Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Editorial Comment - (2016) Volume 0, Issue 0
This prospective clinical trial summary provides the background and rationale for evaluating optimal radiation dose for definitive concurrent chemo-radiation for inoperable esophageal carcinoma. We designed the multi-center clinical trial comparing the efficacy of high dose group (60 Gy/30F) with low dose group (50 Gy/25F) concurrent with weekly chemotherapy using 3D-CRT or IMRT technology for esophageal carcinoma. The primary outcome is local/ regional progression-free survival, and secondary outcomes include Overall survival; local control rate; patterns of treatment failure; toxicity; radiation-related advent events.
Keywords: Concurrent chemo-radiation; Esophageal carcinoma; Radiation dose; Randomized trial
Esophageal carcinoma (EC) is one of the most fatal cancers in the world, and China is one of the high-incidence areas of all time. The overall 5 year survival rate for all EC patients is not better than 20% [1]. Different from the western countries, esophageal squamous cell carcinoma (ESCC) accounts for 95% of all Chinese EC patients [2]. Radiotherapy alone is one of the standard treatments of EC before 1980’s. With the advent of chemotherapeutic agents such as cisplatin and fluorouracil, people began to try the combination of radiotherapy and chemotherapy in the treatment of esophageal cancer. The landmark RTOG 85-01 [3] was undertaken to investigate whether primary treatment with both chemotherapy and radiotherapy was superior to radiation therapy alone in patients with EC. This phase III prospective, randomized, and stratified trial was undertaken to evaluate the efficacy of four courses of combined fluorouracil (1000 mg/m2 daily for four days) and cisplatin (75 mg/m2 on the first day) plus 5000 cGy of radiation therapy, as compared with 6400 cGy of radiation therapy alone. The trial was stopped after the accumulated results in 121 patients demonstrated a significant advantage for survival in the patients who received chemotherapy and radiation therapy. The median survival was 8.9 months in the radiation-treated patients, as compared with 12.5 months in the patients treated with chemotherapy and radiation therapy. In the former group, the survival rates at 12 months and 24 months were 33% and 10%, respectively, whereas they were 50% and 38% in the patients receiving combined therapy (P<0.001). In 1999, the authors reported the long-term outcomes of RTOG85-01 [4]. In the randomized part of the trial, at 5 years of follow-up the overall survival for combined therapy was 26% (95% confidence interval (CI), 15%-37%) compared with 0% following RT. In the succeeding nonrandomized part, combined therapy produced a 5 year overall survival of 14% (95% CI, 6%-23%). Severe acute toxic effects also were greater in the combined therapy groups. There were no significant differences in severe late toxic effects between the groups. According to the results of RTOG85-01, Concurrent chemoradiotherapy (CCRT) is established as a standard treatment option to treat inoperable locally advanced EC and chemotherapy based on cisplatin has also been confirmed as a standard concurrent regimen [1-3].
Although there was a significant improvement in local/regional control and overall survival with radiation plus chemotherapy compared with radiotherapy alone, the incidence of local/regional failure and local/regional persistence of disease was 47%. RTOG 94-05 [5] was undertaken to investigate whether high-dose radiation (64.8 Gy) could achieve better results than standard-dose (50.4 Gy). For the 218 eligible patients, there was no significant difference in median survival (13.0 v 18.1 months), 2 year survival (31% v 40%), or local/ regional failure and local/regional persistence of disease (56% v 52%) between the high-dose and standard-dose arms. The higher radiation dose did not increase survival or local/regional control. Although there was a higher treatment-related mortality rate in the patients assigned to the high-dose radiation arm, it did not seem to be related to the higher radiation dose. The standard radiation dose for patients treated with concurrent 5-FU and cisplatin chemotherapy is 50.4 Gy. CCRT with 50.4 Gy is still the standard treatment regimen for locally advanced EC in most western countries.
