Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2014) Volume 2, Issue 2
Purpose: Chronic Heart Failure (HF) is complicated by bone loss and osteoporosis, which have been linked to hyperparathyroidism. We studied the bone metabolism and possible role of cytokines in patients suffering from HF.
Methods and results: We measured bone alkaline phosphatase (BALP), C-telopeptides of type I collagen (β-CTx) and Interleukin-(IL) 6 in 60 men, 56 ± 11 years of age, suffering from chronic HF, and in 13 age-matched men free from HF. We also measured total body and femoral bone densitometry and parathyroid hormone (PTH). The β-CTx concentrations were significantly higher in men with than in men without HF. The concentrations of BALP (12.4 ± 4.9 vs. 9.9 ± 3 μg/l; P=0.03) and β-CTx (0.67 ± 0.35 vs. 0.33 ± 0.21 ng/ml; P<0.001) were significantly higher in patients in New York Heart Association (NYHA) functional classes III or IV than in patients in classes I or II. Moderately strong correlations were observed between β-CTx, BALP, PTH and bone densitometry measurements. Positive correlations were observed between NYHA functional classes and a) mean PTH (r2=0.19; P<0.001) and b) mean β-CTx (r2=0.30; P<0.001) concentrations. Moreover, increasing serum β-CTx and BALP concentrations were correlated with measurements consistent with decreasing bone mass and increasing severity of HF. IL-6 was also correlated with β-CTx, BALP and PTH, though not with measurements of bone density. Increased serum concentrations of IL-6 were correlated with the severity of HF. β-CTx was a strong predictor of adverse clinical events (hazard ratio 6.32; 95% confidence interval 1.8-22.5; P=0.005), including after controlling for other prognostic markers of chronic HF severity and measurements of bone densitometry.
Conclusion: Chronic HF, particularly at advanced stages, was associated with an acceleration of bone turnover and uncoupling of bone formation and resorption. These changes in bone metabolism, among others, could be due to secondary hyperparathyroidism and the chronic inflammatory state associated with chronic HF. The increased osteoclastic activity observed in chronic HF was associated with a poor prognosis.
<Keywords: Bone metabolism; Bone markers; Bone densitometry; Heart failure; Osteoporosis; Hyperparathyroidism
Chronic Heart Failure (HF) has recently been linked to an excessive loss of bone mass [1,2]. Furthermore, chronic HF is associated with an increased risk of bone fractures due to osteoporosis [3-6]. Hyperparathyroidism, hypogonadism, hypovitaminosis D, renal dysfunction, pharmaceuticals, physical inactivity and increased concentrations of inflammatory cytokines have all been incriminated in this disorder [1,2,7,8]. However, reports of abnormal bone metabolism in chronic HF are scarce [8,9].
Bone is a living tissue that undergoes continuous remodeling, a process which depends on bone resorption by osteoclasts on the one hand and bone formation by osteoblasts on the other. These mechanisms are tightly coupled in space and time [10]. Measurements of specific, circulating markers of bone resorption and formation, respectively released by osteoclasts and osteoblasts, reflect the overall timing of bone turnover and help defining the balance between these competing constituents of bone metabolism [11]. Uncoupling of bone resorption and formation occurs with aging and in chronic diseases. Chronic inflammatory diseases may stimulate the osteoclastic effects mediated by cytokines and inhibit the osteoblastic activity, uncoupling bone formation and resorption in favor of bone loss [12]. Moreover, the increased bone turnover is associated with exacerbation of bone loss leading to osteoporosis. It is particularly noteworthy that changes in bone markers reflect early changes in bone metabolism, which can be expressed later as measurable changes in bone mass [8]. Therefore, bone markers and the assessment of bone turnover reflect ongoing bone remodeling more accurately than measurements of bone mass and predict bone loss [8,13]. Chronic HF is a systemic disease, characterized by several metabolic abnormalities and by the stimulation of inflammatory pathways that are likely to involve bone tissue and bone metabolism.
