Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Review Article - (2014) Volume 2, Issue 2
Vertebral fractures are the most common fractures in patients with osteoporosis; however, the biggest part of them never comes to clinical attention. Symptoms and secondary deformities can reduce the heath-related quality of life, and increase the risk of mortality. Vertebral fractures can be treated conservatively or surgically by vertebroplasty or kyphoplasty. In this study, we report an overview on the osteoporotic vertebral fractures management, focusing on the most used approaches. Although effectiveness of all these approaches is defined, surgical procedures can lead to higher short-term benefits about relief of pain, improved vertebral body height, physical function and quality of life; the rate cost-effective for vertebroplasty and kyphoplasty appears definitely higher.
<Keywords: Vertebral fractures; Osteoporosis; Conservative treatment; Surgical treatment
Vertebral fractures are the most common fractures in patients with osteoporosis [1-3] (Figure 1). The World Health Organization considers osteoporosis a critical health problem among general population; it is second only to cardiovascular diseases [4]. The prevalence of osteoporosis in Italy is among 23% in women (45% from 70 to 79 years old or more), and almost 15% in men; thus, it is supposed that about 4 million Italian women and 800.000 men are affected by osteoporosis [5,6].
The European Vertebral Osteoporosis Study reported that about 12% of people from 50 to 80 years old present vertebral deformities on imaging, with about 1.4 million of new vertebral fractures dues to osteoporosis each year; a recent study presents an estimated number of vertebral fractures in Italian people aged from 40 to 100 years old: during the year 2004 they were 58.987, 59.116 in 2005, and 60.880 in 2006, with a +3.1% each year [7-9]. However, it is difficult to assess the real incidence of vertebral fractures among the general population: seen that vertebral fractures can be asymptomatic (50% of cases) or produce non-specific symptoms, such as back pain, the biggest part (about 70%) of vertebral fractures never comes to clinical attention [10]. The hospitalization rates of patients with vertebral fractures in Italy between 2004 and 2006 were 27.6% [11]. Symptoms such as constant back pain and physical limitations following a vertebral fracture are referred by about 40% of patients [12]. The failure of the anterior column of the vertebral body causes the wedge deformity and the resulting spine deformity in kyphosis, that can reduce the pulmonary function [5,13]. Symptoms and deformities can interfere with normal day activities and decrease the health-related quality of life [12,14-16].
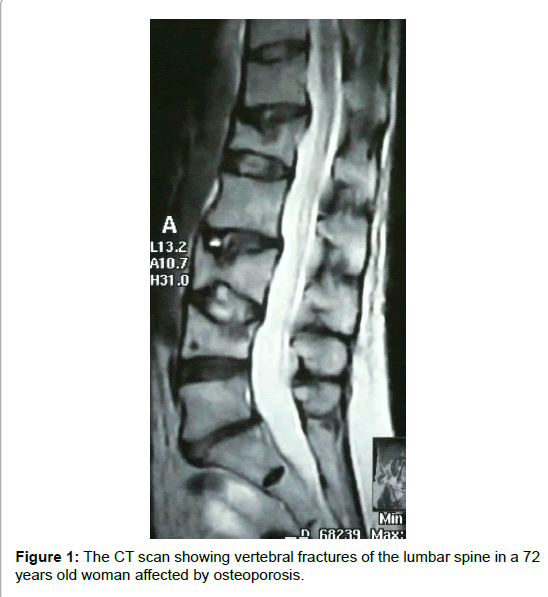
Figure 1:The CT scan showing vertebral fractures of the lumbar spine in a 72 years old woman affected by osteoporosis.
Vertebral fractures should be treated when painful and to avoid complications and deformities [17]. Patients with a previous vertebral fracture present a higher risk of subsequent osteoporotic fractures, especially during the first year, and an increased risk of mortality until 23%, with an expectation of life in 5 years reduced of 16% [5,18-21].With a world that took to an aging population, the incidence of osteoporosis and consequently of vertebral fractures is predicted to increase [12].
The aim of this study was to review the treatment of osteoporotic vertebral fractures, about conservative management, vertebroplasty and kyphoplasty.
Vertebral fractures treatment
A comprehensive search of PubMed, Medline and Google Scholar was performed; various combinations of the keywords as vertebral fractures, osteoporosis, conservative management, kyphoplasty, vertebroplasty, cementoplasty were used. A total of over 1500 citations were obtained and more papers were obtained from the references of the studies which were studied. We included articles with relief, extracted from important journals, recent (expect about bracing because more relevant articles are a little timeworn), with large series, and presenting comparisons between two techniques. Exclusion criteria were case reports, non relevant articles, non relevant journals, little series. A total of 47 studies were finally reviewed.
