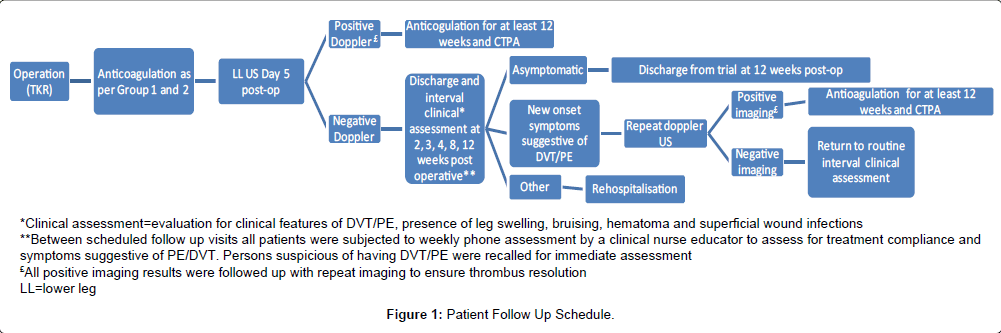
Figure 1: Patient Follow Up Schedule.
Doppler US was employed to assess for the presence of DVT based on 95-99% sensitivity for detecting lower leg DVT when combined with clinical assessment [9]. MRI venography and conventional venograms remain superior to Doppler US for detection of pelvic DVT, however majority of DVT post TKR occur in the lower calf and only 5-10% of DVT following THR occur in the upper mid-upper leg or pelvis [10]. Moreover, as this study is intended to develop recommendations regarding assessment and management of VTE within a routine clinical setting, the convenience, availability and feasibility of Doppler US over other imaging modalities promotes its use.
All procedures employed in this study were carried out in accordance with the document ‘When does quality assurance in health care require independent ethical review? Advice to Institutions, Human Research Ethics Committees and Health Care Professionals’ as per recommendations by the National Health and Medical Research Council, Australia. The study was approved by the South Eastern Health Human Research Ethics Committee: reference number 04/64 and registered with the Australian New Zealand Trial Registry (no: ACTRN12613000240741).
Statistical analyses were performed using IBM SPSS statistics (V 19.0.0 IBM Corporation, Armonk NY USA). Comparisons of the proportion of adverse events (imaging evidence of DVT/PE, bleeding and prolonged hospital stay) between groups (as originally allocated by computer randomization) was made using Pearson’s Chi-Square test or Fisher’s Exact test where the minimum expected cell frequency assumption was violated. Using the exact tests the probability of the observed outcome or an outcome more extreme is calculated exactly based on the distribution of the test statistic, rather than relying on the asymptotic assumptions of large sample sizes and balanced data distributions. A p value of less than 0.05 was considered statistically significant.
All major studies evaluating the efficacy of anti-coagulant based with non anti-coagulant based regimes for preventing VTE amongst post operative orthopaedic patients have found the former to be superior by 21-47% depending on patients’ co-morbid risk factor profile [11]. Hence, as both group interventions in this trial include the use of anti-coagulation, an acceptable group treatment difference of ± 15% was conservatively chosen to calculate equivalence powers.
Table 1 summarises the demographic characteristics of the studied patient groups. Six patients were lost to follow up due to geographical distance [4] or non compliance with CCD [2] leaving thirty-eight patients in Group 1 and thirty-nine patients in Group 2.
| Group 1(LMWH + CCD) | Group 2(LMWH) | |
|---|---|---|
| Total (n) | 38 | 39 |
| Lost to f/u (n) | 2 | 4 |
| Female (n) | 20 | 23 |
| Male (n) | 18 | 16 |
| Age Range (yrs) | 40-91 | 54-91 |
| Median Age (yrs) | 71 | 72 |
Table 1: Demographic characteristics for group 1 and group 2.