The aim of this study was to examine the bone turnover and its association with disease severity in patients suffering from chronic HFrEF. We have previously shown that, in these patients, secondary hyperparathyroidism is an underlying pathophysiologic mechanism of chronic HF, and that the severity of the latter is correlated with the amount of bone mass loss [2]. In addition, the serum concentrations of Parathyroid Hormone (PTH) were correlated with the patients’ exercise capacity [14]. We hypothesized that secondary hyperparathyroidism is reflected in an increased bone turnover and uncoupling of bone formation and resorption, and that the up regulation of proosteoclastogenic cytokines is associated with the stimulation of bone resorption in patients suffering from chronic HF.
Between August 2007 and August 2009, we studied 31 men suffering from ischemic and 29 men suffering from dilated cardiomyopathy, who were followed in our chronic HF ambulatory department. The study inclusion criteria of the chronic HF group were 1) a ≥6-month history of chronic HF due to ischemic or idiopathic dilated cardiomyopathy, 2) a left ventricular (LV) ejection fraction <40% measured by echocardiography, 3) a stable clinical status and medication regimen for ≥1 month preceding enrollment in the study. We enrolled 13, age-matched, hypertensive men presenting with a ≥50% LV ejection fraction and no history or manifestation of HF in the no HF control group. The exclusion criteria from both groups were 1) a history of chronic, non-cardiac disease that may influence bone metabolism, including autoimmune diseases, cancer, multiple myeloma and other hematological malignancies, chronic obstructive pulmonary disease, advanced liver failure, hyperparathyroidism and Cushing syndrome, 2) renal dysfunction, defined as a serum creatinine concentration >2.5 mg/dl or treatment with long-term hemodialysis, and 3) current or previous administration of pharmaceuticals that may modify the bone metabolism, such as biphosphonates, calcitonin, estrogen glucocorticoids, vitamin D or calcium. The study protocol was approved by our institutional ethics committee and was performed according to the ethical standards of the declaration of Helsinki, and all study participants granted their written consent.
Total Body (TB) and Femur (F) Bone Mineral Density (BMD), and femoral T- and Z-scores were measured in both groups, using a DPX-MD dual energy X-ray absorptiometry scan (Lunar Corporation, Madison, WI). The measurements of serum PTH and vitamin D concentrations, as well as BMD measurements in all patients, were published recently (2). The same venous blood samples were used to measure the markers of bone metabolism in the present study. More specifically, the osteoblastic component of bone metabolism was measured, using bone specific alkakine phosphatase (BALP) and an enzyme-linked immunosorbent assay (Immunodiagnostic Systems Limited, Bold on, UK) and the Ostase® BAP EIA kit. The normal range for this assay was 7-20 μg/l. To measure the osteoclastic activity, we used a chemiluminescence immunometric assay to measure the serum concentrations of C-telopeptides of type I collagen (β-CTx) with a Modular E170 analyzer (Roche, Diagnostics, Mannheim, Germany) and the β-Cross Laps® serum kit. The normal range for this assay was 0.3 ± 0.6 ng/ml. BALP and β-CTx are markers of bone formation and resorption, respectively, which accurately reflect the anabolic and catabolic activity of bone metabolism [15,16]. We also measured the serum concentrations of high-sensitivity interleukin-(IL)6, using the ultrasensitive, solid phase, Quantikine®, “sandwich” enzyme-linked immunosorbent assay (R&D Systems, Abingdon,UK). The normal range for concentrations of IL-6 was 0.38-10.1 pg/ml (intra assay coefficient variation 5.9% in the limit of 2.73 pg/ml, and 16.5% in the limit of 3.58 pg/ml). IL-6 is one of the cytokines involved in the pathophysiology of chronic HF and known to promote the formation of osteoclasts [17,18].
| Chronic HFrEF (n=60) |
Controls (n=13) |
|
|---|---|---|
| Age, y | 57 ± 11 | 57 ± 10 |
| Body mass index, kg/m2 | 27.7 ± 4.3 | 28.1 ± 3.3 |
| New York Heart Association functional class I II III IV |
15 15 16 14 |
Not applicable Not applicable Not applicable Not applicable |
| Left ventricular ejection fraction, % | 26 ± 6 | 59 ± 4* |
| Serum concentrations Creatinine, mg/dl Calcium, mg/dl Phosphorus, mg/dl Thyroid-stimulating hormone, mIU/ml |
1.2 ± 0.3 9.2 ± 0.6 3.4 ± 0.5 2.6 ± 1.6 |
0.8 ± 0.2* 9.3 ± 0.5 2.8 ± 0.5* 2.4 ± 0.4 |
Values are means ± standard deviation or numbers of observations.