In China, there are many studies on the dose of radical radiotherapy for EC in the last century. A series of 221 EC patients admitted from 1983 to 1984 for radiotherapy was randomized into two groups: Group A (50 Gy/5 week, 111 patients), and Group B (70 Gy/7 week, 110 patients). There were 3 and 11 patients who did not complete their treatment in these groups. The 5 year survival rates of Group A and B were 16.7% and 17.2% (P>0.05). Due to the absence of superiority and higher incidence of discontinuation in the 70 Gy group, the authors believe that high dose regimen is not warranted for EC [6]. After ten years of follow-up, there was also no significant difference in survival between the two groups [7]. Sha [8] also reported a control study covering two hundred patients with EC who were randomized into two groups receiving a total dose of 50 Gy/5 weeks or 70 Gy/7 weeks for radiotherapy. All patients have been followed for more than 5 years. The results showed that there was no difference either in the tumor remission as shown on the X-ray films or in the 5 year survival rates between these two groups. The frequency of complications induced by radiation and the 1 year death rates were higher in the 70 Gy group. The authors believe that high dose of 70 Gy for EC is not warranted.
All of the above studies are based on the technology of two dimensional radiotherapy. Nowadays, three-dimensional conformal radiation therapy (3DCRT), or intensity-modulated radiation therapy (IMRT) has been used widely in EC. Xiao [9] assessed the dose distribution by 3D conformal radiation treatment comparing 2D conventional technique and enlarge field technique for the primary lesion and normal surrounding tissues around EC. The volumes of GTV, CTV covered by prescription dose were 37%, 38% and 27%, 33%, respectively for conventional technique and enlarge field technique. The volume of GTV and CTV covered by prescription dose was 95% and 100% in 3DCRT. The lung V20 was 23%, 31% and 20%, respectively. 3DCRT can well achieve ideal dose distribution and coverage to the target volumes and spare the normal tissues at the same time, as compared with the conventional and enlarged field radiotherapy techniques. Two dimensional radiotherapy has obvious dosage deficiency and cold-spot, which may be one of the main reasons of high local failure rate. Therefore, all results based on 2D radiation technology are worthy to be reevaluated. There is no prospective, randomized trial reevaluating the optimal radiation dose for definitive concurrent chemo-radiation in EC till now. So we conducted the prospective, randomized, multi-center clinical trial comparing the efficacy of high dose group (60 Gy/30 F) with low dose group (50 Gy/25 F) concurrent with weekly chemotherapy using 3DCRT or IMRT technology for ES. We have completed the registration on the ClinicalTrial website. The number is NCT01937208.
The primary objective is local/regional progression-free survival. Secondary objectives include: Overall survival; local control rate; Patterns of treatment failure; toxicity; radiation-related advent events.
Eligibility criteria
The main inclusion criteria are: (1) histological or cytologic confirmed esophageal squamous cell carcinoma; (2) medically inoperable or patient refusal; (3) clinical stage from IIA to IVA (AJCC 2002 edition); (4) age 18-70 years; (5) Karnofsky Performance Status (KPS) of at least 70; (6) joined the study voluntarily and signed informed consent form; (7) patients must not have received any prior anticancer therapy; (8) Target lesions can be measured according to RECIST criteria; (9) no serious system dysfunction and immunodeficiency; (10) adequate organ function including the following: Hemoglobin ≥ 9 g/dl, WBC ≥ 3 × 109/L, Neutrophils (ANC) ≥ 1.5 × 109/L, platelet count ≥ 100 × 109/L, TBIL<1.5 × ULN, ALT and AST ≤ 2.5 × ULN, creatinine ≤ 1.5 × ULN;(11) life expectancy of more than 3 months.
Exclusion Criteria mainly include: (1) multiple carcinomas of the esophagus; (2) biopsy-proven invasion of the tracheobronchial tree or tracheoesophageal fistula; (3) a primary tumor that extended to within 2 cm of the gastroesophageal junction; (4) prior chemotherapy, prior thoracic radiation, surgical resection of the primary tumor; (5) concurrent pregnancy or lactation; (6) history of a second malignancy other than nonmelanoma skin cancer.
Pretreatment evaluation
Routine pretreatment evaluations included physical examination, complete blood cell count and biochemistry, esophageal barium X-ray, endoscopy of the upper gastrointestinal tract and biopsy of primary tumor, CT of neck, chest and upper abdomen. 18F-fluorodeoxyglucose positron emission tomography (PET) were optional. All patients were clinical staged based on the AJCC TNM classification of malignant tumors (2002).
