Journal of Bone Research
Open Access
ISSN: 2572-4916
ISSN: 2572-4916
Review Article - (2018) Volume 6, Issue 1
Objectives: To consolidate the current literature and find the evidence of any advantages of the use of the above mentioned techniques and also to emphasize the need for well-designed studies to evaluate long- and short-term function and risk of posttraumatic osteoarthritis in arthroscopically-assisted treated patients.
Background: The role of arthroscopy in the fixation of tibial plateau fractures has been advocated in the literature in the last decades. A number of papers have been published regarding Arthroscopically Assisted Internal Fixation (mainly) and Arthroscopically Assisted External Fixation (significantly smaller amount of papers) of tibial plateau fractures.
Materials and Methods: 29 studies including 983 patients were identified via Pubmed search. Most of them are small studies, poorly controlled and with potential bias.
Results: Despite the small amount of studies comparing ARIF with ORIF technique and studies with an average follow up longer than 3 years), the advocates of ARIF suggest, that this technique can have a key role in the management of tibial plateau fractures and is the treatment of choice for associated intra-articular pathology. Nevertheless, most of these studies, if not all, are selected, small studies, poorly controlled and with potential bias.
Conclusions: There is a need for well-designed studies to evaluate long- and short-term function and risk of posttraumatic osteoarthritis in arthroscopically-assisted treated patients.
Keywords: Arthroscopy; Arthroscopically-assisted reduction; Soft tissue injury; Tibial plateau fracture treatment
Tibial plateau fractures have always been a challenge for orthopaedic surgeons. Cast immobilization, skeletal traction and Open Reduction and Internal Fixation (ORIF) have been among the preferred treatment methods traditionally. Arthroscopic joint surgery has evolved dramatically in the last decades and nowadays arthroscopically assisted internal fixation (ARIF) is considered to be a very attractive option among the available surgical treatments. It was first introduced by Reiner, McGlynn and Jennings in 1980s [1-4] and was proven effective in the treatment of Schatzker 1,2 and 3 fractures with decreased morbidity rates compared to ORIF. In Schatzker 5 and 6 fractures, the use of arthroscopy seems to improve the quality of reduction, making an extensive arthrotomy unnecessary [1,5]. We present a systematic review of the studies concerning the use of arthroscopy-assisted surgery for the treatment of tibial plateau fractures.
Tibial plateau fractures are relatively rare fractures, representing approximately 1% of all fractures in adults [6-8] and may be difficult to manage. They may be related to high-energy trauma –especially in young people with good bone density- or mild traumatic injury (in elderly individuals with osteoporotic bones). Tibial plateau fractures are bicondylar in 30-35% and unicondylar in 60% of cases, usually involving the lateral tibial plateau (90%). Fractures of the intercondylar eminence represent a 10% of cases [1]. Approximately 5% to 10% of these fractures are related to sports [9], such as skiing [10].
Cubin & Conley in 1934, Marchant in 1939, Duparc & Ficat in 1960 and Hohl & Moore in 1990 developed classification systems for these fractures [1,7,11]. The most widely used classification system in our days is developed by Schatzker (Figure 1) [1]. Its simplicity has made this classification system very popular compared to the Duparc-Ficat classification system and the -too complex to be suitable for every day practice- AO classification system [12,13].
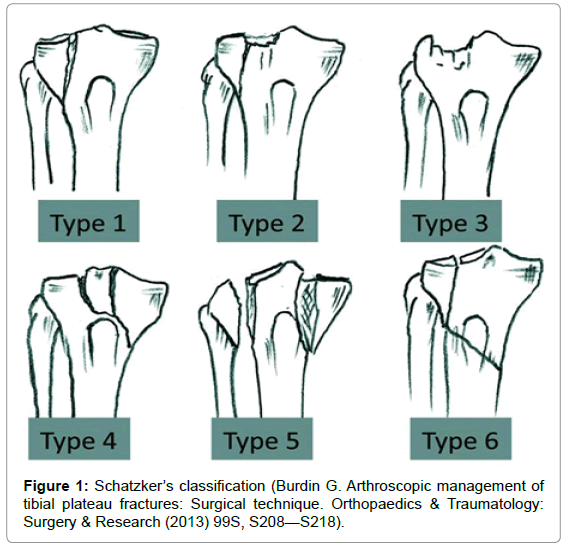
Figure 1: Schatzker’s classification (Burdin G. Arthroscopic management of tibial plateau fractures: Surgical technique. Orthopaedics & Traumatology: Surgery & Research (2013) 99S, S208—S218).
Associated soft tissue injury
These fractures are associated with a high incidence of soft tissue injury inside the joint, which demonstrates the usefulness of the arthroscopy in their treatment. Vangsness et al. reported a frequency of 47% concerning meniscal tears [14], Gill et al. reported rupture of the anterior cruciate ligament (ACL) in 32% of their cases [10], whereas Abdel-Hamid and Chang found soft tissue injury in 71% [15]. More analytically, Abdel-Hamid et al. in their diagnostic retrospective study (2006), hypothesized that the use of arthroscopy to evaluate soft tissue injury in cases of tibial plateau fractures would reveal a greater number of associated injuries than have previously been reported. The purpose of the study was to assess the incidence of soft tissue injury with the use of arthroscopy, and then to determine the relationship between frequency of soft tissue injury and tibial plateau fracture pattern severity.
98 consecutive patients with all types of closed tibial plateau fracture, who had undergone arthroscopically assisted reduction and osteosynthesis, were enrolled in this study. The average age at surgery was 49 years, and the mean follow-up period was 4.8 years.
71% of the patient had some associated soft tissue injury. The most common soft tissue injury was a meniscal tear, which was noted in 57%; all 6 types of tibial plateau fracture had a high incidence of meniscal tears, ranging from 33% to 75% and a peripheral tear was the most common type of meniscal injury. The second most common injury was an ACL injury; this occurred in 25% of the cases with the tibial avulsion representing 40% of ACL injury. Other ligament injuries were present in 3 to 5%. Type IV, V, and VI fractures exhibited significantly higher injury rates in the ACL and the PCL and multiple soft tissue injuries.
A variety of soft tissue injuries are common in tibial plateau fracture and must be suspected in all types of fractures; these can be diagnosed with the use of an arthroscope [15].