Conservative treatment
Conservative treatment for vertebral fractures consists in bed rest, analgesics, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), braces and rehabilitation; but the duration of each of them is not clear in literature [1,3,17].
Bed rest: Bed rest should be advised only in the acute phase during some days, for not reducing muscles activity and increase osteoporosis [22].
Drugs: NSAIDs are indicated to treat pain, but complications are widely reported in literature: abdominal pain, diarrhea, increase of 47% of cardiovascular risk, and above all gastrointestinal injuries, that lead to 16.000 deaths in USA [Drugs: NSAIDs are indicated to treat pain, but complications are widely reported in literature: abdominal pain, diarrhea, increase of 47% of cardiovascular risk, and above all gastrointestinal injuries, that lead to 16.000 deaths in USA [17,23-25]. Gastrointestinal risk is reduced by the use of selective Cyclooxygenase-2 Drugs (COX-2), but cardiovascular risk is increased [26-28].,23-25]. Gastrointestinal risk is reduced by the use of selective Cyclooxygenase-2 Drugs (COX-2), but cardiovascular risk is increased [26-28].
Muscle relaxants can be useful in treating muscles spasms during the acute phase and, in associations with NSAIDs, in stopping the cycle of pain, but complications such as drowsiness are reported [29,30].
Strong pain can be controlled by analgesics: paracetamol is preferred to opioids because of the risk of the reduction of gastrointestinal motility, urinary retention and cognitive deficiency that can lead to serious problems in aged patients [31].
Drugs for treating osteoporosis appear to have some effects in relief of pain too, and always have to be indicated in case of osteoporotic fractures [3].
Braces: Braces have to be indicated for vertebral fractures, but no consensus about type and length of brace wearing is reported in the literature, however, it should be up to 6 months [17,32].
The goal for using a brace is: to reduce pain, bed rest inactivity, and secondary deformities; thus, they have to be comfortable, easy to put on, light, made with pressures, pads, chairback, in hyperextension position; braces don’t have to be too rigid (it should lead to stiffness, limitation of movement and normal respiration) [17,32-34]. Several brace models have been designed, but some limitations are reported: Jewett and cruciform anterior spinal hyperextension braces don’t permit the complete control on spine movement on coronal and transverse planes, and the Knight-Taylor brace on axial plane and dynamic balance [17]. A moulded in hyperextension plastic thoracolumbar orthosis appeared to be the best design [33,35].
Rehabilitation: Rehabilitation has many reported benefits; it has to be composed by proprioceptive and extensor muscles strengthening programs, and has the scope to reduce osteoporosis, the risk of successive vertebral fractures and of secondary deformities in hyperkyphosis, to improve physical function and the subsequence quality of life [36- 39]. Effectiveness of rehabilitation is reported between 10 weeks and 6 months [39].
Pain relief after conservative treatment is reported between 4 weeks and 8 months [1,16]. No differences in pain relief (by using the Visual Analogic Scale [VAS]) between conservative and surgical treatment were seen at 3 month by Rousing et al. [40], 6 months by Shen et al. [41], Diamond et al. [42] and Alvarez et al. [43], and 12 months by Nakano et al. [44] and by Wardlaw et al. [7]. However, some residual pain can be present in patient after conservative management of vertebral fracture [1,16].
Improvement in physical function (by using the Short-Form- Health Survey 36 [SF-36] score) is reported by Wardlaw in 95% of vertebral fractures conservatively treated, and at 1 year it was similar to that obtained surgically [7]. No differences in function improvement (by using the Roland Morris Disability Questionnaire [RMDQ]) and return to work activities between conservative and surgical treatment were seen at an average last follow-up of 4 years [41].
However, by conservative treatment, the restoration of vertebral body height cannot be achieved and the risk of secondary deformity in kyphosis cannot be reduced [3,45].
Surgical treatment
Surgery for treating osteoporotic vertebral fractures usually consists in percutaneous minimally invasive procedures: vertebroplasty and kyphoplasty.
The purposes of surgical treatment are the rapid relief of pain, the restore of the vertebral body height and the prevention of the kyphosis deformity [1,3].
Surgical procedures are associated with higher risks of complications and costs than conservative management [46], but today, with better control of patients comorbidities and reduced complication rates, surgery produces high satisfactions with acceptably risks [1,3], and it can be an alternative treatment for people that can’t manage braces [17].
Earlier relief in VAS after surgical treatment is reported in 1 month [41]. Moreover, kyphosis are quite well controlled by surgical procedure: from an average value of 12.8° to 11°, but it seems that there is no relation between kyphosis magnitude and pain [46].