Radiation plan
Radiation had been delivered by three-dimensional conformal radiation therapy, or intensity-modulated radiation therapy. All patients underwent CT simulation in the supine position, with CT images obtained at a 5 mm thickness throughout the entire neck, thorax and upper abdomen. The gross tumor volume (GTV) includes primary tumors (GTV-T) and lymph node metastasis (GTV-N). GTVT included all esophageal tumors, which were found by CT scan, esophageal bariumendoscopy, endoscopic ultrasonography and PET/CT. The definitions of GTV-N (to meet one) were as follows: Nodes greater than 1.0 cm in the shortest axis in the intra-thoracic and intra-abdominal region [10-12] and greater than 0.5 cm beside the recurrent nerve [10,11] on CT scans or with a high standardized uptake value-max of 18F-deoxyglucose avid on PET/CT images [12]. CTV-T was defined as 3 cm supero-inferior margins and a 0.6 cm lateral margin from the GTV-T. We recommended CTV-N should include cervical and upper mediastinal nodes for lesions in the upper thoracic esophagus. Upper, middle/lower mediastinal and abdominal nodal regions should be involved in the middle thoracic EC. For lesions in the lower thoracic esophagus, the CTV-N should cover the middle, lower mediastinal and abdominal lymph nodes regions. The planning target volume (PTV) was generated by adding a uniform 5mm margin around the CTV (CTV-T+CTV-N). Prescribed dose is given to the PTV. Total dose of 60 Gy/30F in high dose group and 50 Gy/25 F in low dose group was given in 6 weeks or 5 weeks with five fractions per week.
Radiation had been delivered by three-dimensional conformal radiation therapy, or intensity-modulated radiation therapy. All patients underwent CT simulation in the supine position, with CT images obtained at a 5 mm thickness throughout the entire neck, thorax and upper abdomen. The gross tumor volume (GTV) includes primary tumors (GTV-T) and lymph node metastasis (GTV-N). GTVT included all esophageal tumors, which were found by CT scan, esophageal bariumendoscopy, endoscopic ultrasonography and PET/CT. The definitions of GTV-N (to meet one) were as follows: Nodes greater than 1.0 cm in the shortest axis in the intra-thoracic and intra-abdominal region [10-12] and greater than 0.5 cm beside the recurrent nerve [10,11] on CT scans or with a high standardized uptake value-max of 18F-deoxyglucose avid on PET/CT images [12]. CTV-T was defined as 3 cm supero-inferior margins and a 0.6 cm lateral margin from the GTV-T. We recommended CTV-N should include cervical and upper mediastinal nodes for lesions in the upper thoracic esophagus. Upper, middle/lower mediastinal and abdominal nodal regions should be involved in the middle thoracic EC. For lesions in the lower thoracic esophagus, the CTV-N should cover the middle, lower mediastinal and abdominal lymph nodes regions. The planning target volume (PTV) was generated by adding a uniform 5mm margin around the CTV (CTV-T+CTV-N). Prescribed dose is given to the PTV. Total dose of 60 Gy/30F in high dose group and 50 Gy/25 F in low dose group was given in 6 weeks or 5 weeks with five fractions per week.
Concurrent and consolidation chemotherapy
From the first day of thoracic radiotherapy, all Patients were given weekly doctaxel (25 mg/m2 IV over 60 min) followed by cisplatin (25 mg/m2 IV over 30 min). Radiation was generally administered after chemotherapy. Dexamethasone (10 mg IV) and diphenhydramine (50 mg IV) were given 30 min before treatment. Two groups were both treated with concurrent chemotherapy for 5 weeks. Chemotherapy was withheld if grade 3/4 toxicity developed, and doctaxel and cisplatin were restarted at a 10% dose reduction if the severity decreased to grade 3 or less. After the completion of concurrent chemoradiation, the patients have a 3-4 weeks rest, and then receive 2 cycles’ consolidation chemotherapy with doctaxel 70 mg/m2 plus cisplatin 25 mg/m2 day 1-3 (Figure 1).
