Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2013) Volume 3, Issue 1
Introduction: Adverse Drug Reactions (ADRs) reporting is the cornerstone for any Pharmacovigilance system. The attitude and awareness towards ADRs reporting shows great variation among the health pharmacists and many factors influences the reporting of ADR. Aims and objective: To determine and evaluate awareness, knowledge and attitude of community pharmacists towards ADRs reported in the Makkah in Kingdom of Saudi Arabia (KSA). Materials and method: The present cross-sectional study was conducted by taking face to face interviews of 170 community pharmacists in Makkah. A prescribed questioner was used to collect basic information, professional information and knowledge about ADR reporting system and constrains in reporting ADR. Results: It was observed that all the participants were male and were of 23-30 yrs of age group. 88% of pharmacists were not having internet facility at their work place. Only 18% participants were aware of the ADR system. 56% of the respondents were not aware of the existence of the Saudi National Pharmacovigilance centre (NPC). According to 65% respondents the Ministry of Health (MOH) was responsible receiving and interpreting ADR reporting, whereas 65% of respondents considered the reporting of ADRs to be integral to this professional role as a pharmacist. The main factors that discouraged ADR reporting were the lack of reporting forms being available, that it was time consuming, that they did not know how to report them and some commented on their indifference to the system. Conclusion: The Community pharmacists could play an important role in ensuring the use of safe medications in patients. To achieve this aim more knowledge about the importance of reporting ADRs through appropriate training courses should be encouraged.
Keywords: Pharmacovigilance, Adverse Drug Reactions (ADRs) reporting, Community pharmacist, Makkah, Kingdom of Saudi Arabia(KSA)
Pharmacovigilance, according to Harmark and van Grootheest (2008) issued on behalf of World Health Organization (WHO), is “the science and activities relating to the detection, evaluation, understanding, and prevention of ADRs or any other drug-related problems.” This concept is very widely used and crucially involves information about ADRs. The collection of such data, originally initiated by the thalidomide tragedy in the 1960s, tries to ensure that all drugs are safe and effective in use by preventing any ADRs occurring in the future based on reporting of ADRs as they occur [1].
ADRs are a global problem and cause high levels of morbidity and mortality. The KSA has been a member of the WHO international drug monitoring program since 2009. The independent organisation, Saudi Food and Drug Authority (SFDA), plays an important role for monitoring drugs and protect everyone in Makkah, whether citizens all year round and pilgrims during Hajj and Ummrah, ensuring that the drugs they take are as safe as possible, they also have created programmes such as post-marketing surveillance. The KSA government invested significantly in this scheme to improve the public health services [2].
ADR reporting is the cornerstone for Pharmacovigilance several countries have formal ADR reporting programmes so that physicians who detect serious ADRs are able to report their observations. Hospital pharmacists, community pharmacists, nurses and even patients have the eligibility to report ADRs in many countries of the world. Furthermore, Pharmacists play a major role in detecting and reporting ADRs, more than any other health professionals [2-4]. The attitude and awareness towards ADRs reporting shows great variation among the health professionals and pharmacists and many factors influences the reporting of ADR.
a) To determine and evaluate awareness, knowledge and attitude of community pharmacists towards ADRs in Makkah, KSA.
b) To study factors influencing their reporting by health professionals.
The present cross sectional study was conducted during the months of July, August and September, 2010 in Makkah, KSA. In 2010, the Health Affairs Directorate register listed 339 private community pharmacies in Makkah as being authorized by the MOH. 220 pharmacists were contacted to participate in the study. But 50 pharmacists declined to take part in the study because they were unwilling, or needed to have authorization from the owner (manager) or were too busy to participate. Thus total 170 pharmacists participated in the study. The study was fully explained to the participating health professional and they were assured about the anonymity and confidentiality of the data. The responses of the health professionals were collected on a pre-structured questionnaire either obtained at the same time as the distribution or collected later time if the pharmacist was busy. The questionnaire comprised of 5 groups of questions i.e. part A, B, C, D and E. The part A consists of Demographic information of health professionals. Information about Familiarity with the ADR reporting system was covered in part B. Purpose of the ADR reporting system was in part in C. Attitude towards ADR reporting and Constraint of ADR reporting in the Makkah was collected in part D and E respectively. Questions where possible were worded as a series of statements and the community Pharmacists were asked to indicate their agreement or disagreement on a 4 point Likert scale from ‘strongly agree’ to ‘strongly disagree’.