Anteroposterior, lateral (and oblique views less frequently) and a 15o caudal tibial view to assess the slope of the tibial plateau and the degree of articular depression, are included in the necessary radiographic evaluation [16,17]. CT is more precise in depicting articular displacement and comminution than plain films [18]. It has also been shown to help surgical planning and to lead to more reliability in classifying the fracture and deciding on a treatment plan [19,20] by illustrating the depressed fragments, the size of articular fragments and the location and orientation of fracture lines better than plain radiographs.
MRI, which has been found to be equivalent to traditional twodimensional CT [21], provides additional information about injuries to the soft tissue structures of the knee, which are not obtained with other imaging modalities. CT was found to be sensitive and specific in identifying ligament injuries because most of them had at least small bony avulsions, but MRI was necessary to detect meniscal injuries [22]. CT-angiography must be performed in cases where a vessel damage is suspected.
Treatment options
The treatment options for these fractures are the non-operative, with a plaster immobilization and the operative with either open reduction and internal fixation (ORIF) or minimal invasive arthroscopically assisted internal fixation (ARIF). Arthroscopy allows direct visualization of the soft tissue and articular surface damages [23-25] and, therefore, precise reduction of fracture fragments. Lately, arthroscopically assisted circular external fixation in bicondylar tibial plateau fractures has been introduced [26,27]. This technique is ideally used for Schatzker V and VI fractures to reduce the possibility of infection and soft tissue problems that occur by using two side plates [27].
Indirect reduction and external fixation has been advocated by many authors to improve the results and to minimize the risk of serious complications in high energy, complex tibial plateau fractures [28-30].
In any case, the goals of treatment are the restoration of normal alignment, joint congruity and stabilization and, ultimately, the prevention of degenerative osteoarthritis.
Successful results depend on the quality of reduction, ligament stability, treatment of associated soft-tissue injuries, and preservation of the soft-tissue envelope; in addition, good visualization of the articular surface with minimal dissection can help to achieve the desired goal [31-34].
In the last years the minimal invasive techniques have gained popularity, preventing mostly the additional surgical trauma by using a minimally invasive approach, and there is a plenty of studies with enough evidence to support the use of arthroscopy to assist in reduction of tibial plateau fractures [34-39].
In this field, the advocates of this technique claim that the arthroscopically assisted fixation of the tibial plateau fractures seems to have some advantages, such as:
• better visualization of the articular surfaces,
• better reduction of the fracture,
• better anatomical restoration of the joint surface,
• the possibility to assess and treat the associated intra-articular ligamentous and meniscal injuries,
• the possibility, through joint lavage, to remove loose fragments,
• the possibility to achieve stable fixation with the least amount of softtissues dissection,
• low risk of complications and low morbidity,
• the possibility of converting to arthrotomy, if necessary, and
• shorter hospital stay with faster recovery of joint motion.
In (Figure 2) we present one of our cases.
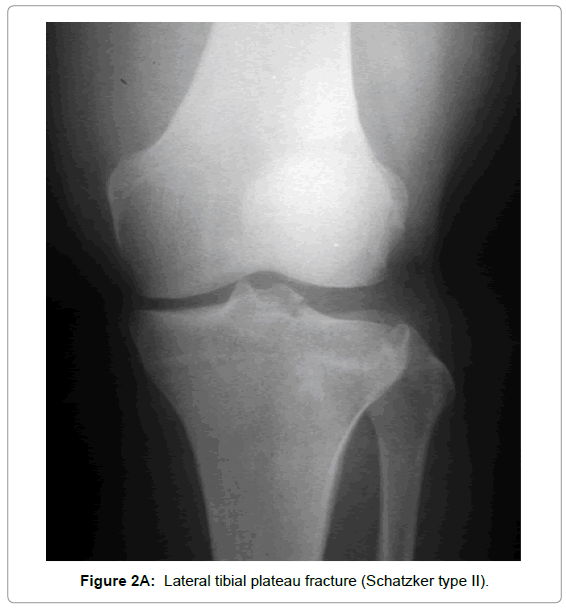
Figure 2A: Lateral tibial plateau fracture (Schatzker type II).
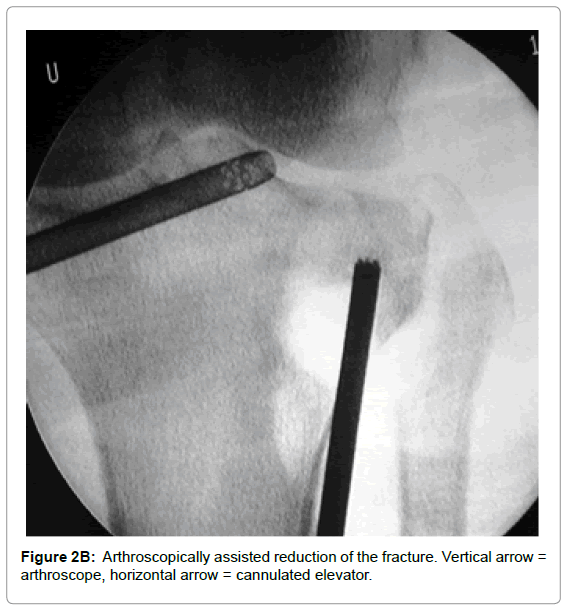
Figure 2B: Arthroscopically assisted reduction of the fracture. Vertical arrow = arthroscope, horizontal arrow = cannulated elevator.
Figure 2C: Arthroscopically assisted reduction of the fracture. Vertical arrow = arthroscope, horizontal arrow = cannulated elevator.
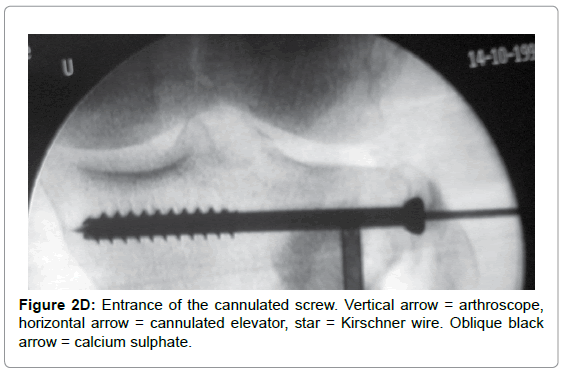
Figure 2D: Entrance of the cannulated screw. Vertical arrow = arthroscope, horizontal arrow = cannulated elevator, star = Kirschner wire. Oblique black arrow = calcium sulphate.