*P<0.05; all other between-groups comparisons are statistically non-significant.
Table 1: Baseline characteristics of the study groups.
Cardiovascular evaluation
The New York Heart Association (NYHA) functional class was estimated at the time of initial evaluation. All study participants underwent transthoracic echocardiography. Cardiac catheterization was performed in 54 patients at the time of initial evaluation, while on an optimal medical regimen, for measurements of hemodynamic function, including pulmonary capillary wedge pressure. Exercise capacity was measured by the mean oxygen consumption (VO2) in the last 20 sec of symptom-limited exercise on a ramp, incremental treadmill. Brain natriuretic peptide (BNP) was measured using a Triage® analyser (BIOSITE, San Diego, CA). The upper normal limit of this assay is 99 pg/ml
Study endpoints
The primary composite endpoint of the study was death, implantation of a LV assist device, or the long-term administration of inotropes. The endpoint was ascertained at each follow-up visit.
Statistical analysis
Continuous variables are expressed as means ± SD (median). Distribution normality was assessed using the Kolmogorov-Smirrnov test. An independent-samples t-test (or Mann-Whitney test for variables that were not distributed normally) was used for betweengroups comparisons of continuous variables. Correlations between variables were examined, using Pearson’s correlation coefficient (or Spearman’s for variables not distributed normally). The prognostic significance of variables was tested by Cox regression analysis, and hazard ratios (HR) and 95% Confidence Intervals (CI) were calculated. For all tests, a two-sided P-value<0.05 was considered significant. The SPSS software, version 17.0 (SPSS Inc., Chicago, IL) was used for all statistical computations.
The chronic HF group comprised 31 men presenting with ischemic and 29 with dilated cardiomyopathy with reduced ejection fraction, while the control group included 13 hypertensive men with preserved LV function. The median length of follow-up was 2 years. The baseline clinical and laboratory characteristics of the two groups are shown in Table 1. The patients suffering from chronic HF were subdivided into a mild to moderate (NYHA functional classes I-II) and an advanced to severe (NYHA functional classes III-IV) HF group, whose cardiovascular indices were significantly different [2].
Bone markers in chronic heart failure
The mean concentration of β-CTx was significantly higher in patients with chronic HF than in controls; likewise, the mean concentration of BALP was higher in patients with chronic HF, though the difference did not reach statistical significance (Table 2). Moreover, the mean concentrations of β-CTx and BALP were significantly higher in patients with advanced or severe HF than in patients in NYHA functional classes I or II (Table 3).
| Chronic HFrEF (n=60) |
Controls (n=13) |
P | |
|---|---|---|---|
| C-telopeptides of type I collagen, ng/ml Bone alkaline phosphatase, µg/l Interleukin-6, pg/ml |
0.499 ± 0.333 11.2 ± 4 5.219 ± 5.868 |
0.253 ± 0.134 9.6 ± 2 1.354 ± 0.824 |
0.01 0.08 0.02 |
Values are means ± standard deviation.
Table 2: Serum concentrations of bone markers and interleukin-6 in patients with
chronic heart failure versus controls.
| NYHA I-II (n=30) |
NYHA III-IV (n=30) |
P | |
|---|---|---|---|
| C-telopeptides of type I collagen, ng/ml Bone alkaline phosphatase, µg/L Interleukin-6, pg/ml |
0.333 ± 0.208 9.9 ± 3 4.811 ± 6.578 |
0.665 ± 0.354 12.4 ± 4.9 5.627 ± 5.143 |
<0.001 0.03 NS |
Table 3: Serum concentrations of bone markers and interleukin-6 in patients with mild or moderate versus advanced or severe chronic heart failure.
