Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2012) Volume 2, Issue 1
Background:Although postoperative atrial fibrillation (AF) is prevalent after cardiac surgery, the corresponding medication burden associated with this postoperative arrhythmia is unknown.
Methods: We conducted a prospective study of 204 patients aged 60 or older (median age 73) undergoing cardiac surgery at two academic medical centers. We defined “AF at discharge” as AF that developed after surgery and was present on the day of discharge. We evaluated the prevalence of anticoagulant and antiarrhythmic use at discharge, and out to 1 year post-discharge. We investigated the association between age and prescription of both classes of medications at discharge.
Results: Ninety-one (45%) patients developed new postoperative AF, which persisted at discharge in 28 (14%) patients. Thirty-four percent of patients with postoperative AF were discharged on warfarin, 62% were discharged on antiarrhythmic medication, and 25% were discharged on both. Eighty-two percent of those discharged on both were older than 72 years of age. Patients with AF present at discharge were more likely to be discharged on anticoagulant agents than patients whose AF resolved prior to discharge (54% versus 26%, p=0.01), and more likely to be discharged on antiarrhythmic agents than patients whose AF resolved prior to discharge, though not significantly so (73% versus 57%, p=0.2). At 12 months, the proportion of patients on antiarrhythmic and anticoagulant medications had still not returned to preoperative rates.
Conclusions:AF persists at hospital discharge in nearly one-third of affected patients. Cardiac surgery results in the initiation of anticoagulant and antiarrhythmic medications in many older patients annually, often concurrently. Our findings underscore the need for additional studies on the natural history of this arrhythmia and clinical trials investigating different management strategies after discharge. Such research will help to inform development of guidelines addressing duration of use for these medications, to aid physicians in these complicated post-discharge management decisions
Keywords: Atrial fibrillation; Cardiac surgery; Anticoagulants; Antiarrhythmia agents
AF: Atrial Fibrillation
Despite advances in prophylactic regimens, postoperative atrial tachyarrhythmias remain a common problem after cardiac surgery. Estimated incidence rates range from 20-50% after coronary artery bypass graft procedures, to even higher rates after valvular procedures, making this the most common postoperative complication [1-5].
While atrial fibrillation is a risk factor for increased length of stay and hospital cost [2-4,6,7], the most devastating complication associated with atrial fibrillation is stroke. Prior studies have demonstrated a twoto four-fold increased risk of stroke in patients with postoperative atrial fibrillation [6,8-11]. Accordingly, consensus guidelines recommend considering use of warfarin in patients with postoperative atrial fibrillation that lasts more than 48 hours [12]. Additionally, on the basis of several large randomized controlled trials demonstrating a significant reduction in postoperative atrial tachyarrhythmias with the use of perioperative amiodarone [13-15], use of this medication has increased. The use of both anticoagulant and antiarrhythmic medications is not without risk, and could be associated with significant morbidity in older patients [16]. Unfortunately, guidelines addressing duration of use for these agents are lacking. Furthermore, although postoperative atrial fibrillation is generally thought to be a transient phenomenon, surprisingly few studies have examined the natural history of this post-operative arrhythmia [17-20]. Physicians must therefore make important decisions about use of potentially harmful medications in the absence of clear guidelines, and limited information on the natural history of this rhythm after hospital discharge.
To our knowledge, there are no studies assessing utilization of these medications in a post-cardiac surgery cohort, or the impact of age and/or atrial fibrillation presence on the day of discharge on medication decisions. In the present study, we sought to define the incidence of postoperative atrial fibrillation persisting on the day of hospital discharge, thereby identifying a group of patients who would warrant consideration of anticoagulant and antiarrhythmic agents, and to assess utilization of these medications at discharge and at several post-discharge time points out to one year.