Total 170 pharmacists participated in the study and the overall response rate for the study was 77.27%. The major reasons for nonparticipation were being too busy and/or unwilling to participate. Results of part A were shown in table 1. Out of total 170 participants all were male. No females took part due to the convention in KSA of females not being employed as community pharmacists. Most of the patricians were in the age group of 23-30 yrs (56%). 82% of pharmacists were having bachelors’ degree. 62% were having experience between 1-5 yrs. Most of pharmacists were registered with Saudi council for Health Specialties (SCHS) in the years 2006-2007. 88% pharmacists were not having internet facility at work place. 64% were using British National Formulary (BNF) for reference.
| Variable | Number (%) |
|---|---|
| Pharmacists contacted | 220 |
| Pharmacists declined to participate in the study | 50 (22.73%) |
| Pharmacists participated in the study (response rate) | 170 (77.23%) |
| Sex | |
| Male | 170 (100) |
| Female | 0 (0) |
| Age in Years | |
| 23-30 | 95 (56%) |
| 31-40 | 65 (38%) |
| >40 | 10 (6%) |
| Pharmaceutical Education | |
| Bachelor | 139 (82%) |
| Master PhD degree Other qualifications |
29 (17%) 00 (0%) 02 (1%) |
| Pharmacist Experience in years | |
| 1-5 | 108 (62%) |
| 6-10 | 31 (18%) |
| > 10 | 31 (18%) |
| Nationality | |
| Saudi | 43 (25%) |
| Non-Saudi | 127 (75%) |
| Year of registration with Saudi council for Health Specialties (SCHS) | |
| 2007 | 73 (43%) |
| 2006 | 65 (38%) |
| 2002 | 32 (19%) |
| Continuing education hours per month | |
| None | 90 (53%) |
| 1-5 hours | 39 (23%) |
| 6-10 hours | 41 (24%) |
| Internet facilities in your workplace | |
| Yes | 20 (12%) |
| No | 150 (88%) |
| References available* | |
| Middle East Drug Index | 49 (29%) |
| Martindale | 00 (00%) |
| British National Formulary (BNF) | 109 (64%) |
| Saudi National Formulary (SNF) | 49 (29%) |
| MIMS | 00 (00%) |
| None | 00 (00%) |
Table 1: Part A: Demographic information of Health professionals.
Part B: Familiarity with the ADR reporting system
The part B of questionnaire consisted of familiarity of pharmacist with ADRs system. It was observed that only 18% were aware of the ADR system whilst, 82.35% (n=140) were not aware. According to majority of community pharmacists 65% had no available systems in place for an ADR reporting at the workplace while 35% did have such facilities available to them. It was observed that 56% (n=100) of the community pharmacists were unaware of the existence of the NPC and they also had a poor awareness of the SFDA 41% (n=70) had some awareness of NPC. According to 65% respondents, ADR should be informed to the MOH and 29% of community pharmacists claimed that they submitted ADR reports to the SFDA. One person had actually submitted ADR reports directly to the relevant pharmaceutical companies. None of the community pharmacists stated that during the last month they had come across an ADR that they wished to report to the MOH or to a pharmaceutical company.
Part C: The purpose of the ADR reporting system
According 53.24% of surveyed community pharmacists the main purpose of ADR reporting was to identify safe drugs. Whereas 29% considered that it would be useful to calculate the rate of incidence of ADRs and 6% considered of community pharmacists stated the purpose of the ADR reporting system was to identify ADR within the same pharmaceutical class and 12% of community pharmacists considered the purpose of the ADR reporting was to detect potential ADRs simply. And according to 6% the system served as a source of information about the characteristics of ADRs (Figure 1).
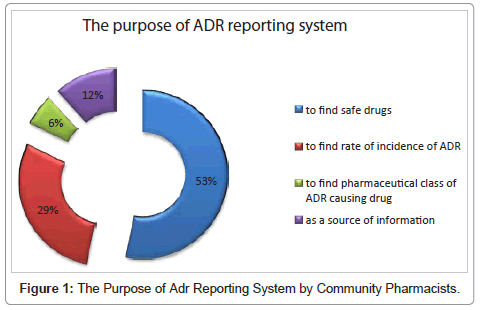
Figure 1: The Purpose of Adr Reporting System by Community Pharmacists.
Part D: Attitudes of community pharmacists’ towards the ADR reporting system
According to 38.80% of participants ADR reporting was the responsibility of pharmacists whereas 32.90% stated that it was the responsibility of physicians (Figure 2). 65% (n=110) of respondents considered the reporting of ADRs to be an integral part of the professional roles of the pharmacist’s duties and all community pharmacists decided to report after the researcher had explained the importance of ADRs reporting.
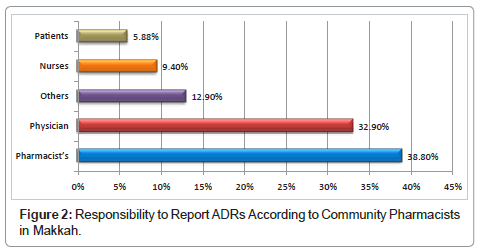
Figure 2: Responsibility to Report ADRs According to Community Pharmacists in Makkah.