Figure 2E: Final X-ray.
This review was performed following the PRISMA guidelines (Liberati et al. 2009). We performed a literature search on June 23, 2014 using PubMed database with the words or phrases “arthroscopy AND tibial plateau fracture, arthroscopy-assisted reduction, arthroscopicallyassisted reduction.” The search was restricted to English language. Review articles were also scanned in order to find additional eligible studies. In addition, reference lists of all primary articles and previous systematic reviews and meta-analyses were scanned manually for additional publications. Information was carefully extracted from all eligible publications. Abstract evaluation was the first step and further full text scanning the second.
Inclusion criteria for this review were studies concerning tibial plateau fractures, treated operatively with arthroscopically assisted internal or external fixation, presenting at least 9 patients treated shows the mean results of all studies included in our paper.
Clinical studies were evaluated using the Levels of Evidence rating for studies addressing clinical care (Wright et al. 2003) and Grades of Recommendation are based on this evaluation (Wright et al. 2005) as follows:
• Grade-A recommendations: Consistent Level-I studies (Table 1a).
| Author | McGlynn, 1985 [3] | Jennings, 1985 [2] |
Bobic, 1993 [42] |
Fowble, 1993 [45] |
Holzach, 1994 [46] |
Bernfeld, 1996 [41] | Scheerlink, 1998 [34] |
Mazoue, 1999 [50] |
Roerdink, 2001 [38] |
Gill, 2001 [10] |
Kiefer, 2001 [48] |
| Number of patients | 20 | 21 (20 reviewed) |
16 | 12 | 16 (15 reviewed) |
9 | 38 | 14 | 30 | 25 | 29 |
| Average age | 14 to 85 | 40,3 | Unclear | 38,83 | 52,3 | 50,2 | 47 | 43 | 72 | 45,2 | 47,4 |
| Type of Fractures | I to VI (Hohl) | I to V (Hohl) | I,II,IV | II,III (Hohl) |
B2.2 B3.1 (AO) |
I to V (Hohl) | AO B & C | I to VI | I to IV | AO-type B1, B2, B3, C3 | |
| Average follow-up (months) | - | 12 to 60 | - | 6,63 | 35.3 (12 to 76) |
10,6 (6 to 18) |
60 (12 to 168) |
14,6 (5 to 30) |
36 (24 to 60) |
24 (12 to 35) |
25,1 (15 to 32) |
| Postoperative complications (%) | 15 | 10% | Unclear | 25 | 6,67 | 11,1 | 0 | 14,3 | 3,3 | 0 | 6,9 |
| Average IKS score | - | - | - | - | - | - | - | - | - | - | |
| Average Functional IKS score | - | - | - | - | - | - | - | - | - | - | |
| Average Lysholm score | - | - | - | - | - | - | - | - 5 excellent 6 good 0 fair 3 poor |
- | - | - 21 excellent 2 good 6 fair 2 poor |
| Average Clinical Rasmussen score | - | - | - | - | - | - | - | - | - 12 excellent 12 good 3 fair 3 poor |
27,5 84% excellent 16% good |
- |
| Average Radiological Rasmussen score | - | - | - | - | - | - | - | - | 4 excellent 10 good 10 fair 6 poor |
- | - |
| Arthrosis Xray (%) | - | 0% | - | 0 | 13,33 | - | 28,94 | 21,4 | - | - | 12,9 |
| Malalignment (%) | - | - | - | 0 | - | - | 15,78 | - | - | - | 6,9 |
| Study type | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy |
| Study Design | Case series | Case series | Case series | Case series | Case series PROSPECTIVE |
Case series | Case series | Case series | Case series | Case series | Case series |
| Class of Evidence | IV | IV | IV | IV | IV | IV | IV | IV | IV | IV | IV |
| Other evaluation score | - | Undefined Evaluation Method* : 80% Good 10% ROM 10-100o 5% Good with anterior instability 5% Soreness with activity *= patient returned to usual activity without limitation |
- | - | Davos Knee Scoring System 93,33% Excellent 6,67% Fair |
Undefined Evaluation Method : 66,67% excellent. 22,22% good, 11,11% moderate | HSS knee score: 78.9% excellent 13.2% good 7.9% fair 0% poor. |
- | - | - | - |
Table 1a: Short term results of tibial plateau fractures treated with arthroscopically assisted fixation Grade A.
• Grade-B recommendations: Consistent Level-II or III studies (Table 1b).
| Author | van Glabbeek, 2002 [39] | Asik, 2002 [40] |
Hung, 2003 [8] |
Chan YS, 2003 [5] |
Ohdera, 2003 [51] |
Suganuma and Akutsu, 2004 [55] | Pogliacomi, 2005 [52] |
Oguz et al, 2007 [27] |
| Number of patients | 20 | 45 | 31 | 18 | 19 | 26 | 18 | 13 |
| Average age | 49 | 39 | 46,9 | 35 | 47,5 | - | 36 | 27 |
| Type of Fractures | I,II,IV,V | I to VI | I to VI | V to VI | II to III | - | I to IV | V to VI |
| Average follow-up (months) | 39 (27 to 64) |
36 (14 to 72) |
36 (24 to 48) |
48 (39 to 69) |
22 (12 to 53,5) |
- | - (12 to 81) |
35 months (16 to 38) |
| Postoperative complications (%) | 0 | 4,2 | 6,45 | 33,3 (0% directly associated to arthroscopy) |
0 | 0 | 0 | 53,84 (0% directly associated to arthroscopy) |
| Average IKS score | - | - | - | - | - | - | - | - |
| Average Functional IKS score | - | - | - | - | - | - | - | - |
| Average Lysholm score | - | - | - | - | - | - | - | 82,46 |
| Average Clinical Rasmussen score | 28,89 90% excellent & good |
- 16 excellent (35%) 25 good (54%) 3 fair (7%) 2 poor (4%) |
- | - 4 (22,2%) excellent 12 (66,7%) good 2 (11,1%) fair |
- | - | - 8 (44,4%) excellent 7 (38,9%) good 2 (11,1%) fair 1 (5,6%) poor |
- |
| Average Radiological Rasmussen score | - | - | - | - 89% excellent & good |
- | - | - 5 excellent 7 good 4 fair 2 poor |
- |
| Arthrosis Xray (%) | - | 63 | 3,2 | 16,7 | 15,78 | - | 27,8% | - |
| Malalignment (%) | - | - | - | 11,1 | 0 | - | - | - |
| Study type | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy |
| Study Design | Case series | Case series | Case series | Case series | Cohort | Case series | Case series | Case series |
| Class of Evidence | IV | IV | IV | IV | III | IV | IV | IV |
| Other evaluation score | - | Resnick and Niwoyama criteria : grade 0: 17 (37%) grade 1: 18 (39%) grade 2: 7 (15%) grade 3: 4 (9%) |
HSS: 25 excellent (80,6%) 4 good (12,9%) 2 poor (6,45%) |
- | Hohl & Delamarter scoring system: 94.3±6.2 | - | Hohl’s clinical and radiographic scoring system: 7 excellent 8 good 2 fair 1 poor |
- |
Table 1b: Short term results of tibial plateau fractures treated with arthroscopically assisted fixation Grade B.