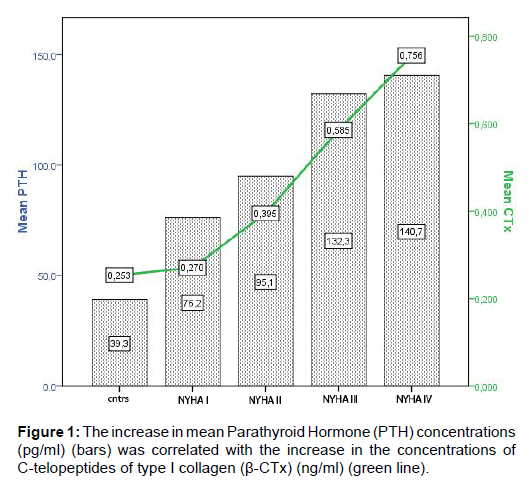
Figure 1:The increase in mean Parathyroid Hormone (PTH) concentrations (pg/ml) (bars) was correlated with the increase in the concentrations of C-telopeptides of type I collagen (ß-CTx) (ng/ml) (green line).
In the group of patients presenting with HFrEF, the osteoclastic (β-CTx) activity was positively correlated with the osteoblastic (BALP) activity (r2=0.19; P=0.001) and with hyperparathyroidism (r2=0.19; P=0.001; Figure 1). Figure 1 also illustrates the positive correlations we observed between NYHA functional classes from 0 (control group) to IV (severe HF) and a) mean PTH (r2=0.19; P<0.001) and b) mean β-CTx (r2=0.30; P<0.001) concentrations. Figure 2 shows the a) negative correlation between mean β-CTx concentrations and the decrease in mean femoral T- score (r2=0.10; P=0.01), b) negative correlation between the increase in NYHA functional class from 0 to IV and mean femoral T-score (r2=0.20; P=0.001). We also found correlations between increasing β-CTx concentrations and a) decreasing bone mass expressed as TBBMD (r2=0.06; P=0.03) and FBMD (r2=0.08; P=0.03), and b) indices of chronic HF severity, including increasing serum concentrations of BNP (r2=0.29, P=0.0001) and pulmonary capillary wedge pressure (r2=0.37, P=0.0001; Figure 3), and decreasing LV ejection fraction (r2=0.10, P=0.01) and peak VO2 (r2=0.19, P=0.001).
The serum concentrations of BALP were weakly correlated with the serum concentrations of PTH (r2=0.08; P=0.01). BALP was also positively correlated with indices of bone density, including TBBMD (r2=0.08; P=0.01), FBMD (r2=0.15; P=0.001), femoral T-score (r2=0.14; P=0.003) and Z-score (r2=0.17; P=0.001). Finally, changes in BALP were correlated with NYHA functional class (r2=0.10; P=0.02) and with pulmonary capillary wedge pressure (r2=0.10; P=0.02).
Interleukin-6 in bone metabolism and heart failure
The serum concentrations of proinflammatory cytokine, IL-6, were correlated with the concentrations of β-CTx (r2=0.16; P=0.0001), BALP (r2=0.08; P=0.01) and PTH (r2=0.32; P=0.006), though not with the BMD measurements. The increase in IL-6 observed in the patients suffering from chronic HF was correlated with NYHA functional classes (r2=0.26; P<0.001), decrease in peak VO2 (r2=0.24; P<0.001), BNP concentrations (r2=0.27; P<0.001) and pulmonary capillary wedge pressure (r2=0.15; P=0.004), and weakly correlated with LV ejection fraction (r2=0.06; P=0.05).
Markers of bone turnover and clinical outcomes
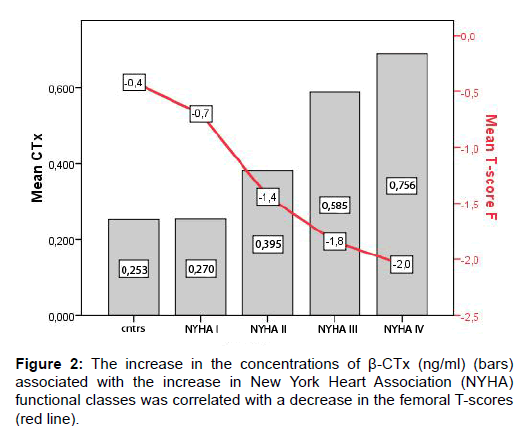
Figure 2:The increase in the concentrations of ß-CTx (ng/ml) (bars) associated with the increase in New York Heart Association (NYHA) functional classes was correlated with a decrease in the femoral T-scores (red line).