Although 29.41% (n=50) of the community pharmacists believed that ADRs reporting to facilitate the science of monitoring drug safety was important. Also, 94% (n=160) responded they indicated that they must be sure of the causality between the drug and ADR it was essential to be certain about an effect before reporting. Nevertheless, 88.23% (n=150) of community pharmacists saw reporting as an integral part of the pharmaceutical task and 70.5% (n=120) said that ADR reporting was an indication of taking patients’ complaints seriously. 35.29% (n=60) of respondents believed to get more information about ADRs that they may come across during their professional practice. 76.47% (n=130) of respondents felt the need to discuss the report with the prescriber before reporting. The vast majority of the community pharmacists (94.11%) decided that the ADRs reporting should be a role for all community pharmacists to prevent any patients risk and also for community pharmacist’s provider to take care of public safe medication (Table 2).
| Statement | Participants agreed (%) |
|---|---|
| Reporting ADRs is part of the professional role of a pharmacist | 110 (65%) |
| I believe that the science of monitoring drug safety is important | 50 (29.41) |
| I want to be sure that the ADRs is related to the drug before reporting | 160 (94%) |
| I report for getting more information about ADRs questions that I come across in my profession practice | 60 (35.29%) |
| I report to show the patient that their concerns are being taken seriously | 120 (70.5%) |
| I always report ADRs because it is part of tasks | 150 (88.23%) |
| Consulting the physicians is important before reporting ADRs | 130 (76.47%) |
| ADRs reporting should be compulsory | 160 (94.11%) |
| ADRs reporting should be voluntary | 10 (5.88%) |
Table 2: Attitudes of Community Pharmacists.
The majority of respondents about 40% (n=68) commented that, these effects are caused by reporting mainly on “life threatening situation”. Maybe astonishingly, most of community pharmacists 45.2% (n=77) stated that they had come across a patients to the pharmacy with ADRs during the last month and community pharmacists wished to report it (Table 3). Actually, 47% (n = 80) were submitting a ADRs report to MOH in Makkah (Figure 3).
| Have you come across patient(s) with ADRs during last month and wished to report it? | Number | Percentage |
|---|---|---|
| Yes | 77 | 45.2% |
| No | 52 | 30.5% |
| I don’t know | 41 | 24.1% |
| Total | 170 | 100% |
Table 3: Proportion who encountered patient(s) with adrs during previous month and had wished to report it.
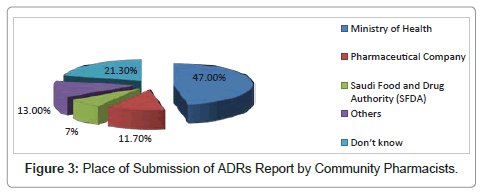
Figure 3: Place of Submission of ADRs Report by Community Pharmacists.
Part E: Constraint of ADR reporting
Constrains in reporting of ADRs were also evaluated. It was found that according to 59% pharmacists ADR reporting forms were not available where as 29% did not know the address to which the reports should be sent. According to 23%, reporting forms are too complicated. 17.6% believed that they had insufficient clinical knowledge about ADR reporting whereas 23% consider that the process was too time consuming. 41.17% of participant pharmacists believed that all severe ADRs had already been detected for a newly marketed drug. 52% of community pharmacists believed that they may not care about it (Figure 4).
The present study was conducted with the aim to determine and evaluate awareness of knowledge and attitude of community pharmacists towards ADRs. Totally 170 community pharmacists participated in the study. All the participants were male. No females took part due to the convention in KSA of females not being employed as community pharmacists.
The findings of this unique study of community pharmacists, which turned out to be in the majority, male, middle-aged Egyptians with a bachelor’s degree employed in Makkah, showed that majority of participants strongly agreed that ADR reporting is part of their professional duties and responsibilities. Against this background it was very surprising to find that the majority were not aware of the ADR reporting program. Similarly, a lack of awareness of the system of reporting is similar to results previously reported in community pharmacists in Hong Kong by Lee et al. [5], where the average who were not aware of the systems was 88% and a study in Riyadh city by Bawazir [6] found that 87% were not aware of the system. And in Iran a study by Vessal et al. [7] showed that 87% were unaware of ADR reporting systems. However, these figures were better than those reported for example in the Netherlands, where 99% were unaware of the ADR reporting system by Van Grootheest et al. [8].