Vertebroplasty
Vertebroplasty is a percutaneous minimally invasive procedure, that was first performed in France in 1985 for treating vertebral angiomas [47]. To perform a vertebroplasty, a bone needle is passed through or lateral unilateral or bilateral pedicles until the vertebral body and a small amount of cement of Polymethylmethacrylate (PMMA) or Calcium phosphate-based, mixed with antibiotic and barium or tantalum is pushed into. Once injected, the cement hardens quickly. The procedure is monitored by fluoroscopy [1,3,44] (Figure 2).
Pain relief after vertebroplasty is reported in 24-48 hours [1], and it remains higher compared to conservative management until from 6 weeks [3,47-50] to 13 months [51,52]. Several studies reported the relief of pain after vertebroplasty in 70-90% of cases [1,18]. Even if vertebroplasty is performed 3 months later the fracture when conservative treatment failed, pain relief (measured by VAS) and functional outcome (measured by the Oswestry Disability Index, [ODI]) improve significantly up to 2 years [53].
The restoration of vertebral body height can be achieved by vertebroplasty [51], especially in fresh fractures [3,54].
One of the most common complications of vertebroplasty is the leakage of the cement, until 65% of cases [1,3,52,55], with symptoms in only 1.1-3% of them [47,56]. Cement can leak to the peridural space or to vertebral venous system, and it can produce radiculopathies (4% of cases), spinal cord injuries (<0.5% of cases) [47,55,57,58], pulmonary or cerebral embolism [1,59]. Other general complications are reported from 2.4 to 4.8% of cases [56,60].
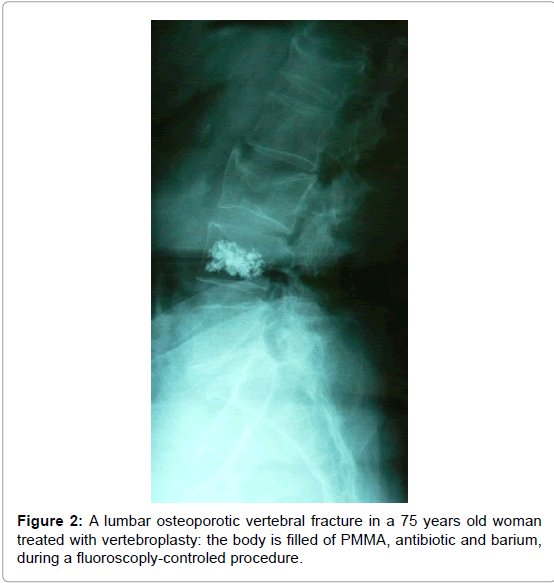
Figure 2:A lumbar osteoporotic vertebral fracture in a 75 years old woman treated with vertebroplasty: the body is filled of PMMA, antibiotic and barium, during a fluoroscoply-controled procedure.
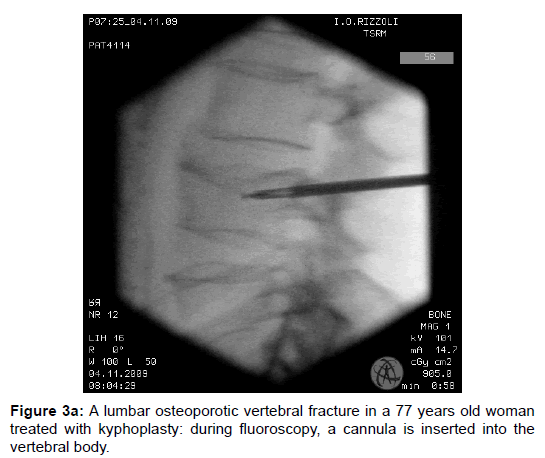
Figure 3a:A lumbar osteoporotic vertebral fracture in a 77 years old woman treated with kyphoplasty: during fluoroscopy, a cannula is inserted into the vertebral body.
Baroud et al. reported an inward bulge up to 17% of the endplate adjacent to the one augmented after vertebroplasty that may be cause fractures [61]; adjacent vertebral fractures were seen by Lovi in 1.3% of cases [53], by Schofer in 3.3% [52] and by Grohs in 4.3% [62]; others papers reported non-significant differences with conservative treatment [40,42]. New vertebral fractures were reported in 1.3% of patients by Lovi [53].
Even if vertebroplasty is associated with higher costs than conservative management, the Ratio cost-effective is higher [46,54].
Kyphoplasty
Kyphoplasty is a percutaneous minimally invasive procedure. Patient is positioned in the hyperlordotic position; a little cannula is inserted until the vertebral body, and a balloon catheter is passed through it; afterwards, it is blown to increase the collapsed space and to create a defined cavity, that is then filled of the cement [1,63-65] (Figure 3a- c).