Participants and data collection
This is a substudy of a study designed to investigate cognitive outcomes in patients undergoing cardiac surgery [21]. Patients aged 60 or older undergoing coronary artery bypass surgery (CABG), valve surgery (aortic or mitral), or a combination of the two procedures at two major academic medical centers from August 1st, 2002 to June 30th, 2006 were eligible for inclusion. All patients provided written informed consent. Exclusion criteria included living more than 60 miles from the medical center, medical instability that would limit preoperative assessment, additional surgical procedures (including the MAZE procedure), and inability to speak English. Patients whose surgery was canceled or who were found to be delirious on preoperative assessment were also excluded. All patients underwent routine admission electrocardiogram. In order to measure the incidence of new postoperative atrial fibrillation, patients in atrial fibrillation on their admission electrocardiogram were excluded; patients with a history of atrial fibrillation, but who were in sinus rhythm on their admission electrocardiogram, were included. The study was approved by the Institutional Review Board at each institution. Data were collected prospectively via patient interview and comprehensive medical record review performed by an experienced clinician.
Atrial fibrillation outcomes
Postoperatively, all patients were monitored for arrhythmia via telemetry until hospital discharge. We defined postoperative atrial fibrillation as new onset atrial fibrillation occurring at any point postoperatively prior to hospital discharge. “Resolved atrial fibrillation” was defined as new onset postoperative atrial fibrillation that had resolved by discharge. “Atrial fibrillation at discharge” was defined as new onset postoperative atrial fibrillation that had not resolved by the time of hospital discharge. Rhythm was assessed daily via comprehensive chart review, including telemetry strips, electrocardiograms, and physician notes when available.
Medication utilization
To investigate medical practice surrounding postoperative atrial fibrillation, we recorded medications prescribed on discharge via chart review. To investigate the longer-term medication utilization associated with postoperative atrial fibrillation we recorded medications prescribed at two post-discharge time points – 1-3 months and 12 months. Medication use was assessed via patient interview during home visits. Patient self-report was then confirmed by direct review of the pill bottles in the home setting.
Antiarrhythmic medication was defined as amiodarone, sotalol, propafenone, procainamide, dofetilide, flecainide, disopyramide, and quinidine. For anticoagulant therapy, enoxaparin and fondaparinux were not utilized in our cohort; therefore, we simplified our definition to refer only to warfarin.
For the 1-3 month time frame, we used one month medication data preferentially, and substituted 3 month data in patients for whom 1 month medication data was unavailable (n = 20).
Statistical analysis
The proportion of patients with any new postoperative atrial fibrillation and the proportion with this rhythm present on the day of discharge were analyzed descriptively; 95% confidence intervals for all proportions were calculated using a 2-sided type-1 error of 0.05.
We report the proportion of patients on warfarin and antiarrhythmic medication at hospital discharge stratified by atrial fibrillation status at discharge (no atrial fibrillation, resolved atrial fibrillation, atrial fibrillation at discharge). We investigated the association between age - dichotomized at the median - and prescription of both classes of medications at the time of discharge in patients with postoperative atrial fibrillation using the Fisher’s Exact Test.
For the follow up analysis, we describe the proportion of patients on warfarin and antiarrhythmic medication at the time of hospital discharge, at 1-3 months, and at 12 months, also stratified by atrial fibrillation status at discharge. Patients who died prior to discharge were excluded from the medication analysis. Patients started on warfarin or antiarrhythmic medication for reasons other than atrial fibrillation at the time of discharge were also excluded from the medication analysis.