All these findings may indicate a need for cooperation between all organizations, so as to work together to put programs into place and plan for the long-term training all of healthcare professionals in regards to ADRs reporting and Pharmacovigilance. This should raise their awareness and ensure that the next generation of pharmacists is more knowledgeable about the subject. Clearly there is a need for community pharmacists to be educated about the ADR reporting system, especially expatriates, such as the Egyptians in KSA who may not be familiar with the country’s rules and regulations and perhaps did not receive any education about it in their bachelor’s degree.
The present study showed that reporting rate to the NPC via the internet was low. It may be because of the fact that 88% (n=150) of community pharmacists in the Makkah did not have access to the internet in their workplace. By contrast, even if computer access were made available then 56% (n=90) of the respondents who were not aware of the existence of the NPC within the SFDA and were also unaware of the system of reporting ADR through the appropriate channel and filling in the forms to report ADR, would still pose a problem.
It was also observed that majority of community pharmacists were having poor knowledge about ADR and Pharmacovigilance, which may be one of the reason for declining to participate in study and fear to report ADRs. Similar findings were also reported by Toklu and Uysal [9] in their study. Though the knowledge of pharmacists was poor about ADR a clear positive attitude towards ADR reporting was observed. Majority of pharmacists (94%) stated that reporting suspected ADR as a professional obligation and considered ADR reporting as the responsibility of physicians, pharmacists and patients. 88% of respondents considered ADR reporting an integral part of pharmaceutical care. These results were very similar to figures reported for community pharmacists in the Netherlands by Van Grootheest et al. [8] and similar results of community pharmacists in Riyadh city, KSA [6], in the UK by Green et al. [10] and in Norway by Granas et al. [11].
According to 96% (n=160) pharmacists, they must be sure of the relation between ADR and the drug before reporting it. Similar responses were reported by pharmacists and physicians in different countries such as; by Bawazir [6] from KSA, Green et al. [10] from the UK, Vessal et al. [7] from Iran and by Van Grootheest et al. [8] from the Netherland. The pharmacist uncertainty may reflect the fear of making errors due to a lack of comprehensive patient details, and any problems which would occur may reflect badly on their professional image. This problem could be addressed by exposing pharmacists to the ADR system during their undergraduate studies and by conducting a series of workshops to reduce their concerns and to strengthen clinical confidence in the reporting of an ADR. Consequently, 76% (n=130) of community pharmacists felt that they should discuss the ADR reports with physicians before submitting it, indicating a lack of confidence and desire to avoid any legal action that may come about. This is a similar finding to the present study observed in studies carried out in the Netherlands and with community pharmacists in Riyadh KSA [6,7,12].
The present study and other studies carried out in other communities and hospital pharmacists in many different countries, showed that there was low awareness of the ADR reporting programme.
Alhazmi and Naylor [2] concluded the study for healthcare professionals in the Makkah including hospital pharmacists as positive awareness and knowledge toward ADRs reporting by relevant increasing training and education would engender a reporting culture that may lead to the establishment of a Pharmacovigilance centre in the region.
In a study conducted by Van Grootheest et al. [7] reported that the countries which rely heavily on ADR reporting programmes, namely, Canada, Australia, Japan, Spain and Portugal had received 88.3%, 40.3%, 40.2%, 39%, 26%, and 23% of ADR reports by community and hospital pharmacists respectively. This finding should encourage the administrators of KSA Healthcare programmers to invest in educating, training and practicing of reporting ADR by community pharmacists in Makkah.
Major constrain in reporting of ADR was unavailability of forms. Most of the community pharmacists considered the process as being too time consuming. Insufficient clinical knowledge was also observed among the community pharmacists. These barriers could simply be overcome by making the reporting forms available easily, reducing the complexities of the forms. The other barriers were pharmacists’ knowledge about ADR and uncertainty regarding the causality relationship between a drug and an adverse effect. To reduce these barriers, there is an urgent need to train community pharmacists by providing educational programmers about ADR reporting and Pharmacovigilance. Similar solutions to overcome such barriers were reported by physicians and pharmacists by Lee et al. [5], Green et al. [10], Van Grootheest et al. [7], Bawazir [6], Granas et al. [11], Toklu and Uysal [9], Bawazir and Al-Sultan [12], Vessal et al. [7] and Al Hazmi and Naylor [2].
In the end we can conclude that most of community pharmacists were unaware about ADR reporting system and were having poor knowledge about ADR and Pharmacovigilance. Though the knowledge was poor most of them consider that main purpose of ADR reporting was to identify safe drugs and they were ready to participate in ADR reporting if they were being trained to these procedures. Thus Community pharmacists practicing in KSA should be encouraged to address the concept of ADR reporting and the procedure should be made easy and less time consuming.
The authors would like to thank the MOH of Makkah, KSA for their permission to carry out this study and the community pharmacists in Makkah who gave their time and effort by providing data for use in this study which will contribute to a PhD thesis by Naif Al-Hazmi.