• Grade-C recommendations: Level-IV or V evidence, or conflicting evidence (Table 1c).
| Author | Rossi, | Chan, | Duan Xiao-jun, | Kayali, | Rousseau, | Levy, | Cristea, 2010 [44] | Siegler, | Dall’oca, 2012 [26] | Chiu CH, |
| 2008 [56] | 2008 [43] | 2008 [37] | 2008 [47] | 2008 [53] | 2008 [49] | 2011 [54] | 2013 [36] | |||
| Number of patients | 57 | 54 | 39 | 21 | 14 | 16 | 262 | 27 | 50 | 25 |
| (46 reviewed) | (21 reviewed) | |||||||||
| Average age | 48 | 48 | 35,9 | 41 | 47,3 | 44,8 | 51 | 45 | 47,19 | 46 |
| Type of Fractures | II to III | I to VI | I to V | I to III | I to IV | II | I to VI | I to III | I to VI | IV to VI |
| Average follow-up (months) | 60 | 87 | 33,6 | 38 | 75,6 | 41 | 60 | 59,5 | 73,27 | 86 |
| (22 to 128) | (12 to 60) | (50,4 to 96) | (24 to 138) | (12-116) | (60 to 108) | |||||
| Postoperative complications (%) | 4,3 | 0 | 0 | 0 | 0 | 0 | 4,9 | 0 | 14 | 36 |
| (0 associated to arthroscopy) | ||||||||||
| Average IKS score | 93.2 | - | - | - | 187,4 | - | 93 | 85,2 | - | - |
| (excellent or good in 43 patients (93%)) | ||||||||||
| Average Functional IKS score | 94.8 | - | - | - | - | - | 95 | 91 | - | - |
| (excellent or good in 43 patients (94%)) | ||||||||||
| Average Lysholm score | - | - | - | - | - | - | 92 | 96 | - | - |
| Average Clinical Rasmussen score | 28,2 | 28,4 | 26 | - | 28 | 29,25 | 9 | 25,5 | 27,62 | 25,9 |
| 81% excellent | 26 excellent 10 good | excellent 62% | excellent 79% | 11 (44%) excellent | ||||||
| 15% good | 3 fair | good 28% | good 21%) | 12 (48%) good | ||||||
| 2 (8%) fair | ||||||||||
| Average Radiological Rasmussen score | - | 16,1 | - | - | - | 16,87 | 9 | 8 | 16,56 | 15,8 |
| 96% excellent or good | excellent 52% good 33% | 12 excellent | ||||||||
| 4 good | ||||||||||
| Arthrosis Xray (%) | 8,6 | 19 | - | 24 | 50 | 12,5 | 25 | 47,6 | 2 | 24 |
| Malalignment (%) | 8,7 | 3,7 | - | - | - | 12,5 | 4,9 | 32,1 | 2 | 8 |
| Study type | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy | Therapy |
| Study Design | Case series | Case series | Case series | Case series | Case series | Case series | Case series | Case series | Cohort | Case series |
| PROSPECTIVE | ||||||||||
| Class of Evidence | IV | IV | IV | IV | IV | IV | IV | IV | II-III | IV |
| Other evaluation score | Mean HSS score: 93.4 (excellent or good in 46 patients (100%) | - | - | - | Resnick and Niwoyama (Radiological) : 0: 37%, 1: 39%, 2: 15%, 3: 9% | - | - | Tegner activity level: 4 | HSS: 76,36 | - |
| SF8: 4,64 |
Table 1c: Short term results of tibial plateau fractures treated with arthroscopically assisted fixation Grade C.
• Grade-I recommendations: Insufficient evidence to make a treatment recommendation.
The AO TraumalineTM database was also used to identify pertinent articles and find some articles’ Class of Evidence.
Our initial search identified 205 potentially relevant articles. Following thorough abstract and full text screening, only 25 met the inclusion criteria. 4 more articles were found through literature manual scanning. Finally, 29 studies met the inclusion criteria [2,3,5,8,10,26,27,34,36,37-55]. Information was carefully extracted from all 29 eligible publications.
983 patients were included in this analysis. Of the 29 included studies, two are retrospective cohort studies, two are prospective case studies, and all the others are retrospective case studies. Most of the studies (Figure 3) were focused on arthroscopically assisted internal fixation of tibial plateau fractures, while there was one about arthroscopically assisted external ring fixation of tibial plateau fractures [27] and another about both techniques depending on fracture type [44]. There were only three comparative studies [26,45,51] between these two techniques.
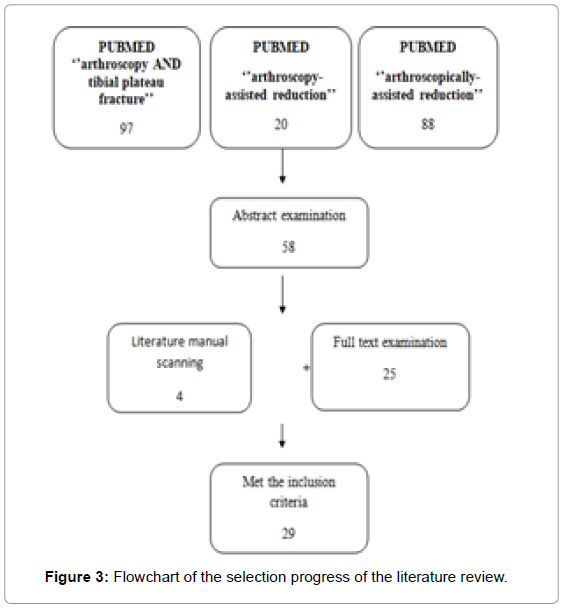
Figure 3: Flowchart of the selection progress of the literature review.