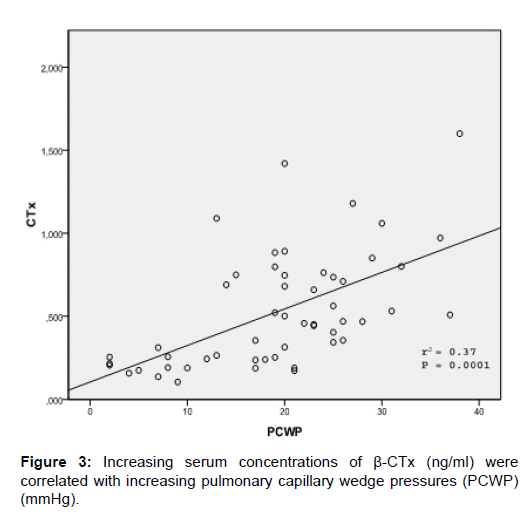
Figure 3:Increasing serum concentrations of ß-CTx (ng/ml) were correlated with increasing pulmonary capillary wedge pressures (PCWP) (mmHg).
During the 2-year follow up, 11 patients died, 5 became inotropedependent, and 3 underwent implantation of LV assist devices [2]. By Cox regression analysis, a high concentration of β-CTx was a strong predictor of adverse clinical events (HR 6.3; 95% CI 1.8-22.5; P=0.005). When entered in a bivariate Cox regression analysis, β-CTx retained its prognostic value, along with well established prognostic markers of cardiac function, such as LV ejection fraction (HR 5.3; 95% CI 1.3-21.2; P=0.02), peak VO2 (HR 5.0; 95% CI 1.2-20.6; P=0.02), BNP (HR 5.6; 95% CI 1.3-23.6; P=0.02) and cardiac index (HR 6.7; 95% CI 1.6-28.2; P=0.01). β-CTx retained its prognostic value in a bivariate analysis with TBBMD (HR 5.85; 95% CI 1.6-21.2; P=0.007) and femoral Z score (HR 6.54; 95% CI 1.3-33.8; P=0.02), which have been recently found to be prognostic factors in the same patient population [2].
The main observations made in this study were 1) in patients suffering from chronic HFrEF, the bone turnover was up-regulated and, since the increase in osteoclastic activity exceeded that in osteoblastic activity, the resorption and formation of bone was uncoupled, 2) the predominant increase in catabolic bone turnover was associated with a clinical deterioration and worsening of the laboratory indices of HF, 3) secondary hyperparathyroidism and increased concentrations of IL-6 were associated with enhanced osteoclastic and osteoblastic activities, 4) the increased bone turnover accelerated bone loss, measured by TBBMD, FBMD and femoral T- and Z-scores, and 5) increased concentrations of β-CTx were associated with increased morbidity and mortality.
