Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Case Report - (2016) Volume 6, Issue 5
Dyke-Davidoff-Masson syndrome (DDMS) refers to atrophy or hypoplasia of one cerebral hemisphere (hemiatrophy), which is usually due to an insult to the developing brain in fetal or early childhood period. The clinical features are variable and depend on the extent of brain injury. More commonly they present with recurrent seizures, facial asymmetry, contralateral hemiplegia, mental retardation or learning disability and speech and language disorders. The classical radiological findings are cerebral hemiatrophy, calvarial thickening, and hyperpneumatiztion of the frontal sinuses [1].
The condition is usually diagnosed in childhood but, in rare cases the condition is diagnosed in adolescent or adult years. We report two cases of DDMS, where both patients presented in a similar manner. Here we present a case of a 54-year old male and another case of a 46 year old male, both patients presented with Generalized Tonic Clonic seizures, Hemiparesis of the left arm and leg along with characteristic radiological findings.
DDMS was first described by C.G Dyke, L.M Davidoff and C.B Masson in 1933 in a series of nine patients with plain skull radiographic and pneumatoencephalographic changes. The condition is characterized by cerebral hemiatrophy, facial asymmetry, thickening or thinning of cranial vault, contralateral hemiplegia or hemiparesis, seizures and mental retardations [2].
Diagnosis is usually conducted by clinical examination and radiological studies. The condition is usually diagnosed in childhood but, in rare cases the condition is diagnosed in adolescent or adult years. We report two cases of DDMS, where both patients presented in a similar manner. Here we present a case of a 54-year old male and another case of a 46 year old male, both patients presented with Generalized Tonic Clonic seizures, Hemiparesis of the left arm and leg along with characteristic radiological findings (Figure 1).
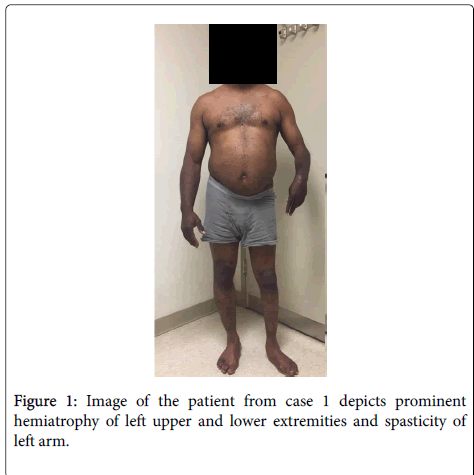
Figure 1: Image of the patient from case 1 depicts prominent hemiatrophy of left upper and lower extremities and spasticity of left arm.
Case 1
A 54-year old male presented with a history of seizure disorder, cerebral palsy, chronic lower back pain and degenerative joint disorder of cervical spine. Patient was unaware of any known history of significant antenatal or perinatal complications. Patient has had Generalized Tonic Clonic seizures since the age of five. Patient has left sided hemiparesis since birth along with hypereflexia.
The patient is currently taking Dilantin 100 mg TID and Keppra 750 mg BID for seizure management. However, he continued to have seizures intermittently as a result of non-compliance. The patient did not show any sign of cognitive loss or deficits and he continues to hold an occupation and sustain family life. However, mobility of the patient is limited and he walks with a limp as a result of the left sided hemiparesis.
Neurological findings
1. Motor strength 3/5 on the left upper and lower extremity
2. Left leg muscle atrophy, spasticity on the left arm and pronated left hand
3. Decreased sensation on the left side
4. Motor strength and sensation intact on the right upper and lower extremity
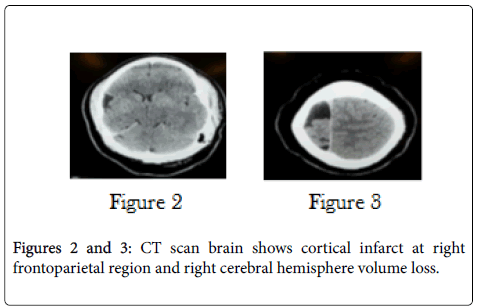
CT scan results demonstrated volume loss in the right cerebral hemisphere with peripheral areas of decreased attenuation which may represent encephalomalacia /old infarct/ congenital abnormality. Visualized paranasal sinuses show mucoperiosteal thickening of the ethmoid sinuses (Figures 2 and 3).
Figures 2 and 3: Representative photomicrograph of histopathological features in pulmonary necropsies.
Diagnosis was primarily derived upon the patient’s clinical presentation, chronic history of Generalized Tonic Clonic seizures, and hemiparesis along with hyperreflexia. The characteristic radiological findings of cerebral hemisphere volume loss and the appearance of old infarct along the distribution of middle cerebral artery further strengthened the diagnosis of Dyke Davidoff Masson Syndrome.