Most published studies, regarding the results of the arthroscopically assisted internal fixation of the tibial plateau fractures, enroll relatively small series of patients with different patterns of fractures. This is mostly due to the rarity of this condition and renders the comparison of the studies difficult. In 1985 McGlynn et al. published a series of 30 tibial plateau fractures, type I to VI according to Hohl’s criteria. They used arthroscopy in 20 of the patients for diagnosis, joint washing, partial meniscectomy, closed internal fixation and placement of grafts.
They concluded that, with diagnostic arthroscopy, they revealed information that they couldn’t get in other way and also that in 15 cases they achieved arthroscopically stable reduction with or without grafts. In terms of complications, they had 2 peroneal nerve injuries and one suture abscess in patients that they used arthroscopy. They conclude, that selected fractures can be reduced and stabilized with this technique and appropriate postoperative management determined [3].
In the same year, Jennings described 21 tibial plateau fractures (Hohl types I to V) treated with arthroscopically assisted fixation. Of those 21 patients, only 20 were available for a 1 to 5 years follow-up. 19 patients were treated with Arthroscopically Assisted Internal Fixation (ARIF) and one with arthroscopically assisted external fixation. 16 of the patients had good outcome. He concluded that arthroscopic technique offers advantages (minimal morbidity, less hospitalization) with few complications [2].
Bobic et al. in 1993, presented their 31 patients experience (from 1986 to 1993). Of those 31, only 16 (Schatzker types I,II,IV) were treated with the aid of an arthroscope. They found 7 meniscal tears (23%), 4 anterior (13%) and one posterior (3%) cruciate ligament tears. They had two complications –one deep vein thrombosis and one septic arthritis- but they fail to specify, if they were associated with the patients treated arthroscopically. They suggested that arthroscopy provides the best view to the tibial plateau, demonstrates clearly the extent of the fracture and the degree of displacement or depression of the articular surface and makes the diagnosis and reduction of soft tissue injuries more accurate. They, finally, raised the question of which fractures should be treated with this technique [42].
Holzach et al. in 1994 published their prospective study of 16 cases of lateral tibial plateau fractures in skiers. They used the arthroscope to visualize the knee joint, while using a cannulated plateau elevator to reduce the fracture and –subsequently- autogenous bone graft and, when indicated, transverse cancellous lag screw. The average follow-up was 35.3 months (12 to 76 months). Out of their 16 patients, 15 were available for a follow-up, of whom 14 presented excellent functional score according to the Davos Knee Scoring System. Only two reported resumption of activity to preinjury levels. There were no surgical complications other than a late bony exostosis in one patient. The authors summarize suggesting the ARIF technique is useful for the treatment of lateral tibial plateau fractures [46].
Bernfeld et al. in 1996 described satisfactory results and good functional outcome in a series of 9 non complicated tibial plateau fractures (Types I to V according to Hohl’s classification) with a mean follow up period of 10.6 months. The mean age of the patients was 50,22 . The intraoperative arthroscopy showed associated knee pathology in four patients (44.4%). They had no intraoperative complication. One patient presented peronial neurapraxia (fully recovered). They evaluated all their patients clinically and radiographically, but only 4 out of 9 arthroscopically during their follow-up. The remaining 5 patients refused an additional arthroscopic examination, as they were clinically satisfied. They found good and excellent clinical results in 88,88% of their patients and a sustained anatomic reduction in 75% of the patients they evaluated arthroscopically, during their follow-up. The authors found arthroscopic control technique advantageous in evacuating the knee, evaluating soft tissues pathology and treatment [41].
Scheerlinck et al. in 1998 reported excellent and good results according to the Hospital for Special Surgery (HSS) knee-rating Score in 92.1% of 38 patients treated with arthroscopically assisted internal fixation. The mean follow-up was 5.2 years (1.3 to 14) and 21 of the patients reviewed had a follow-up of five years or more. Narrowing of the joint space was found in 28.9% of the injured and 5.3% of the unaffected knees and axial deviation ranging from 5° to 10° in 15.8% of the injured and 10.5% of the unaffected knees [34].
Mazoue et al. in 1999 published their 14 patients’ series with an average follow-up of 14.6 months (range, 5-30 months). The average patient age was 43 years (range, 25-65 months). The average knee range of motion obtained was 5o-126o, with 9 of 14 patients regaining full symmetric motion. According to Lysholm scale, 79% of the patients received excellent and good rating. Only two patients experienced postoperative complications: one had painful hardware requiring removal, and the other had an infection that resolved after appropriate treatment. According to the authors, their report advances the treatment of tibial plateau fractures by documenting the feasibility of the arthroscopic management of many fracture types [50].
Roerdink et al. in 2001 reported excellent or good results in 80% of the patients treated with ARIF for different fracture types (Schatzker I: 6, Schatzker I: 13, Schatzker III: 5, Schatzker IV: 3, Schatzker V: 2, Schatzker VI: 1) with a mean age over 50 years. Secondary displacement occurred in 9 patients (30%) within 12 weeks after surgery, but no differences were found in the clinical outcome among the patients with or without secondary displacement of the fracture. Given the good clinical results, they suggested arthroscopically assisted osteosynthesis as highly efficient in the treatment of tibial plateau fractures in the elderly [38].
Gill et al. in 2001 published 25 cases (Schatzker I to IV), treated with ARIF. The post-operative mean Rasmussen score was 27.5. The authors concluded that the results of ARIF are comparable to those of ORIF, but with the advantage of the direct visualization of the articular surface, less soft tissue stripping, the evacuation of the hematoma, the remove of loose bodies (reducing in this way the morbidity), the length of hospital stay, and the capability to diagnose other intraarticular pathologies. All these factors could be causes of poor clinical and functional results [10].
Kiefer et al. also in 2001 reported the results of arthroscopic reduction and internal fixation of 31 lateral tibial plateau fractures. Fractures were stable and allowed full weight-bearing in all cases. Anatomic reduction was achieved in 25 patients. The authors concluded that fracture reduction using arthroscopic techniques is a suitable alternative for joint fracture repair, because additional soft tissue damage can be minimized [48].