The incidence of DVT and PE for both groups is summarized in Table 2. Three cases of DVT were recorded in each group. The difference in the proportions was 2% (-13.4, 14.1%), the 95% CI was within the clinically acceptable range determined a priori (± 15%) and therefore the treatments were considered equivalent for this outcome. Two out of three DVT in Group 1 and all DVT in Group 2 were asymptomatic and were recorded at Day 5 post operative. One DVT in Group 1 was symptomatic and was recorded at the 4 week follow up assessment; this DVT progressed to asymptomatic PE. No DVT in Group 2 progressed to PE. There was no fatal PEs recorded for either group. The difference in incidence of DVT between the groups was zero (P=1.000, Fisher’s exact test). The difference in incidence of PE between the groups was not significant (Group one 1/38, Group two 1/39, p=0.486, Fisher’s exact test). The proportion of symptomatic versus asymptomatic DVT was 1/38 (2.63%, CI 0.05%, 13.49%) and 2/38 (5.26%, CI 1.5, 17.3%) respectively for Group 1 and 0/39 (0%, CI 0, 9.0%) and 3/39 (7.89%, CI 2.7, 20.8%) respectively for Group 2.
| Group 1 (LMWH+CCD) | |||
|---|---|---|---|
| DVT (n=3/38)(n=1/3) | Symptomatic | Time of DVT detection | Progress to PE |
| Case 1 | No | Day 5 | No |
| Case 2 | No | Day 5 | No |
| Case 3 | Yes | Week 4 | Yes |
| Proportion 1/38 (2.63% CI 0.05%, 13.49%)Proportion 2/38 (5.26% CI 1.5, 17.3%) | |||
| Symptomatic Asymptomatic | |||
| Group 2 (LMWH) | |||
| DVT (n=3/39)PE (n=0/3) | Symptomatic | Time of DVT detection | Progress to PE (n=0/3) |
| Case 1 | No | Day 5 | No |
| Case 2 | No | Day 5 | No |
| Case 3 | No | Day 5 | No |
| Difference in incidence of PE between groups (Group 1: 1/3 vs. Group 2: 0/3)P=0.486 (Fischer’s Exact Test) | |||
| Difference in Proportions of PE (Group 1 vs Group 2) | |||
| 2% (-13.4 to +14.1%); clinical acceptable treatment difference +/- 15% | |||
Table 2: Incidence and timing of DVT/PE for group 1 and group 2.
The incidence of all remaining study endpoints is summarized in Table 3. The incidence of patients reporting leg swelling in Group 2 was significantly higher than Group 1 (Group one 5/38, Group two 19/39, p=0.001, χ2=11.34, df =1). The difference in the proportions between the groups for remaining study end points were not statistically significant: pain (Group one 8/38, Group two 8/39, p=1.000, Fisher’s exact test), wound infection (Group one 3/38, Group two 1/39, p=0.108, Fisher’s exact test), bleeding (Group one 2/38, Group two 2/39, p=1.000, Fisher’s exact test) and hospital stay beyond 7 days (Group one 1/38, Group two 2/39, p=1.000, Fisher’s exact test). No patients required blood transfusion.
| Difference | Group 1 (LMWH + CCD) | Group 2 (LMWH) | |
|---|---|---|---|
| (n) | (n) | (p-value) | |
| Leg swelling | 5/38 (13%) | 19/38 (50%) | 0.001* |
| Pain | 8/38 (21%) | 8/38 (21%) | 1.000 (FI) |
| Wound infection | 3/38 (8%) | 1/38 (2%) | 0.108 (FI) |
| Bleeding | 2/38 (5%) | 2/38 (5%) | 1.000 (FI) |
| Stay >7 days | 1/38 (2%) | 2/38 (2%) | 1.000 (FI) |
Table 3: Incidence of non-DVT/PE study endpoints for group 1 and group 2.
In this study, short course therapy (enoxaparin 40 mg SC daily for 5-7 days and CCD for 14 days) proved to be equally effective as standard therapy (enoxaparin 40 mg SC daily for 14 days) in preventing DVT and fatal PE at twelve weeks post operatively and superior to standard therapy in limiting post-operative leg swelling amongst patients undergoing elective TKR.