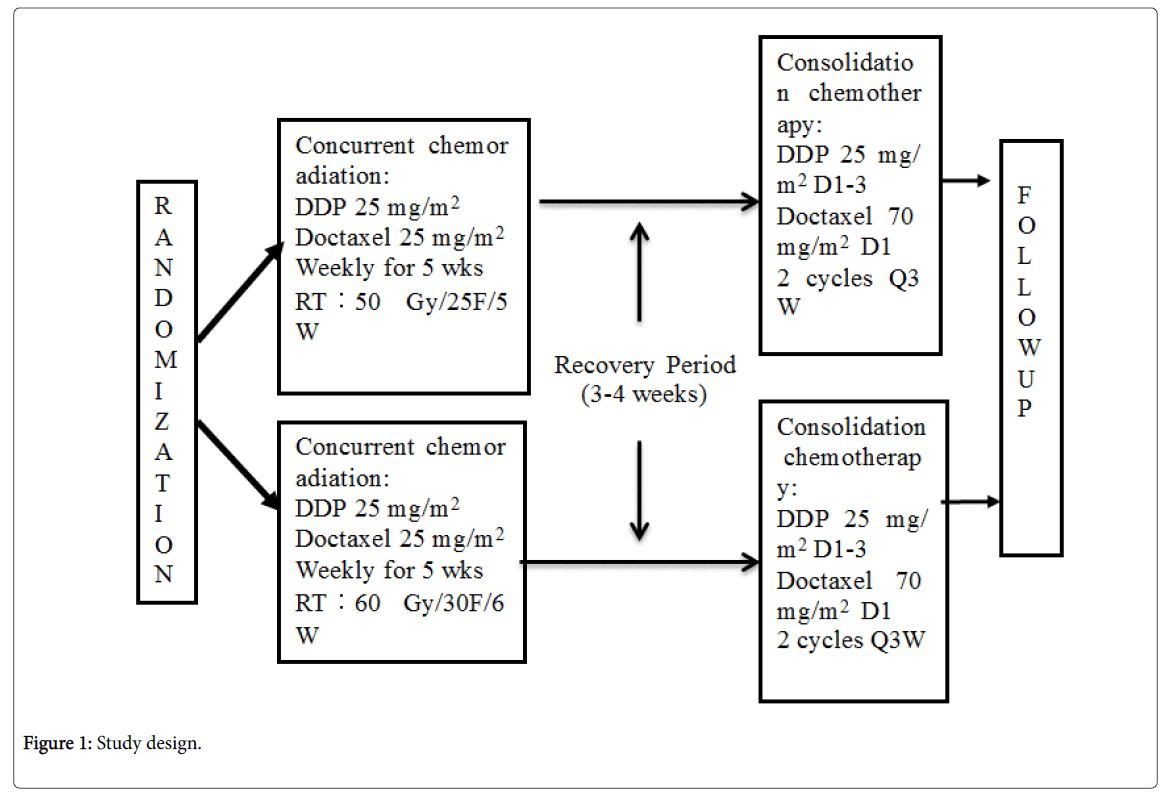
Figure 1: Representative photomicrograph of histopathological features in pulmonary necropsies.
A total of 300 patients will be randomized equally between the 2 arms. This will provide a minimum power of 80% to detect an HR of 0.74 at a 2 sided type-one error rate of 5%.
All enrollment patients were examined weekly throughout all phases of the treatment. Before weekly chemotherapy, physical examination and toxicity assessment were performed. Weekly radiation-related toxicity assessment was performed during radiation therapy. Radiation-related toxicity was classified as either acute (occurring within the first 90 days of irradiation) or late (occurring either 90 days or persisting beyond 90 days after irradiation) and was scored according to RTOG toxicity criteria. The highest score noted was recorded as the patient’s toxicity grade.
A history and physical examination, serum chemistry profile, barium swallow, Chest, upper abdomen CT scan and quality of life analysis was performed within 28 days after the completion of concurrent chemo-radiotherapy and all therapy. The following were performed until the time of disease progression every 3 months for 1 year, every 4 months for 2 years, then 6 months for over 3 years: physical examination, toxicity assessment, complete blood cell count, serum chemistry profile, chest X-ray, barium swallow and upper gastrointestinal, abdominal, and chest CT scan, and quality of life assessment.
We will collect the patient’s peripheral blood samples (including EDTA vacuum anticoagulant tube and common test tube, each of which is about 5 ml) before the treatment, 2, 4 weeks after radiation therapy and at the end of concurrent chemo-radiotherapy and all therapy as well. After collecting the samples, centrifugation should be completed as soon as possible in 30 minutes and try not to exceed 4 hours. After centrifugation, the specimens were placed in ultra-low temperature refrigerator for future molecular detection. We hope to find some useful molecular markers to select the different EC patients with different radiation sensitivity.
Author declares no conflict of interest.