Journal of Clinical Trials
Open Access
ISSN: 2167-0870
ISSN: 2167-0870
Research Article - (2015) Volume 5, Issue 3
Purpose: Safe and effective provision of pain management is one of an essential part and primary goal of initial emergency management of fractured femur in ED. This prospective study was performed to compare the analgesic effects of femoral nerve block (FNB) with parenteral morphine sulfate in patients with fractured femur.
Methods: 40 patients fractured femur were randomized into two groups. The FNB group received 15 ml lidocaine 2% under ultrasound-guided three-in-one, morphine group received 0.1 mg/kg IV morphine sulfate. VAS, were compared during foot dorsi-flexion 15, 30, 60 and 90 minutes later. Resident assistant were advised to prescribe morphine to target a 50% reduction in pain or per-patient request.
Results: There were significant pain relief in FNB according to pain scores (VAS) 15, 30, 60 and 90 minutes after FNB (P<0.001). There was no difference in adverse events between groups.
Conclusion: Ultrasound-guided femoral nerve block able to benefit over IV morphine sulfate for patient with femoral fracture in ED and can provide significant pain relief. Furthermore, standard pain management with parenteral opioids alone provided ineffective pain control in our study.
Keywords: Ultrasound-guided; Femoral nerve block; Lidocaine; Morphine sulfate; Fractured bone femur
Safe and effective provision of pain management is one of an essential part and primary goal of initial emergency management in ED. It can be challenging, especially with a major injury such as a femoral bone fracture. The initial care process involves transfers from stretcher to stretcher/imaging/operating-suite table or hospital bed within the first few hours, so prompt pain relief is essential [1]. Moving patient to get X-rays or transferring to a special bed to support the leg in traction (keeping the leg straight) can cause additional pain on the broken femur. Patient who experience greater pain is at higher risk for slower to mobilize, have longer hospital stays and poorer health-related quality of life. The ramifications of undertreated pain include increased risks for cardiovascular events, depression and sleep disturbances and decreased responses to interventions for other disease states [2,3]. At present, parenteral opioids are most commonly used for pain management. Opioid analgesics are often prescribed hesitantly because of fear of side effects. It has been seen that older adults in the ED are at risk for oligoanalgesia, often with other medical comorbidities, and the use of opioids in this population must be balanced with their potentially deleterious consequences [4,5].
Femoral fractures are usually high-energy injuries typically associated with severe pain. While these fractures do occur in isolation, the mechanism that result in the fracture frequently cause associated additional injuries including head, chest, and abdominal injuries. Risk of severe associated injuries accompanying femoral fracture, these patients typically undergo a formal trauma evaluation in the hospital emergency department, and the use of pain medications that depress the central nervous system must be limited to avoid masking important clinical clues to the underlying injury [6]. A femoral nerve block can provide effective pain relief and can be delivered safely in the emergency department with the appropriate equipment and education of the staff. This study was performed to compare the analgesic effects and pain control of femoral nerve block (FNB) versus intravenous (IV) morphine in patients with fractured femur [7-10]. The purpose of this study was to determine whether a femoral nerve block administered in the emergency department could provide better pain relief for patients with femoral fractures than currently used pain management practices with morphine sulfate [8,11,12].
The study was registered and approval was obtained to study enrollment. The hospital’s institutional and ethical committee approved the study protocol. This study was conducted at Central Hospital, a large, urban, academic emergency department with an annual census of over 100,000 adult visits per year. The hospital was a Level I trauma center. All patients signed their informed consent before participating in the study.
During times a resident co-investigator and trained research assistant were available under supervision by emergency medicine attend, research assistant identified eligible patients by surveillance of the ED. Each patient had an evaluation by the treating resident before recruitment for the study. Patients who were 5 to 80 years old presented to emergency department with femoral fracture were identified as potential candidates for this study. Patients meeting inclusion and exclusion criteria were approached for consent by a resident coinvestigator. Excluding criteria were head trauma and GCS<14, more than one isolated femur fracture, a known hypersensitivity or allergy to lidocaine or morphine, ongoing cardiac attack, renal failure disease, coagulopathy disorder, given more than 10 mg morphine prior to arrive to ED or any opioid addiction, infective lesion in FNB injection site, with local or systemic infection, opium-addicted patients or patients with an abnormal neurological exam in that limb [13-16]. A blinded, randomization occurred and performed by the department’s research coordinator who was not involved in enrollment or data collection. We did allocation of concealment, blinding of participants and personnel, blinding of outcome assessors. Clinical diagnosis confirmed by radiography after patient enrolment. All patients signed their informed consent before participating in the study.
Patients were identified, after orthopedic consult, the orthopedic resident on call determined whether the patient to neurovascular examination was eligible or not, to avoid any confounding effects produced by the nerve block on examination, as such patients may have a higher potential risk for associated thigh compartment syndrome which requires serial sensory exams that would be impeded by the FNB. Then, patients were randomized to one of two 20 patients (40 patients) groups: first arm (20 patients) femoral nerve block (FNB), second arm (20 patients) morphine sulfate alone. Along with the femoral nerve block, these patients received current standard-of-care management of the fracture pain, which consisted of extremity traction (a Hare traction splint applied either at the scene or in the emergency department) and an intravenous analgesia. The US-guided femoral nerve block was performed using a portable sonoAce R3 Medison (with a 7.5 MHz linear array transducer). The femoral nerve blocks were performed by trained and expert emergency medicine resident. All last year residents of emergency medicine in a position to enter patients into the study underwent 20 hours training session with an attending anesthesiologist on the practice of femoral nerve block to further augment their knowledge. The blockade procedure was performed under ultrasound guidance the femoral nerve block (4 cc/kg of lidocaine 2% without epinephrine) [17,18].
