Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Case Report - (2016) Volume 5, Issue 5
A 27-year-old woman was referred to our office for a dental assessment regarding temporomandibular joint pain. On initial screening, she was found to be at high risk for obstructive sleep apnea, and subsequently underwent polysomnography, which revealed an apnea-hypopnea index of 118 hr-1. Her condition was initially controlled with continuous positive airway pressure therapy, which she did not tolerate well. Therefore, treatment proceeded with biomimetic oral appliance therapy. After 10 months of combined continuous positive airway pressure therapy and biomimetic oral appliance therapy, the apnea-hypopnea index fell to 1 hr-1 and obstructive sleep apnea could not be observed with or without the appliances in situ. We conclude that combined continuous positive airway pressure therapy and biomimetic oral appliance therapy might represent a potential cure for severe cases of obstructive sleep apnea in certain patients.
Keywords: Severe obstructive sleep apnea, Biomimetic oral appliance therapy
Obstructive sleep apnea (OSA) is a highly prevalent condition that is a health burden affecting virtually every specialty in medicine [1-4] as it may be the root cause of many chronic conditions [5]. In addition, the all-cause mortality risk is significantly increased in patients with sleep disordered breathing if left unmanaged [6]. Currently, it is thought that OSA cannot be cured but only managed over the lifetime of a patient with: weight loss; surgical procedures; continuous positive airway pressure (CPAP) therapy; a mandibular advancement device (MAD) or a combination of these methods [7]. However, patient adherence with CPAP devices is low and many people suffer from untreated, severe OSA. There also can be problems with undesirable craniofacial changes with long term use of CPAP [8]. Similarly, unwanted side effects of long-term MAD use have been reported [9]. Therefore, the following case study demonstrates a novel protocol that may represent a potential cure for OSA in a patient diagnosed with severe OSA who was unable to comply with CPAP therapy.
A 27-year-old female was referred to a dental practice for evaluation of temporomandibular joint (TMJ) pain. History taking revealed that she was a severe snorer, had a long history of obesity, migraine-like headaches, facial/jaw pain, ringing in the ears, and stiff muscles in the neck and back. She also had a history of nocturnal bruxism, as well as popping and clicking in both TMJs. In addition, she admitted to chronic daytime fatigue, problems with insomnia, memory and intellectual impairment, and had trouble breathing through her nose. She had been told that she stops breathing at night.
Initial screening revealed an Epworth Sleepiness Scale of 8. Her vital signs were BP=115/78, P=83 bpm, oxygen saturation (SaO2)=98%, neck circumference 15 in (38 cm) and a BMI of 39 kgm-2. A detailed craniofacial examination, as well as an ambulatory sleep study, was performed by a general dentist to reach a working diagnosis in collaboration with medical sleep specialists. The differential diagnoses included: OSA, tonsillar hypertrophy with possible pathology and airway obstruction, sleep bruxism, and TMJ/craniomandibular disorder. Immediate referrals were made to a pulmonologist and otolaryngologist (ENT) for diagnosis and treatment. An urgent PSG was performed, which confirmed severe OSA; having an AHI of 118 hr-1 with a SaO2 nadir of 82%. The patient was started on CPAP therapy, and a CPAP pressure of 10 cm H2O seemed to be effective in correcting her OSA by reducing her AHI to O hr-1 with normal oxygen saturation in all stages of sleep. The final diagnosis from the sleep physician was severe OSA.
The ENT specialist found enlarged tonsils on the right side graded as 4+ and grade 3+ on the left side. There was no lymphadenopathy or masses within the neck. Flexible endoscopy showed the adenoids were grade 2+ with all laryngeal structures being within normal limits. The remainder of the head and neck exam was within normal limits. The risks and benefits of surgery to remove the tonsils and adenoids were discussed with the patient by the otolaryngologist, and she would be required to stay in the hospital overnight due to the diagnosis of severe OSA.