Sample characteristics and prevalence of atrial fibrillation
Figure 1 describes the screening, eligibility, enrollment, and follow-up experience of our study cohort. The table 1 describes the characteristics of the study participants. Out of 204 patients, 91 (45%) developed new postoperative atrial fibrillation (95% CI 38% to 51%). In 28 patients, atrial fibrillation persisted at the time of hospital discharge, constituting 31% of patients with any atrial fibrillation (95% CI 22% to 41%) and 14% of the total sample (95% CI 10% to 19%)
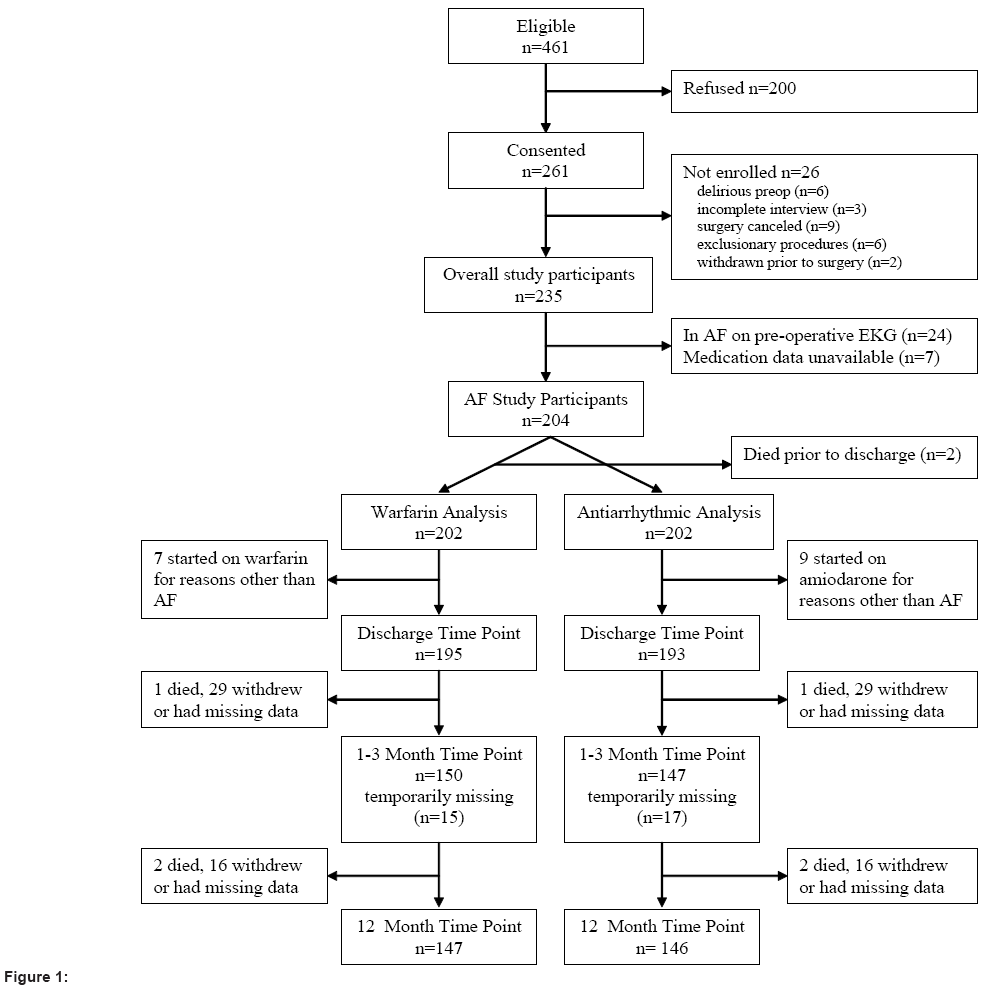
Figure 1
| Overall (n = 204) | |
| Demographics: | -- |
| Age – median (range), years | 73 (60-89) |
| Male sex – n (%) | 158 (77) |
| BMI – median (range), kg/m2 | 27 (18-47) |
| Comorbidities – n (%): | -- |
| History of AF | 19 (9) |
| Congestive heart failure | 36 (18) |
| Hypertension | 174 (86) |
| Diabetes | 86 (42) |
| Chronic Lung Disease | 36 (18) |
| Type of Procedure – n (%): | -- |
| CABG | 163 (80) |
| Valve repair or replacement ± CABG | 41 (20) |
| Operative Data: | -- |
| Cardiac bypass used – n (%) | 197 (97) |
| Bypass duration – median (range), min | 87 (0-261) |
| Aortic Cross Clamp time – median (range), min | 62 (0-202) |
Table 1: Overall Cohort Characteristics.