Van Glabbeek et al. in 2002 in a series of 20 patients, presented excellent or good results in 90% of their cases. The only poor result noted was caused by the fact that they were unable to reduce the fracture arthroscopically and had to perform an arthrotomy [39].
In the same year, Asik et al. in their retrospective review, evaluated the results of arthroscopy-assisted surgery for tibial plateau fractures in 45 patients with closed tibial plateau fractures (mean follow-up 36 months). They reported satisfactory clinical (Rasmussen criteria) and radiological (Resnick and Niwoyama criteria) results and concluded that arthroscopy is an excellent and minimally invasive method for assessment and treatment of tibial plateau fractures. They added that the advantages are the complete and anatomical reduction of the fractured articular surface and the evaluation of other concomitant intra-articular pathology while this technique entails only little additional morbidity, especially compared to arthrotomy [40].
Hung et al. in 2003 described 31 cases of all types of tibial plateau fractures treated with arthroscopically assisted reduction from March 1996 to March 1998.The average age at operation was 46,9 years (21- 77 years) and the mean follow-up period was 3 years (2-4 years). They found associated intra-articular lesions in 30,7% of their patients. 25 had an excellent HSS Knee score, 4 good and 2 poor. 91% of the patients returned to their normal activities and 84% returned to their preinjury level activities, including sports. Only one patient with a Schatzker type VI fracture had post-traumatic arthritis in the final follow-up and another one with a type II fracture had joint depression. A patient with type V fracture had residual intra-articular loose bodies 3 months post-operatively. There were no complications directly associated with arthroscopy in any of the 31 patients. The authors suggest arthroscopically assisted treatment for tibial plateau fractures in order to achieve a much more satisfactory result, with quicker recovery and fewer complications [8].
In the same year Chan et al. in their case series of 18 patients with type V and VI (according to Schatzker’s classification) tibial plateau fractures, reported 100% union rate and 89% excellent and good clinical and radiological results (Rasmussen’s criteria). Complications occurred in 33,3% (n=6) of patients: wound dehiscence (n=1), condylar joint surface depression (n=3), paresthesia over the lateral calf (n=2). Secondary osteoarthritis developed in 16,7% (n=3) of the patients. They concluded that arthroscopic-assisted reduction with bilateral buttress plate fixation for complex tibial plateau fractures allows for accurate fracture reduction, diagnosis and treatment of associated intra-articular lesions, and less dissection than open reduction-internal fixation [5].
Suganuma and Akutsu in 2004 published a new technique of reduction of the articular surface impaction with the use of arthroscopy. Using custom made instruments, they impacted the cancellous bone through the metaphysis, reducing the articular discrepancy, under arthroscopically vision. They treated 26 patients consecutively with no complication and with no loss of reduction in any case. Unfortunately, these are the only data they present about their patients and results. However, they don’t miss the chance to state, that their technique completely eliminates the risk of the tip of the impactor protruding into the joint space and allows an accurate and quick reduction of the depressed fragments without using fluoroscopy [55].
Pogliacomi et al. in 2005, treated 18 patients sustaining Schatzker type I, II, III and IV fractures, performing a combined arthroscopic and radioscopic assisted reduction and internal fixation of their tibial plateau fractures. In this retrospective study they evaluated the functional and radiographic results and the value of the combined arthroscopic and radioscopic treatment of tibial plateau fractures. The mean age of the patients was 36 years and the follow up period ranged from 12 to 81 months.
They wrote down excellent and good results according to radiological, clinical and functional scales (Rasmussen’s clinical and radiographic scoring system). In only three patients they noted fair or poor results. Associated intra-articular injuries were found in 33,3% of the patients, which were treated after bone fixation. Finally, using Ahlback’s scoring system, they observed signs of osteoarthritis in 5 patients. They didn’t report any complications related to the arthroscopy procedure [52].
Oguz et al. (2007) presented their results of arthroscopically assisted circular external fixation in bicondylar tibial plateau fractures (Schatzker 5 and 6). Thirteen patients (12 males and 1 female) with a mean age of 27, were treated with circular external fixation under arthroscopic control. Eight of these patients had an open fracture. They used two portals and one arthroscope to wash up the joint, remove structures obstructing vision, reduce the joint surfaces, stabilize the fragments and treat soft tissue injuries. Fluoroscopy was used additionally for the insertion and application of the K-wires. After a 26, 6 months mean follow-up they found a mean Lysholm’s and Gillquist’s knee score 82,46. With regards to complications, they had 2 patients with superficial soft tissue infection and 5 patients with pin-tract infection.
They concluded that arthroscopically assisted circular external fixation of bicondylar tibial plateau fractures is efficient to obtain satisfactory functional results, allow early motion and full weight bearing and decrease the complications of simple ring external fixation [27].
Rossi et al. (2008) in a prospective study presented the results of their technique (arthroscopic-assisted technique conceived to use a compacted cancellous bone graft, taken from the medial metaphyseal side of the tibia, and a percutaneous fixation) after 5 y of follow up in 46 patients with type II and III tibial plateau fractures. Their mean age was 48 years.The clinical and functional scores (Knee Society Score, HSS score and Rasmussen’s) were excellent in 80 to 89% and good in 11 to 13%.The radiological score were excellent in 11% and good in 85% of the patient. Only in a few patients the results were fair and poor. They did not find any relationship between the outcomes and the type of fracture [56].
Chan et al. (2008) performed the arthroscopic assisted internal fixation of all types of tibial plateau fractures in 54 patients. The mean age was 48y and the average follow up period 87 months.
The results, according to functional and radiological scores, were excellent and good in the 96% of the patients. According to Ahlbäck’s scale, secondary osteoarthritis was noted in 19% of the cases. No statistical difference was noted between the unicondylar and bicondylar group of fractures.
No patient had serious complications such as infection, compartment syndrome, knee stiffness, or deep venous thrombosis, or other related to the arthroscopic technique [43].
Xiao-Jun et al. in the same year reported on the clinical outcome of their 39 patients’ series with Schatzker I to V tibial plateau fractures treated with ARIF. The mean follow-up was 33,6 months. According to the Rasmussen scoring system, 13 excellent scores were obtained in 26 patients, good in 10, and fair in 3 (2 type III and 1 type V). Generally speaking, 36 patients (92.3%) obtained satisfactory results and the mean score was 26±3. Thirty-five (90%) patients had no pain while walking, 3 (7%) reported mild pain, and one (3%) had moderate pain. All patients had excellent to good range of motion (ROM) results. Thirtyfour (87%) patients returned to normal work and thirty (77%) patients recovered to their previous activity level, including sports. No patient was dissatisfied with the treatment. All 39 fractures united. No severe osteoarthritis with complete loss of joint space or bone destruction was observed. They concluded that, ARIF in the treatment of selected tibial plateau fractures allows achievement of anatomic reduction and stable internal fixation with less morbidity than ORIF and it is superior in the visualization of the entire joint [37].