Following successful tonsillectomy, a home sleep test (HST) was obtained without CPAP, which revealed an AHI of 70 hr-1. The patient continued to use CPAP postoperatively but with increasing intolerance. After 8 months, the patient presented to our clinic once again, requesting an oral appliance, as she did not like CPAP therapy. Moreover, the patient wanted to try a novel, FDA-approved, biomimetic oral appliance (DNA appliance®, BioModeling Solutions, Inc., USA) that might re-develop her midfacial architecture combined with mandibular advancement. After obtaining informed consent, the device was offered as an option for this patient as long as she continued to wear the CPAP every night throughout the whole process. She agreed to have further HST studies to monitor any changes. The sleep specialist was informed of her decision to proceed with this treatment.
Following 9 months of oral appliance therapy for 12 h to 16 h per day and excellent patient compliance with CPAP, a 2-night HST was performed. The first night of the sleep study lasted 4 h and 37 min with the biomimetic oral appliance in situ. There were 72 snoring events with a mean SaO2 of 94% but little sign of OSA. The second night of the sleep study lasted 8 h and 39 min with no appliance in the mouth. There were 176 snoring events with a mean SaO2 of 90% but little sign of OSA. Thus, after 9 months of combined therapy, OSA could not be observed with or without the biomimetic oral appliance or CPAP in the 2-night study. The impression reported by a sleep specialist was, ‘No obstructive sleep apnea with or without the dental appliance’. Despite these results, the outcome was assessed further with another laboratory based polysomnograph, which confirmed the absence of OSA in all positions and all stages of sleep. There was 20% REM recorded during that sleep study, putatively indicating restoration of a more normal sleep architecture. The sleep study continued to be negative for OSA when tested without the CPAP or biomimetic oral appliance in situ, which the patient did not wear for 3 weeks prior to the sleep study.
Figure 1 shows the pre and post operative oropharyngeal region. Figure 2 shows the facial and nasal characteristics. Figures 3-5 show the dental occlusion before and after treatment.
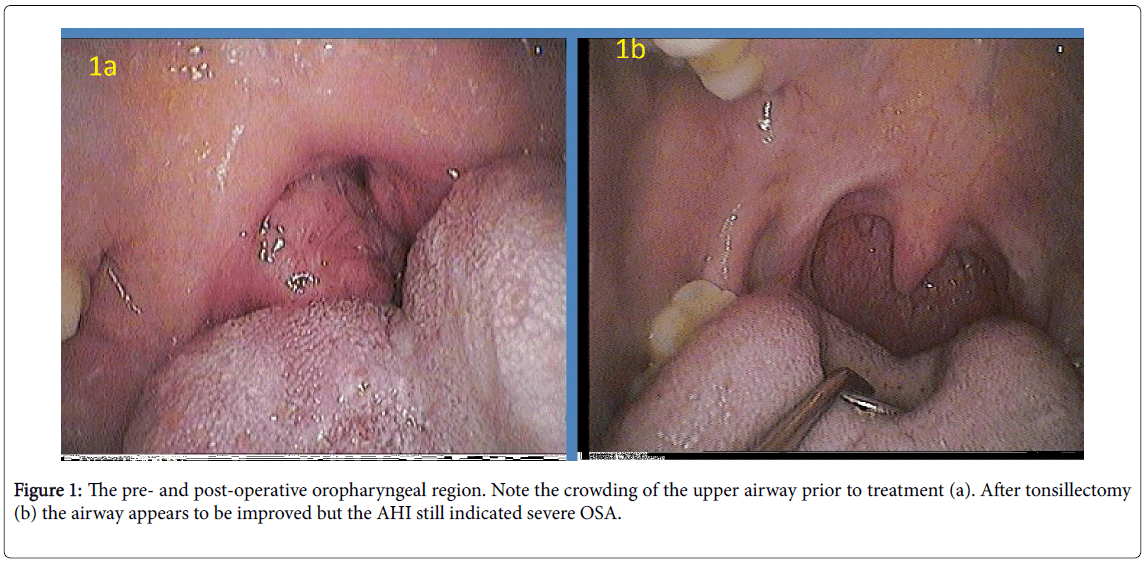
Figure 1: The pre- and post-operative oropharyngeal region. Note the crowding of the upper airway prior to treatment (a). After tonsillectomy (b) the airway appears to be improved but the AHI still indicated severe OSA.