Three cases of DVT were recorded in each group (Group one 3/38, 7.89% and Group two 3/39, 7.69%) with all recorded DVT occurring within four weeks post-operative. Given that a clinical difference of 15% in favor of the treatment or control was considered acceptable the confidence interval of the difference in the two proportions indicates the treatment can be considered equivalent. Majority of DVT were asymptomatic (2/38, 5.26% in Group 1 and 3/39, 7.69% in Group 2), identified only by ultrasound. A single case of non fatal PE was recorded in the short course therapy group (Group 1, 1/38, 2.63%) at the routine four week follow up after further investigation of a symptomatic DVT. There was a non significant group difference for PE between short course and standard therapy patients.
Device misuse of CCD2∞ resulting in propagation of DVT is a well described phenomenonen [12-15] and may account for this single case of PE rather than factors related to short course LMWH therapy. Additionally, current literature quotes an average incidence of 5% for symptomatic DVT, 0.5-1% for fatal PE, 1-3% for non fatal PE and upto 38% for asymptomatic DVT amongst post operative orthopedic patients whom are receiving anticoagulation in accordance with current major guidelines, (study sample sizes ranging from 4177 to 5738) [16-18]. Our findings of both symptomatic and asymptomatic DVT and PE (fatal and non-fatal) amongst post operative TKR patients receiving short course anti-coagulation therapy lie well within these indices.
Benefits of short course therapy distinct from DVT/VTE prophylaxis included significantly reduced leg swelling (5/38 group 1, 19/39 group 2, p=0.001) and shorter duration hospital stay, though the latter did not reach significance in this study (1/38 group 1, 2/39 group 2, p=1.000 Fisher’s exact test). Superiority in reducing post operative leg swelling is most likely due to the mechanical effects of the CCD in improving lymphatic and venous ‘milking’[19,20]. Reducing leg swelling amongst short course therapy patients further expedited mobilization and allowed for greater distances to be mobilized post operatively, both of which significantly reduce the development of DVT and related VTE [21,22] . Earlier ambulation in turn prevented cardio-respiratory complications such as pneumonia which are directly related to immobility and are one of the largest causes of prolonged hospitalization amongst orthopedic patients [23].
The difference in incidence of the remaining endpoints in the short course and standard therapy groups were not statistically significant. Exaggerated bleeding (defined clinically as larger than expected hematoma for recovery stage or need for transfusion Hb<90) and need for additional analgesia for intractable post operative pain were equal amongst groups (bleeding: 2/38 group 1 and 2/39 group 2; pain 8/38 group 1, 8/39 group 2, p=1.000, Fisher’s exact test). Superficial wound infection was marginally higher amongst the short course therapy group (3/38 group 1, 1/39 group 2, p=0.108 Fisher’s exact test.
Our findings support previous larger sample sized studies in which prolonged therapy with LMWH (greater than 7 days) was not associated with significant reductions in incidence of VTE, major bleeding or death compared with short course LMWH therapy (<7 days) amongst post operative patients including TKR [24,25]. A notable proportion of patients in these study cohorts displayed characteristics (such as age >61, arthroscopic surgery and BMI>25) that would place them at moderate to high risk of DVT/VTE according to existing major orthopedic guidelines [6,26,27].
In contrast, other studies presenting a focused evaluation of higher risk patients (i.e. entire cohort >61 years old and undergoing elective arthroplasty) reported significantly higher short term mortality secondary to VTE amongst patients who failed to continue with chemo-prophylaxis post discharge (mean discharge time being 7 days) compared with those who continued therapy for a minimum of ten-fourteen days (4.2% mortality vs. 0.7% mortality) [28]. Metaanalyses of nine randomized control trials have also demonstrated clear superiority of extended thromboprophylaxis (for 30-42 days postoperative) in achieving 51% risk reduction of venography confirmed DVT and 61% risk reduction in incidence of symptomatic VTE compared with short course therapy, though these studies focused on patients undergoing total hip replacement. Similar risk reductions have not been documented for persons undergoing TKR [29].