Kayali et al. (2008) in a retrospective study of 21 patients with low-energy Schatzker I to III tibial plateau fracture, who were treated with arthroscopically assisted percutaneous osteosynthesis (AAPO) presented 13 excellent (62%), 6 good (28%) and 2 fair (10%) clinical results, and 11 excellent (52%), 7 good (33%) and 3 fair (14%) radiologic results. They observed mild or moderate arthritic changes in 5 patients (24%). The mean follow-up was 38 months (range 12-96). They suggested that arthroscopically assisted treatment of lateral tibial plateau fractures yields satisfactory results and can be accepted as an alternative and effective method for the treatment of low-energy tibial plateau fractures [47].
Rousseau et al., also in 2008, published their long term results (mean follow-up 6,3 years) after ARIF for tibial plateau fractures. 14 patients with type I to IV, according to Schatzker’s classification, tibial fractures were evaluated. They presented excellent clinical results. Radiological signs of osteoarthritis were noted in 50.0% of cases, not relating to the clinical status. This is similarly to what has been reported after open surgery in the long term [53].
Levy et al. (2008) published their mid- to long-term results concerning the use of a medial approach for arthroscopic-assisted fixation for lateral tibial plateau fractures. Sixteen patients with Schatzker II tibial plateau fracture underwent ARIF through a medial metaphyseal window. After a mean follow-up of 41 months, they presented excellent clinical results in 100% of patients (Rasmussen criteria), with a mean score of 29,25. In 75% of patients there were excellent and in 25% good radiological results (mean Rasmussen score 16,87). There were no intraoperative complications. The most common complication was painful hard-ware; 5 patients required hardware removal. The use of small fragment screws has alleviated this complication. They concluded that the main advantage of using the medial approach for these fracture patterns is the creation of a long tunnel for sub-chondral support and the ease of fracture reduction, demonstrating satisfactory clinical and functional outcomes [49].
To our knowledge, Cristea et al. (2010) have the largest published series of tibial plateau fractures treated with the aid of arthroscopy. They presented the results from 262 patients with all Schatzker types of tibial plateau fractures, who were treated using the following method: in case of fractures with pure cleavage or split fractures, K wires were inserted perpendicular to the fracture’s line, subchondral, under X-ray and arthroscopic guidance. Eventually, compression forces were applied by inserting cannulated cancellous screws in parallel planes. In cases of fractures with depression, a K wire was inserted in the depressed bone fragment. This bone fragment was then lifted under X-ray and arthroscopic control and another K wire was inserted through these reduced bone fragments, subchondrally. Eventually, compression forces were applied by inserting cancellous screws in parallel planes.
In cases of complicated fractures, cleavage and depression, a K wire was inserted through the fracture’s cleavage directly in the depressed bone fragment, and this depressed bone fragment was lifted using strong forces till the K wire was bend, under X-ray and arthroscopic control. Then, another K wire was inserted through these reduced bone fragments, perpendicularly to the cleavage fracture, and compression forces were applied by inserting parallel cancellous screws. After the alignment of the articular surface was obtained, these fragments were fixed with cancellous screws or another K wire. In cases of comminuted fractures, first the depression was reduced and then the cleavage.
In cases of Schatzker type V-VI external fixation was used after obtaining the alignment of the articular surface.
After a mean follow-up of 60 months, they found very good results in 80% of cases. The mean International Knee Society (IKS) score was 93, whereas average functional IKS score was 95 and average Lysholm score was 92. The clinical Rasmussen average score was 9 and the radiological 9 as well. In terms of complications, they had one case with infection after a month which necessitated extraction of the screws and wires. In 15% of cases they obtained around 95-105 degree of knee flexion. Finally, in 4% of the cases they were not able to restore the entire surface of the tibial plateau.
The authors concluded that, besides the standard treatment with one or two plates and screws, reduction of the fracture’s fragment with K wires under X-ray and arthroscopic control (to confirm the quality of a good reduction and accurately assess and treat the associated lesions of the soft tissue) could be done, and then the fragments could be fixed with K wires and screws. They, finally, advocate this technique to treat all tibial fractures types and not only Schatzker I to III, mentioning its advantages, which are minimal blood loss, small infection rate, good mobilization of the knee without pain, cheaper implants, reproducibility of the technique, and that it can be performed in an emergency setting, cost – efficiently [44].
Siegler et al. in a recent publication in 2011 reported on results from percutaneous fixation of the tibial plateau fractures (type I-III) under arthroscopy, in 27 patients. In the 59.5 months follow up period they have collected many functional and clinical scores concluding in good and satisfactory results. 47.5% of the patients presented signs of osteoarthritis of which 10% was due to axis deviation. They concluded also in a positive statistical correlation between the age at the time of surgery and the midterm postoperative osteoarthritis signs [54].
The latest article to our knowledge is coming from Chiu et al. (2013) and presents the radiologic and clinical results of posteromedial fractures treated with arthroscopy-assisted reduction and buttress plate and cannulated screw fixation. They operated on twenty-five patients with posteromedial tibial plateau fractures (Schatzker IV,V and VI) with the described technique. The mean follow-up was 86 months (range, 60 to 108 months). The mean postoperative Rasmussen clinical score was 25.9 (range, 18 to 29). Among their patients, 11 (44%) had excellent results, 12 (48%) had good results (2 type IV, 1 type V, and 9 type VI), and 2 (8%) had fair results. The mean radiologic score was 15.8 (range, 10 to 18). The radiologic results were excellent or good in 96% of cases. All 25 fractures achieved successful union, and 92% had good or excellent clinical and radiologic results. The 3 fracture types did not significantly differ in Rasmussen scores or rates of satisfactory results. Secondary osteoarthritis was noted in 6 injured knees (24%). No complications directly associated with arthroscopy were noted in any of the 25 patients (100%) [36].