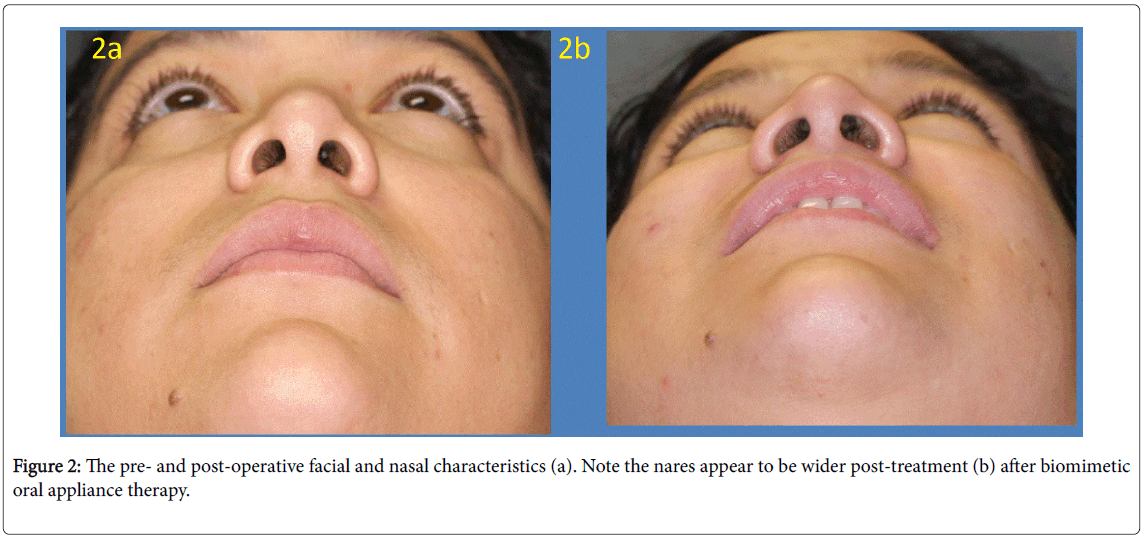
Figure 2: The pre- and post-operative facial and nasal characteristics (a). Note the nares appear to be wider post-treatment (b) after biomimetic oral appliance therapy.
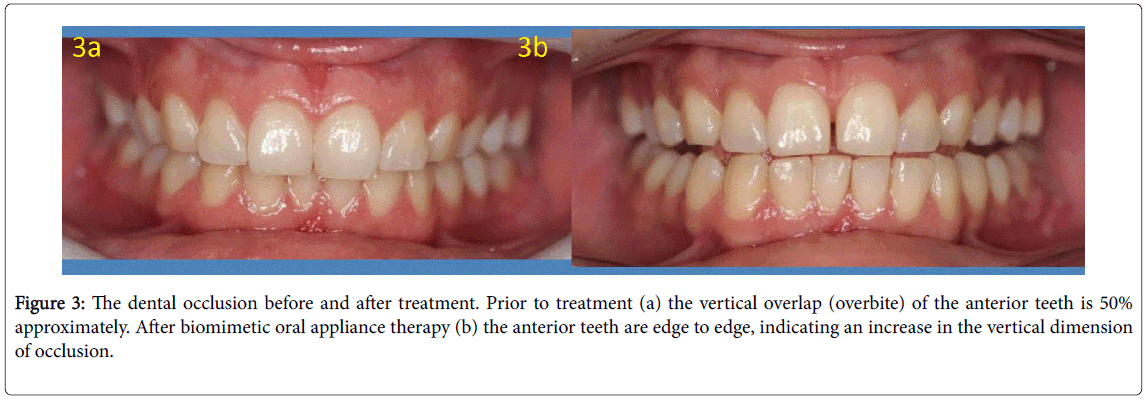
Figure 3: The dental occlusion before and after treatment. Prior to treatment (a) the vertical overlap (overbite) of the anterior teeth is 50% approximately. After biomimetic oral appliance therapy (b) the anterior teeth are edge to edge, indicating an increase in the vertical dimension of occlusion.