Medication utilization
After excluding patients who died prior to discharge (n=2), 84 out of 202 patients (42%) in the study received an antiarrhythmic at some point during their hospitalization, of which 83 were on amiodarone. Prior to hospital admission, 3 patients (1%) were on antiarrhythmic medication. After excluding patients started on antiarrhythmics for reasons other than atrial fibrillation, at hospital discharge this number increased to 57 (30%). Overall, 54 out of 87 (62%) patients with postoperative atrial fibrillation were discharged on antiarrhythmic medication, including 35 out of 61 patients (57%) with resolved postoperative atrial fibrillation and 19 out of 26 patients (73%) with atrial fibrillation present at discharge. Utilization rates of antiarrhythmic medication on discharge in patients with postoperative atrial fibrillation were unrelated to age, with 18 out of 26 (69%) patients ≤ 72 years of age, and 36 out of 61 (59%) patients > 72 years of age receiving antiarrhythmic medication on discharge (p=0.47)
Prior to hospital admission, 5 patients (3%) were on warfarin; after excluding patients started on warfarin for reasons other than atrial fibrillation, at hospital discharge this number increased to 31 (16%). Overall, 30 out of 87 (34%) patients with postoperative atrial fibrillation were discharged on warfarin, including 16 out of 61 patients (26%) with resolved postoperative atrial fibrillation, and 14 out of 26 patients (54%) with atrial fibrillation present at discharge. Patients > 72 years of age with postoperative atrial fibrillation were more likely to receive anticoagulant medication on discharge than patients ≤ 72 years of age with postoperative atrial fibrillation (26 out of 61 [43%] versus 4 out of 26 [15%]; p = 0.02). Twenty-two patients of the 87 (25%) patients with postoperative atrial fibrillation were discharged on both warfarin and antiarrhythmic medication, 18 of which were > 72 years of age.
Figure 2 reports rates of anticoagulant and antiarrhythmic medication use at various subsequent time points. At 1-3 months, 26 (17%) patients were still on warfarin, and 23 (16%) patients were still on antiarrhythmic medication. At twelve months, the percentage of patients on these medications had still not returned to baseline; 15 (10%) patients were still on warfarin and 6 (4%) patients were still on antiarrhythmics. At each follow-up time point, patients with atrial fibrillation at discharge had the highest rates of use of both anticoagulants and antiarrhythmics.
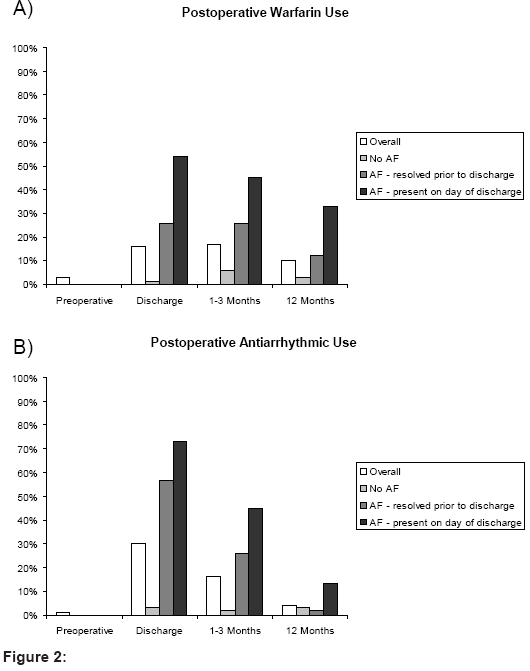
Figure 2
Atrial fibrillation remains a highly prevalent complication after cardiac surgery, occurring in 45% of this cohort of older patients from 2 academic medical centers and persisting at the time of discharge in 31% of these patients. The observed rates of anticoagulant and antiarrhythmic medication utilization on discharge illustrate the substantial long-term treatments and costs associated with this postoperative complication. Our finding that 25 percent of patients with postoperative atrial fibrillation were discharged on both warfarin and an antiarrhythmic agent, the majority of whom were older than 72 years of age, further underscores the need for clear, evidencebased recommendations surrounding duration of use and monitoring of patients on these medications. Taken together, our findings draw attention to the great need for additional research on the natural history of this arrhythmia and clinical trials examining different management strategies after discharge, to inform decision analyses weighing the risks and benefits of medical treatment of this arrhythmia, especially for older patients in whom both the benefits and risks of treatment may be greater.
Our finding that 62% of patients with postoperative atrial fibrillation were discharged on antiarrhythmic medication, and that older patients were as likely as younger patients to receive such treatment has important implications. With the success of amiodarone at preventing postoperative atrial fibrillation when used prophylactically [22,23], and with increased comfort surrounding its use, it is not surprising that amiodarone is commonly used in this patient population. However, amiodarone is not without risk in older patients, who were as likely as younger patients to be prescribed antiarrhythmic medication at the time of discharge. Increased fat mass with aging can prolong the halflife of lipophilic drugs such as amiodarone, potentially increasing the risk for cardiac and non-cardiac side effects [16,24]. The 2003 update of the Beers criteria for potentially inappropriate medication use in older adults added amiodarone to the list of medications to avoid [25,26]. Even more concerning is our finding that of the 22 patients discharged on both warfarin and an antiarrhythmic agent, 18 were older than 72 years of age. Amiodarone may enhance the anticoagulant effect of warfarin, representing a clinically important drug-drug interaction, particularly for elderly patients in whom pharmacokinetics and pharmacodynamics of drugs are already altered due to a multitude of factors.