There are only three studies that compare the ARIF with the ORIF technique. Fowble et al. in 1993 compared retrospectively 12 cases treated with arthroscopic reduction and percutaneous fixation (ARPF) and 11 treated with open reduction and internal fixation (ORIF). The 23 patients suffered tibial plateau fractures with either local compression or split compression according to Hohl’s revised classification system. The results of the ARPF group were superior to those of the ORIF group according to the authors. In the ARPF group, all reductions were anatomic and remained fixed for at least 3 months postoperatively, whereas only six (55%) of the ORIF patients had anatomic reductions initially. Iliac crest bone graft was used in two patients in group A and 10 in group B, but the use of bone graft in the arthroscopically treated group had no effect on the final outcome. Moreover, the ARPF group had shorter postoperative hospitalization, faster full weight-bearing and presented fewer complications (Table 2). The authors concluded that arthroscopic reduction and limited percutaneous fixation should be considered as the treatment of choice in selected tibial plateau fractures [45].
| Fowble et al, 1993 | ARPF | ORIF |
|---|---|---|
| Number of patients | 12 | 11 |
| Average age | 38,83 | 37,82 |
| Average follow-up | 6,63 months | 6,25 |
| Type of fractures | II & III (Hohl) | II & III (Hohl) |
| Anatomic reduction | 100% | 55% |
| Bone graft used | 16,67% | 90,9% |
| Post-op hospitalization | 5,36 days | 10,27 days |
| Average time to full weight bearing | 8,95 weeks | 12,3 weeks |
| Complications | 25% | 36,36% |
| Flexion 120o | 83,3% | 63,63% |
Table 2: Fowble’s ARPF & ORIF results.
Ohdera et al. in 2003 evaluated, retrospectively, the value of arthroscopy for tibial plateau fractures by comparing the clinical results of arthroscopic treatment with the traditional open reduction method. In this study 28 patients with tibial plateau fracture were included, classified as type II and III according to Schatzker’s classification. Nineteen of these patients with a mean age of 47.5 years, were treated by arthroscopically assisted management (group S) and the remaining 9 with a mean age of 51.5 years, underwent conventional open reduction (group O). No patient had ACL injury.
The average follow-up time was 22 months in group S and 51.7 months in group O. They reported equally good results with no significant differences between the groups in terms of duration of operation, postoperative flexion, and clinical results. In group S, however, the postoperative rehabilitation was easier and faster, and more patients (84%) obtained an anatomical reduction, whereas in group O, only 55% did. They didn’t report on complications related to the arthroscopy procedure (Table 3). Also, with arthroscopic assisted management, accurate diagnosis and treatment of any associated joint pathology was possible as opposed to the closed method.Finally, they recommended the arthroscopically assisted management of selected tibial plateau fractures (type II and III) [51]. In 2012 Dall’oca et al. compared ARIF and ORIF in their level II-III Cohort study. They studied 100 patients with a mean follow-up period of 73,27 months (ranged from 12 to 116 months). They evaluated the Rasmussen score, the HSS (The Hospital for Special Surgery knee-rating) score and complications (Table 4). They suggested, that there are no differences between ARIF and ORIF treatment in Schatzker type I fractures, ARIF technique may increase the clinical outcome in Schatzker type II-III-IV fractures and that in Schatzker type V and VI fractures, ARIF and ORIF techniques have both poor medium- and long-term results but ARIF treatment, when indicated, is the best choice due to the lower rate of infections [26].
| Ohdera et al, 2003 | ARIF | ORIF |
|---|---|---|
| Number of patients | 19 | 9 |
| Average age | 47,5 | 51,5 |
| Average follow-up | 22 months | 51,7 months |
| Type of fractures | II & III | II & III |
| Postoperative complications | 0 | 0 |
| Anatomic reduction | 84% | 55% |
| Bone graft used | 84,2 | 100% |
| Osteoarthritic changes | 15,78% | 77,77% |
| Average time to full weight bearing | 9,2 weeks | 10,3 weeks |
| Operation time | 126,3 min | 131,7 |
| Flexion (deg) | 151,3 | 148,9 |
| Time to 120o flexion (weeks) | 4,6 | 9,1 |
| Hohl * Delamarter score | 94,3 | 89,7 |
| Subjective score | 25,6 | 24,0 |
| Functional score | 44,2 | 43,4 |
| Anatomical score | 24,5 | 22,2 |
Table 3: Ohdera’s ARIF & ORIF results.
| Dall’oca et al, 2012 | ARIF | ORIF |
|---|---|---|
| Number of patients | 50 | 50 |
| Average age | 47,19 | 51,16 |
| Type of Fractures | I to VI | I to VI |
| Postoperative complications | 0 associated to arthroscopy 14% totally |
- 58% |
| Average HSS score | 76,36 | 73,12 |
| Average Clinical Rasmussen score | 27,62 | 26,81 |
| Average Radiological Rasmussen score | 16,56 | 15,88 |
Table 4: Dall’oca’s ARIF and ORIF for tibial plateau fractures mean results.
There are a number of limitations in this review. First of all, the language we could only study English literature. Secondary only case series and three comparative studies (except for two cohort studies by Dall’oca and Ohdera) were available for analysis. These have a low evidence level. Conclusions about the effectiveness of a specific therapeutic intervention are best provided by well-conducted, randomised controlled trials or meta-analyses, but none of these exist. Moreover – as previously stated – the heterogeneity of the way the results presented in the studies are analyzed, make statistical analysis difficult. Therefore, only a review of non-randomised trials could be performed.
Despite the small amount of studies comparing ARIF with ORIF technique [26,45,51] and studies with an average follow up longer than 3 years) [5,8,26,34,36,38-40,43,44,47,49,52-54,56], the advocates of ARIF suggest, that this technique can have a key role in the management of tibial plateau fractures and is the treatment of choice for associated intra-articular pathology.
Nevertheless, most of these studies, if not all, are selected, small studies, poorly controlled and with potential bias. This creates the need for well-designed studies to evaluate long- and short-term function and risk of posttraumatic osteoarthritis in arthroscopically-assisted treated patients. It is a demanding and with a long learning curve technique, but in the hands of an experienced surgeon it has very good results even in complex fractures.
On the other hand, as Harris and his associates [57] suggest, a poorly executed ARIF should never substitute for a well-done ORIF.
All authors equally contributed to this paper with conception and design of the study, literature review and analysis, drafting and critical revision and editing, and final approval of the final version.