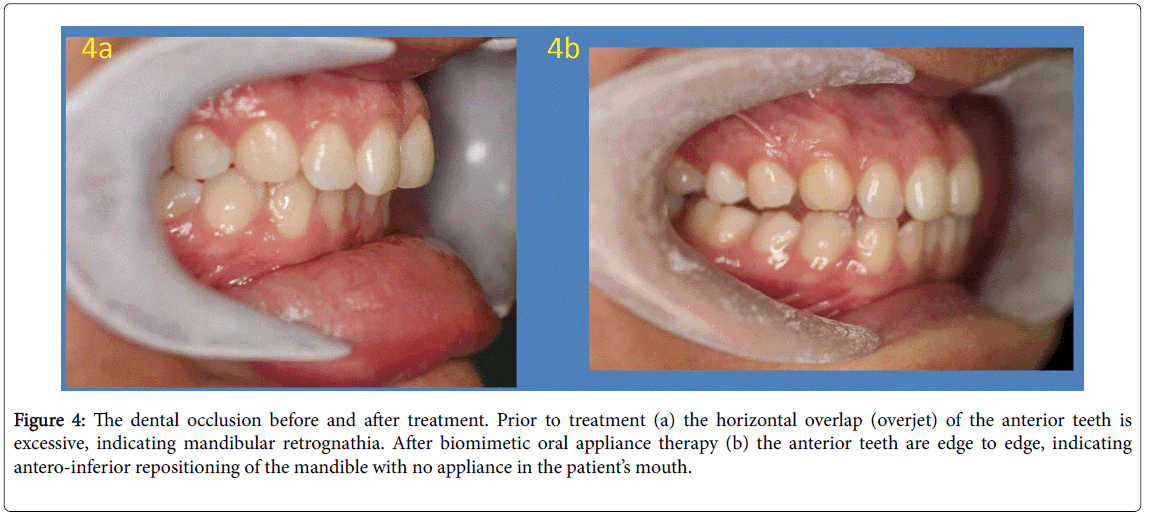
Figure 4: The dental occlusion before and after treatment. Prior to treatment (a) the horizontal overlap (overjet) of the anterior teeth is excessive, indicating mandibular retrognathia. After biomimetic oral appliance therapy (b) the anterior teeth are edge to edge, indicating antero-inferior repositioning of the mandible with no appliance in the patient’s mouth.