The patient was recommended to continue the prescribed antiepileptic medications along with physiotherapy regimen to improve the overall quality of life.
Case 2
A 44 year old male presented with a history of seizure disorder (last episode in 1985), left sided hemiparesis along with hyperreflexia in left upper and lower extremities, hypertension and dyslipidemia. Patient is being followed regularly by a neurologist and is complaint with his medications. Patient began to have Generalized Tonic Clonic seizures at an early age. The patient is currently taking Carbamazepine 200 mg PO am, 200 mg PO noon and 300 mg PO hs for seizure management. Patient was unaware of any known history of significant antenatal or perinatal complications. As with the patient in Case 1, patient in Case 2 also did not show any sign of cognitive loss or deficits and our patient continues to hold an occupation and sustain family life. However, mobility of the patient is limited and the patient walks with a limp as a result of the left sided hemiparesis (Figures 4 and 5).
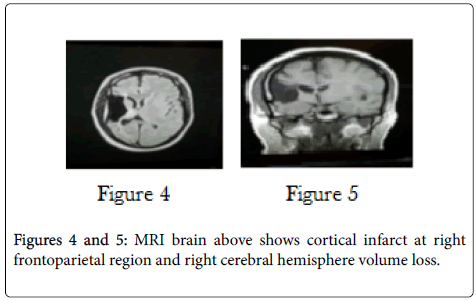
Figures 4 and 5: MRI brain above shows cortical infarct at right frontoparietal region and right cerebral hemisphere volume loss.
Neurological findings
1. Motor strength was 4/5 in left upper and 5/5 in left lower extremity
2. Left-sided atrophy with mild rigidity in the left forearm muscles with flexion deformity of the left elbow joint
3. Sensation was intact in bilateral extremities
4. Hyperflexia was noted in left upper and lower extremities
5. Upgoing Babinski reflex on the left
6. Range of motion in the left elbow is restricted with mild flexion deformity
MRI studies demonstrated volume loss in the right cerebral hemisphere with left to right shift of the midline indicating an infarct early in development. Right Middle Cerebral Artery distribution showed remote infarction likely occurred during early development. There is compensatory underdevelopment of the right calvarium. There is also asymmetric underdevelopment of the right cerebral peduncles and right ventral pons corresponding to Wallerian degeneration or underdevelopment of right cortical spinal tract fibers.
Diagnosis was primarily derived upon the patient’s clinical presentation, chronic history of Generalized Tonic Clonic seizures, and hemiparesis along with hyperreflexia. The characteristic radiological findings of cerebral hemisphere volume loss and the appearance of old infarct along the distribution of middle cerebral artery further strengthened the diagnosis of Dyke Davidoff Masson Syndrome.
The patient was recommended to continue the prescribed antiepileptic medications along with physiotherapy regimen to improve the overall quality of life.
In 1933, Dyke, Davidoff, and Masson described the plain skull radiographic and pneumatoencephalo graphic changes in their series of nine patients whose clinical characteristics included hemiparesis, seizures, facial-asymmetry, and mental retardation. It has been reported that Dyke Davidoff -Masson Syndrome occurs in intrauterine life when the maturation of calvarium has not been completed, or due to brain damage (usually traumatic) occurring in first 3 years of life. The etiological factor for Dyke-Davidoff-Masson syndrome has been postulated as trauma, inflammation or vascular malformations and occlusions. When the insult occurs in-utero, it could be due to gestational vascular occlusion, primarily involving the middle cerebral vascular territory. Clinically, patients present with seizures, facial asymmetry, contralateral hemiparesis and mental retardation. Both our patients have similar presentations - seizures since childhood, hemiparesis along with hyperreflexia [3]. Both our patients presented with significant right cerebral hemisphere volume loss and left to right midline shift along with evidence of old infarct appearing on the radiological studies. Hence, a comprehensive clinical history and CT or MRI provides the right diagnosis. MRI is a valuable method of examination in the analysis of cerebral hemiatrophy as it has the ability to bring to light changes in the cerebral hemispheres as well as highlighting bony structural changes and thus differentiating between congenital and acquired types of DDMS [4].
Hemispherectomy is the treatment of choice with a success rate of 85% in selected cases. However, if the presentation is late as in our two cases, the patients should remain on antiepileptic medications in spite of surgery [1]. Apart from this, the patients should also be recommended for supportive therapy including physiotherapy, speech therapy, and occupational therapy to improve overall quality of life. Further longitudinal studies are required to ascertain the natural course of this syndrome especially in an adult population, which would help in planning strategies regarding the time and nature of interventions and management accordingly [1].