Current American College of Chest Physicians (ACCP) guidelines recommend patients undergoing TKR who are at low to moderate risk of DVT/VTE, use thromboprophylaxis with at least one of either LMWH for a minimum of ten-fourteen days or pneumatic calf compression, provided the latter technique is employed correctly [6] (i.e. proper application to the appropriate site as well as daily duration), thereby suggesting prolonged anti-coagulation with LMWH may be unnecessary in selected patients. Studies exclusively evaluating the efficacy of pneumatic calf compression against LMWH did not demonstrate significant differences in adverse events associated with each treatment modality (i.e. VTE with CCD and major bleeds with pharmacological agents) [6,30]. However, study bias, failure to specify treatment duration for calf compression and inconsistent symptom reporting from these trials encouraged current guidelines to favour LMWH [6]. The role of calf compression may therefore be more prominent in routine post-operative thromboprophylaxis than indicated by current guidelines.
This randomized study draws two major conclusions: (1) short course therapy of LMWH combined with 14 days of intermittent pneumatic calf compression is not inferior to standard 14 day therapy with LMWH in VTE prophylaxis amongst patients undergoing TKR and (2) extended use of mechanical compression with CCD (fourteen days) contributes to significantly lower rates of post operative leg swelling which in turn encourages early ambulation and hence further lowers the risk of DVT/VTE. Furthermore majority of patients in this study were at least moderate to high risk of DVT/VTE post operatively (i.e. 80% of patients were >65 years old) and rates of post-operative DVT and VTE remained statistically equivocal at twelve weeks follow up between treatment groups.
Other major benefits of anti-coagulation limiting regimes demonstrated in previous studies include a reduction in the overall risk of major post operative hemorrhage, reported to be as high as 4.2% (mortality >70%) in selected studies and even higher (8%) in patients with at least one other risk factor for hemorrhage (e.g. previous CVA) [31]. Short course LMWH regimes further provide significant cost reductions (30-40% cost reduction) by lowering pharmaceutical expenses and reducing the use of community services involved in drug administration (e.g. community nurses, GP, carers) [32,33].
Major limitations of this study include a small sample size and recruitment limited to a single institution; hence findings cannot be used in isolation to augment current practice. Replication using larger cohort sizes will increase equivalence power between treatment groups and present more reliable data. Additionally, presence of DVT was determined solely by US assessment which can be highly reporter dependent hence final results may be subject to external bias. Though venography has greater test specificity, its use in all patients was financially and practically unfeasible in this routine focused study. Inability to monitor compliance with CCD between follow up as well as purely subjective reporting of symptoms via phone interviews are other study imprecisions. Larger multicentre trials are needed to verify the findings from this trial. If proven successful, there may be scope for investigation into other anti-coagulant sparing regimes such as the use of anti-platelet therapy for patients with contra-indications to LMWH.
In this study short course therapy was equally effective as standard therapy in preventing DVT and non-fatal PE, and superior to standard therapy in limiting post-operative leg swelling amongst patients undergoing TKR. Additional advantages of shorter anti-coagulation regimes include lowered incidence of significant post-operative bleeding and considerable cost reductions (30-40%) associated with government funded pharmaceutical and community services. Non significant advantages in other criteria (such as lower incidence of prolonged hospitalization) were also demonstrated in the short course therapy group and these may reach significance in larger follow up multi-centre trials.
We would like to acknowledge funding support (non-pharmaceutical) from the Department of Veterans Affairs. We would also like to thank Dr Arvind Madras for assistance with clinical assessment and data collection and Ms Amanda Patracelli for assistance with trial co-ordination. Funding for all aspects of this study was provided by Dr Raj Ramakrishna and Southern Sydney Hematology.