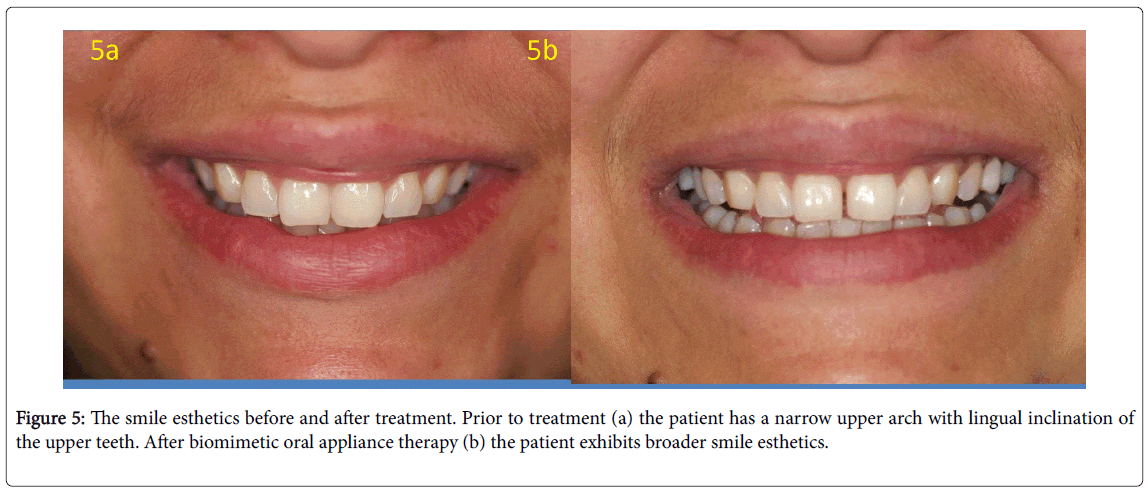
Figure 5: The smile esthetics before and after treatment. Prior to treatment (a) the patient has a narrow upper arch with lingual inclination of the upper teeth. After biomimetic oral appliance therapy (b) the patient exhibits broader smile esthetics.
Obstructive sleep apnea (OSA) is thought by some to be a disorder of craniofacial anatomy. In fact, the protocol described here has been used to treat mild, moderate and even cases of OSA [10-12]. Specifically, the device has been shown to increase midfacial bone and nasal cavity volume in adults [13-14]. In a study of adult patients with mild to moderate OSA, several subjects showed that the AHI dropped to < 5 hr-1 with no appliance in the mouth when the sleep study was performed [11]. Thus, the risks, benefits and alternatives were discussed in this case, including the fact that that oral appliances are typically not recommended for severe OSA unless the patient is refractory to CPAP [15]. Some craniofacial characteristics have been reported as being specific to upper airway resistance syndrome, which is included as a subgroup of OSA in the International Classification of Sleep Disorders [16]. For example, midfacial deficiency can be detected by noting crowding of the maxillary teeth and other dentofacial features, such as a narrow palate or mandibular retrognathia. If the root cause of OSA in a specific patient lies within the craniofacial anatomy, which houses the upper airway, then a potential cure for OSA may lie in that region, and the role of the general dentist becomes vital. When one considers the dynamics of air flow through the upper airway and the impact of Poiseuille’s law and the Bernoulli effect on the physiology of respiration [17], then restoring and maintaining normal craniofacial morphology may present a possible solution for OSA, as predicted by the spatial matrix hypothesis [18].
In this specific case, post-treatment assessment showed improvement of the oropharyngeal airway (Figure 1b), the external nares (Figure 2b) and the maxillo-mandibular relations (Figue 4b). Weight loss is considered an adjunctive therapy in reducing the severity of OSA [19]; however, this patient did not lose weight during the procedure. Although initially the patient felt some daytime sleepiness [20] and used her CPAP for comfort while sleeping at night, more recently, she reports she never uses the CPAP and wears the biomimetic oral device only 75% of nights while sleeping (approximately 8 h). All other craniofacial symptoms were resolved.
Despite these claims, the patient was advised to wear the biomimetic oral appliance every night during sleep, as there are no long term studies at this time that assess the stability of our initial findings. Nevertheless, home based sleep studies have correlated well to the laboratory based sleep studies for this particular patient, and she remains negative for OSA. Therefore, follow up for this case will be monitored using home sleep studies. Indeed, long term follow-up in collaborative clinical trials are now necessary to explore the important findings from this case study, as the costs of health care and impact on the quality of life of patients with OSA is significant. We conclude that this novel, combined protocol may represent a potential cure for OSA in some adults, but it is now necessary to replicate our findings in a larger, homogeneous study sample.
This study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All persons gave their informed consent prior to their inclusion in this study including additional informed consent from all individual participants for whom identifying information is included in this article.