Bone remodeling is a life long coordinated interaction between osteoclastic resorption of old and osteoblastic formation of new bone. These two closely coupled processes renew and preserve the mechanical properties of the skeleton [19]. However, aging, chronic diseases, inflammatory cytokines, under nutrition, inactivity, pharmaceuticals, and endocrine and renal disorders may negatively interfere with bone metabolism and the coupling of these two processes, decreasing the total amount of bone and increasing the risk of fractures [12,20]. Few studies have examined the disturbances caused in the bone microenvironment by chronic HF. Markers of bone metabolism may detect these disturbances at an early stage, predict future bone loss and enable the application of preventive measures before the development of osteoporotic fractures [8]. This study has shown for the first time the existence of an increased bone turnover and uncoupling of the osteoclast-osteoblast activities in chronic HFrEF. These mechanisms can both increase bone loss and promote osteoporosis. Our study provides insights into the pathophysiologic mechanisms behind these derangements. Continuously, as opposed to intermittently elevated concentrations of PTH, as observed in secondary hyperparathyroidism, accelerate the bone turn over and, in particular, the resorptive activity of osteoclasts [21]. In our study the stimulation of osteoclasts was not followed by a similar increase in osteoblastic activity; at the same time, osteoclastic activity exhibited stronger correlation with PTH concentrations. PTH promotes the recruitment and differentiation of osteoclast precursors and inhibits the synthesis of collagen and the osteoblastic cell cycle via locally produced factors and cytokines, such as the macrophage colony stimulating factor, tumor necrosis factor (TNF)-α, IL-1 and IL-6, and via the osteoprotegerin/receptor activator of nuclear factor - κB ligant system [22]. Secondary hyperparathyroidism in chronic HF seems to disrupt the cross-talk between osteoclasts and osteoblasts, ultimately resulting in bone resorption.
Inflammatory cytokines may also alter the bone metabolism. TNF-α, IL-1β, IL-6, IL-11 and IL-17 stimulate the genesis of osteoclasts, whereas interferon-γ, IL-4 and transforming growth factor-β are predominantly inhibitors [18,21]. IL-6 and TNFα are increased in chronic HF and inflammation might play an important role in its development and progression (“cytokine hypothesis”) [17,23]. In our study, the concentrations of IL-6 were increased in patients suffering from chronic HFrEF and were correlated with markers of bone turnover. Therefore, in this inflammatory state, the resorption of bone may be promoted by pro-osteoclastogenic cytokines. We also found a strong association between IL-6 and PTH. The latter promotes the resorption of bone, at least in part by inducing osteoblasts to secrete cytokines, for example IL-6, which stimulate the differentiation and activate osteoclasts [24]. Hence, IL-6 acts as a mediator in the bone resorptive cascade induced by PTH, and the increased concentrations of IL-6 could be due, in part, to hyperparathyroidism.
We also found that both bone markers, β-CTx in particular, were correlated with the severity of HF and with the decrease in BMD. As mentioned earlier, these bone markers, which accurately reflect early changes in bone metabolism, can be used to predict future bone loss. Previous studies have shown the propensity of patients suffering from heart failure to sustain bone fractures [3-6]. Therefore, these markers might be of great help in the early identification of patients at high risk of developing osteoporosis and in the implementation of preventive measures [3,6]. Finally, we identified the predictive value of the osteoclastic marker β-CTx, high concentrations of which were strongly correlated with high morbidity and mortality. It is well known that serum CTx levels could be affected by decreased kidney function. However, in our study β-CTx retained its prognostic significance, even when creatinine entered in the Cox-regression analysis. To the best of our knowledge, it is the first marker of bone metabolism identified as a prognostic factor in chronic HF. Serum β-CTx is easily measured and could be included in the overall assessment of chronic HF, as a prognostic tool and for the early identification of patients at risk of osteoporosis.
This single-center study enrolled a relatively small number of men exclusively. Our observations need to be confirmed in a larger, ethnically more diverse, multicenter study, including both genders and several age groups. This sample of men <60 years of age lacked 2 major contributors to the development of osteoporosis that are old age and the post-menopausal state. These characteristics, therefore, did not confound the correlations we found between chronic HF and bone metabolism. While the control group was also relatively small, the main study objective was to examine the relationship between changes in bone tissue and severity of chronic HF. Finally, our analyses of bone markers were not controlled for known circadian, monthly and circ annual variations in biomarkers of bone turnover [25,26].
In conclusion, chronic HFrEF, particularly in advanced stages, was associated with an accelerated bone turnover and uncoupling of the bone resorption/formation processes. Secondary hyperparathyroidism and chronic inflammation seem to be the underlying pathophysiologic mechanisms behind the changes in bone metabolism observed in chronic HFrEF. A reduced bone mass is the most likely net result of increased bone turnover, of the catabolic phase in particular. Bone markers may be used to identify at an early stage the patients suffering from chronic HFrEF, whose prognosis is poor and who are at high risk of osteoporosis.