Several studies reported the relief of pain until 90% of cases [1,2,18,52], that is gained in 24-48 hours [1], and sustained up to 2 years follow-up [51,62], with a subsequence reduction of drugs necessity during the first 6 months [7].
Improvement in physical function (by SF-36 score) is reported by Lieberman et al. [2], by Kasperk et al. [66], and by Wardlaw et al. in 95% of cases (improvement of 28.3% at 1 month, versus 6.4% in the conservative treated control group) [7].
Pain relief (as measured by the VAS) and functional outcome (as measured by the ODI) improve significantly up to 2 years, even if kyphoplasty is performed 1 months later the trauma, when conservative treatment failed [53].
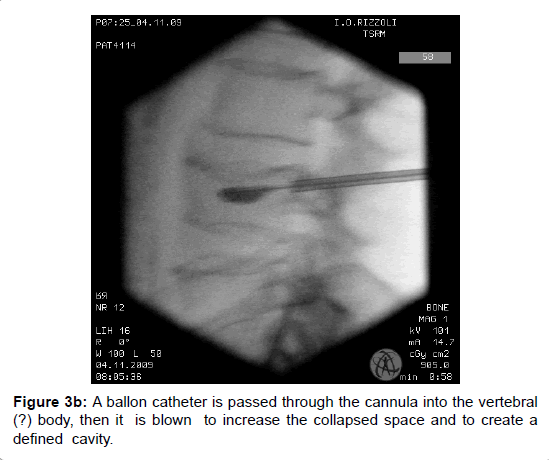
Figure 3b:A ballon catheter is passed through the cannula into the vertebral (?) body, then it is blown to increase the collapsed space and to create a defined cavity.
Figure 3c:The cavity is filled with PMMA, antibiotic and barium.
Restoration of the vertebral body height is achieved in 47% of cases [2,51], higher than in vertebroplasty procedures [51]; at postoperative time, restoration is up to 15.4%, remaining stable up to 3 years followup [53,66]. The control of the vertebral body height reduces the risk of secondary spine deformity in kyphosis [51,66].
New vertebral fractures were seen in 33% of cases at 1 year in a few studies [6], adjacent vertebral fractures were seen by Liu et al. in 4% of patients [51] and by Grohs et al. in 21.4% [62], but other studies reported no new or adjacent fractures [53,67].
Patients operated by kyphoplasty can return to daily activities faster than conservative treated patients, with a difference of 60 days as reported by Wardlaw et al. [7]. Wardlaw et al. also reported an improvement of quality of life as measured by SF-36 physical component summary scale, Euro QOL-5D quality-of-life questionnaire and RMDQ at 1 month until 3 years [7].
Complications after kyphoplasty were seen in 0.8% of 360 consecutive procedures by Majd et al. [68]. Cement leakage is less frequent after kyphoplasty procedure, because of the major cement viscosity [1,18]; the rate is reported form 6.6% to 27%, and all cases were asymptomatic [2,7,45,52].
No differences between kyphoplasty and vertebroplasty were seen in the assessment of pain (VAS) and function (ODI) at 2 years followup by Grohs et al. [62]. Schofer et al. reported a better reduction of kyphosis after kyphoplasty then vertebroplasty [52]. Lovi et al. reported a longer surgical time and bigger quantity of used PMMA after kyphoplasty then vertebroplasty [51,53].
Kyphoplasty is associated with higher costs than conservative management, but the Ratio cost-effective is higher [67].
No differences in pain relief after conservative or surgical treatment was seen over time; this means that the same result can be reached by the two procedures. Considering that the surgical treatment has higher risks, although limited, and higher costs, conservative management should be preferably indicated. However, agreement is reported in literature about short-term benefits of surgical treatment in terms of relief of pain, improved vertebral body height, physical function and quality of life; the rate cost-effective for vertebroplasty and kyphoplasty is definitely higher. Vertebroplasty presents more risks of complications then kyphoplasty; kyphoplasty is the best procedure to regain the height vertebral body and to control kyphosis, but longer surgical time is seen; thus, kyphoplasty should be better indicated in younger people with higher functional demands. The risk of subsequent vertebral fractures have not been clearly demonstrated by literature after the three procedures; referral physicians should be aware patients about this risk, and a focused osteoporosis therapy should be indicated.
Several limitations in comparing studies about choosing conservative or surgical treatment in osteoporotic vertebral fractures have been found, especially because of the big difference in number of patients and clinical scores, and the little sham-controlled studies.