Journal of Developing Drugs
Open Access
ISSN: 2329-6631
ISSN: 2329-6631
Case Report - (2017) Volume 6, Issue 3
Calcium channel blocker (CCB) overdose is a potentially fatal poisoning. The use of intravenous lipid emulsion (ILE) therapy for CCB poisoning has emerged in the past few years. In 2017, the American College of Medical Toxicology published interim guidance for the use of ILE resuscitation in these cases. We report an uncommon complication of ILE, acute respiratory distress syndrome, treated with veno-venous extracorporeal membrane oxygenation (ECMO). Case report: A 40-year-old hypertensive woman presented with shock (blood pressure 62/34 mmHg, pulse 86/ min) following ingestion of 4,800 mg verapamil slow release and 1,500 mcg clonidine during a suicide attempt. She was treated with calcium gluconate, sodium bicarbonate, IV high dose insulin, IV glucagon, cardiac amines and vasopressors without response (blood pressure 69/37 mmHg, pulse 78/min). ILE was initiated, and two hours later, she developed acute respiratory failure necessitating intubation and mechanical ventilation. Due to poor oxygenation (pO2 44 mmHg; FiO2 100%) emergent veno-venous ECMO was instituted. After one hour her blood pressure increased to 104/50 mmHg (pulse 80, pO2 75 mmHg), and continued so until weaning from ECMO and ventilation. Conclusion: Acute respiratory distress syndrome can be a major life threating complication following ILE; venovenous ECMO is suggested for its treatment.
<Keywords: Acute respiratory distress syndrome; Intravenous lipid emulsion; Extracorporeal membrane oxygenation; Verapamil; Poisoning
High-dose insulin (HDI) and intravenous lipid emulsion (ILE) have emerged as a treatment for severe toxicity from some calcium-channel blockers (CCBs) and beta blockers toxicity which caused refractory shock [1]. Intentional ingestion of CCBs is one of the most potentially lethal drug overdoses. Their toxicity is characterized by mainly hypotension, bradyarrhythmia, A-V blocks, cardiac arrest and bowel ischemia; manifestations in slow-release formulations can be delayed [2].
Three mechanisms were proposed for ILE action: (a) Modulation of intracellular metabolism of the cardiovascular system by providing essential fatty acids serving as an energy source [3]. (b) Lipid sink or sponge mechanism causing redistribution of lipid soluble drugs out of the site of toxicity [4]. (c) A post-conditioning effect providing protection against ischemic damage [5,6].
The main reported complications of ILE include pancreatitis and acute respiratory distress syndrome (ARDS) [7]. Cause and effect relationship in these cases have not always been clear. In addition, ILEinduced lipemia can interfere with laboratory determination of AST, ALT and triglycerides [7].
Few case reports described the successful use of extracorporeal membrane oxygenation (ECMO) for CCBs poisoning [8-10]. Only one case report of ECMO used for ILE-induced ARDS was published [11], the procedure was veno-arterial ECMO, not veno-venous.
The objective of this report is to describe ARDS temporally related to ILE used for severe verapamil poisoning, and the successful use of veno-venous ECMO.
A 40-year-old, 80 kg hypertensive woman treated with clonidine was brought to our emergency department after attempting suicide by ingesting 4,800 mg slow release verapamil and 1,500 mcg clonidine. The empty pill packages were brought with her to the hospital.
On admission, the patient was fully conscious and cooperative, Glasgow coma score 15; pulse 68 beats/minute, blood pressure 62/34 mmHg, saturation 100% in room air. Laboratory tests revealed serum creatinine 2.73 mg/dL, BUN 21 mg/dL, potassium 5 mmol/L, sodium 140 mmol/L, glucose 266 mg/dL, pO2 57 mmHg, pCO2 24 mmHg, and pH 7.31.
The patient was treated with IV normal saline 1,000 mL and dopamine 10 mcg/kg/min, and then transferred to the cardiac intensive care unit. Her blood pressure increased to 90/55 mmHg, pulse was 60 beats/minute, saturation 99% in room air; chest X-ray was normal (Figure 1).
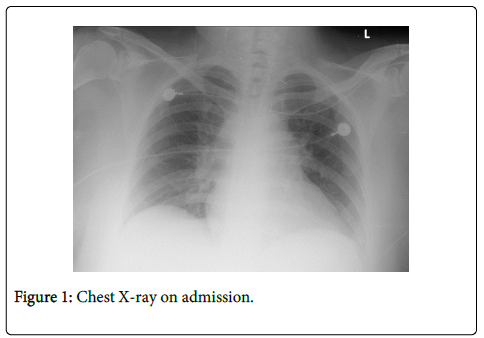
Figure 1: Chest X-ray on admission.
After a few hours blood pressure decreased to 75/50 mmHg (pulse 63 beats/min), and she was treated with IV calcium gluconate 1 gr, IV insulin short acting 50 units, noradrenaline 0.2 mcg/kg/min and dopamine 10 mcg/kg/min. As her blood pressure decreased to 69/37 mmHg, Neo-synephrine 0.15 mcg/kg/min was added.