Unfortunately, older patients are also at higher risk for stroke [10,27], as well as complications related to anticoagulation, making decisions surrounding these postoperative medical treatments even more complicated [28-30]. Our findings draw attention to the great need for large prospective studies and clinical trials to help inform decision making in this realm. More specifically, while postoperative atrial fibrillation is generally thought to be a transient phenomenon, few studies have actually examined the natural history of postoperative atrial fibrillation after discharge [17-20], and none have examined the efficacy of postoperative amiodarone at restoring or maintaining sinus rhythm after discharge – both crucial pieces of the risk-benefit analysis. Additionally, there is little guidance related to possible testing to be performed before discontinuation of warfarin or amiodarone, such as an in-office electrocardiogram or holter monitoring. In our study, use of warfarin and antiarrhythmic medication at 1-3 months and 12 months after surgery still had not returned to pre-operative levels. This finding warrants further investigation in a sufficiently powered study aimed at elucidating whether this represents persistence of the rhythm, new onset or recurrence of atrial fibrillation, or failure of outpatient medication reconciliation. Our findings underscore the need for clinical trials in this area to guide formal recommendations surrounding use and duration of use for these medications.
Our study has several strengths, including the multi-site prospective design, and the detailed medical record review supplemented by patient interview and home visits. There are also several limitations. First, the relatively small sample size limited our statistical power and ability to investigate outcomes associated with atrial fibrillation, such as stroke. Second, our lack of data on rhythm status after discharge prevented us from drawing conclusions related to the appropriateness of medication utilization at post-discharge time points. Finally, studies demonstrating the effectiveness of amiodarone at decreasing the incidence of postoperative atrial fibrillation were largely published towards the end of our study period. Thus, the current rate of antiarrhythmic use may be underestimated, further emphasizing the need for formal recommendations addressing duration of use.
In conclusion, consistent with prior studies, we found that atrial fibrillation is common after cardiac surgery, and persisted at the time of hospital discharge in nearly one-third of those affected. The substantial utilization rates of anticoagulant and antiarrhythmic medications at the time of discharge in this older patient population draw attention to the need for further studies on the natural history of this arrhythmia and clinical trials examining different management strategies after discharge. Such research is imperative for development of guidelines for tailoring medical management of this common postoperative complication, especially for older patients in whom both the benefits and risks of treatment may be greater.
Competing interests
None of the authors have any financial or non-financial competing interests.
Authors’ contributions
SJH developed the concept/design of the study, analyzed and interpreted the data, drafted the manuscript, and gave final approval of the submitted manuscript. JLR participated in the concept/design of the study, collected the data, performed critical revision of the manuscript, and gave final approval of the submitted manuscript. MH interpreted the data, performed critical revision of the manuscript, and gave final approval of the submitted manuscript. LHN analyzed and interpreted the data, performed critical revision of the manuscript, and gave final approval of the submitted manuscript. ERM developed the concept/design of the study, collected and interpreted the data, performed critical revision of the manuscript, and gave final approval of the submitted manuscript.
Funding
This study was funded in part by grant number T32HP11001 from the Health Resources and Services Administration of the Department of Health and Human Services to support the Harvard Medical School Fellowship in General Medicine and Primary Care, and in part by the following grants from the National Institute on Aging: P60AG008812 (the Harvard Older Americans Independence Center), R01AG030618 and R03AG028189. Dr. Marcantonio is supported by a Midcareer Investigator Award in Patient-Oriented Research from the National Institute on Aging (K24AG035075). Dr. Rudolph is funded by a VA Rehabilitation Research Career Development Award. Dr. Ngo is funded by grant number 1 UL1 RR025758- 01 from the National Center for Research Resources to support the Harvard Clinical and Translational Science Center. The funding organizations had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.