Due to unresponsiveness to this vasopressor treatment, ILE was administered; 20% lipid emulsion (Lipofundin), 1.5 mL/kg bolus followed by 40 minutes maintenance dose of 0.25 mL/kg/min [2]. Total dosage of ILE was 11.5 mL/kg. Two hours after ILE was initiated, she developed ARDS manifested by tachypnea, breathing difficulty and sweating. Laboratory tests were pH 7.1, pO2 60 mmHg and pCO2 52 mmHg. Chest X-ray showed bilateral pulmonary congestion, unresponsive to furosemide 60 mg IV. The patient had to be intubated and mechanically ventilated, and a temporary pacemaker was introduced due to the new development of a complete A-V block.
In spite of optimization of mechanical ventilation parameters (PEEP 7 cm H2O, pressure support 14 cm H2O, FiO2 100%) the patient continued deteriorating; blood pressure 70/50 mmHg, pH 7.07, pO2 44 mmHg, pCO2 64 mmHg, HCO3- 18.5 mEq/L, lactate 2.7 mmol/L. Repeated chest X-rays showed bilateral patchy opacities compatible with ARDS (Figure 2).
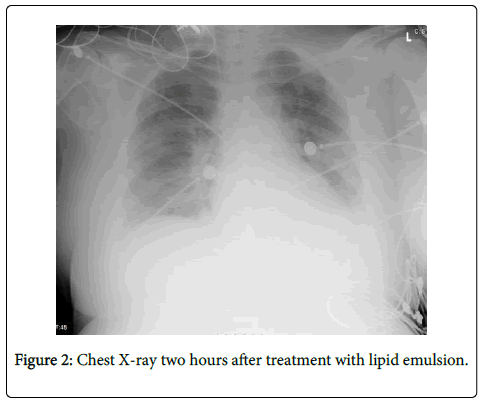
Figure 2: Chest X-ray two hours after treatment with lipid emulsion.
Transesophageal echocardiogram showed normal biventricular function. Due to acute renal failure with anuria (serum creatinine 5.23 mg/dL), hemodialysis was initiated.
After hemodialysis, IV methylene blue 1 mg/kg, nitric oxide and IV glucagon 100 mcg/kg/min were added because of the low blood pressure and poor oxygenation, without any response. At this stage veno-venous ECMO support was initiated. Under this treatment, blood pressure increased in the following day and renal function gradually improved; urine output 40 mL/hr, serum creatinine 2.03 mg/dL and BUN 47 mg/dL. When blood pressure was stable at 140/80 mmHg (pulse 92 beats/min) the amines were discontinued.
On the sixth day of veno-venous ECMO treatment the patient was weaned from this support, and two days later (8th day of hospitalization) she was extubated and returned to spontaneous breathing.
On the 28th hospitalization day the patient was discharged to the community in good medical state (blood pressure 116/74 mmHg, pulse 56 beats/min, saturation 97%) for ambulatory rehabilitation and psychiatric follow up.
In our patient, refractory shock developed after an intentional overdose with mainly slow release verapamil, and to a lesser extent clonidine. Due to the lack of response of the shock to the treatment, ILE was administered. All though ARDS can develop secondary to shock or secondary to verapamil over dose, the proximity to administration of the ILE most probably developed ARDS shortly afterwards, unresponsive to diuretics and mechanical ventilation. Veno-venous ECMO was initiated, and resulted in respiratory and subsequently cardiac and renal recovery.
ARDS was temporally related to ILE therapy suggesting an association between them. ARDS was reported in few cases as a complication of ILE [7,11,12]. Suggested mechanisms include hypoperfusion, hypoxic injury from pulmonary vasoconstriction, and effects from resultant localized alveolar edema [13]. Animal model showed that a bolus injection of soybean-based fat emulsion containing oleic acid (as in ILE), produced acute lung injury with hypoxemia and increased pulmonary vascular permeability [14]. In patients with ARDS, 500 mL of 20% ILE administered over 8 hours resulted in increased pulmonary artery pressure, pulmonary shunting, pulmonary vascular resistance, and decreased partial pressure of oxygen in the alveoli/fraction of inspired oxygen (paO2/FiO2) [15].
ECMO was provided to our patient for treating the unresponsive acute respiratory failure. When the cardiac function is preserved, venovenous ECMO is a preferable procedure to improve gas exchange and spares the complications of veno-arterial ECMO. Veno-arterial ECMO is complicated by bleeding, thrombosis hemolysis and thrombocytopenia. These, along with an increased risk of disseminated intravascular coagulation and heparin-induced thrombocytopenia, increase the risk for neurological events. Veno-venous ECMO requires less heparin than veno-arterial ECMO, thus reducing mortality from bleeding. ECMO was reported in several cases of CCBs poisoning [8-10], in all of them veno- arterial ECMO was used because of cardiovascular collapse. This is unlike our case where veno-venous ECMO was used due to ARDS.
Our case suggests that veno-venous ECMO should be considered in ILE-induced ARDS without evidence of cardiogenic shock.
The authors declare no conflict of interest.