The procedure was performed while the participant was in a supine Trendelenburg position. The skin was prepped with povidone iodine solution. The US probe was placed 1 cm distal to the inguinal ligament on the side of the affected hip to identify the femoral vessels and nerve in cross-section. The nerve was isolated as a hyperechoic structure approximately 1cm lateral to the pulsatile artery and centered on the US screen for optimal viewing. A 27-gauge needle 2 cm lateral to the US probe puncture the skin at a 45° angle in plane to the US probe. The needle was directly visualized by US throughout the procedure to ensure that vascular puncture was avoided and that spread of local anesthetic was administered in the correct facial plane. After aspiration, lidocaine was injected along the nerve sheath through this. Immediately after the injection, manual pressure was held for 5 minutes 1 cm below the injection site [7,19,20]. In second group standard pain management alone titrate parenteral morphine sulfate (0.1 mg/kg in adults and 0.05 mg/kg in pediatrics) by pulse oximetery monitoring. Resident assistant were advised to repeat parenteral morphine sulfate prescribe to target a 50% reduction in pain or per-patient request every 30min in both groups.
Patients were asked to rate the pain and assessed in both group by research assistant who was not aware about patients analgesia method, with use of a visual analog scale, a 10-point visual analog scale, with 10 indicating the worst pain the patient had ever known and 0 indicating no pain at the fracture site, in rest at the initial (0 minute) evaluation and then at fifteen, thirty, sixty and ninety minutes following the initial evaluation in dorsi-flexion position. These measurements were chosen based on our prior experience that the largest decrease in patientreported VAS occurs [21,22].
Statistical Analysis
The sample size required for this study was estimated from our findings in two10 pilot patients. Our pilot study had demonstrated that patients given FNB had lower pain scores (μ1=3.3), by morphine lower pain score (μ2=2.8). Based on α=0.05, β=0.20, with an estimated standard deviation of FNB (S1=0.5) and morphine (S2=0.6), a sample size of 19.2 per group was required for one-tailed testing.
Data were analyzed by SPSS 18 software package. Parametric variables were described as mean ± SD; qualitative variables were described as number (percentage) and as median and range. Paired T-TEST was used as appropriate to compare the two groups. For all comparisons, a P-value<0.05 was considered indicative of a significant difference [23].
During 21 months period study from May 2013 to Feb 2015 about 1814 multiple-trauma patients visited in emergency department. From 114 patients with fractured femur, many patients were excluded for reasons given in the exclusion criteria: 44 patients with more than one isolated femoral bone fracture, 8 patients refused consent, 17 patients with head trauma and GCS<14, 2 patients with allergy to morphine, 2 patients with renal failure, and one patient with warfarin related coagulopathy, 74 patients were excluded for reasons given in the exclusion criteria. Only 40 patients were included in this study, 20 patients in each arm completed the study.
Demographics according to physical status, age (Table 1), weight (Table 2) and sex (Table 3) were not significantly different between the treatment groups.
| Statistics | |||||||
|---|---|---|---|---|---|---|---|
| sex.bolck | sex.morphin | weight.morphine | weight.block | age.morphine | age.block | ||
| N | Valid | 40 | 40 | 20 | 20 | 20 | 20 |
| Missing | 0 | 0 | 20 | 20 | 20 | 20 | |
| Mean | 65.00 | 67.60 | 39.50 | 40.45 | |||
| Mode | 56a | 78a | 23a | 21 | |||
| Std. Deviation | 10.443 | 16.028 | 18.662 | 20.702 | |||
| Minimum | 48 | 20 | 14 | 5 | |||
| Maximum | 85 | 90 | 71 | 80 | |||
Table 1: Age.
| Statistics | ||||
|---|---|---|---|---|
| sex | age | weight | ||
| N | Valid | 40 | 40 | 40 |
| Missing | 0 | 0 | 0 | |
| Mean | 39.98 | 66.30 | ||
| Std. Error of Mean | 3.077 | 2.121 | ||
| Median | 38.50 | 67.00 | ||
| Mode | 19a | 56a | ||
| Std. Deviation | 19.460 | 13.417 | ||
| Minimum | 5 | 20 | ||
| Maximum | 80 | 90 | ||
Table 2: Weight.
| Pain management | N | Mean | Std. Deviation | Std. Error Mean |
|---|---|---|---|---|
| AgeFNB | 20 | 40.45 | 20.702 | 4.629 |
| morphine | 20 | 39.50 | 18.662 | 4.173 |
| Pain management | N | Mean | Std. Deviation | Std. Error Mean |
| FNB | 20 | 67.60 | 16.028 | 3.584 |
| morphine | 20 | 65.00 | 10.443 | 2.335 |
| sex | Frequency | Percent | Valid Percent | CumulativePercent |
| female | 10 | 25.0 | 25.0 | 25.0 |
| male | 30 | 75.0 | 75.0 | 100.0 |
| Total | 40 | 100.0 | 100.0 |
Table 3: Sex.
Fracture types mostly involved the shaft (57.5%), then head and neck (17.5%), intertrochanteric (15%) and distal of femur (10%) respectively. The majority of patients in the FNB and morphine group had shaft of fractures in both male and female (Tables 4 and 5).
| Frequency | Percent | Valid Percent | Cumulative Percent | |
|---|---|---|---|---|
| Head and neck | 7 | 17.5 | 17.5 | 17.5 |
| Intertroc and prox | 6 | 15.0 | 15.0 | 32.5 |
| shaft | 23 | 57.5 | 57.5 | 90.0 |
| distal | 4 | 10.0 | 10.0 | 100.0 |
| Total | 40 | 100.0 | 100.0 |
Table 4: Fracture type.
| Count | |||||||
|---|---|---|---|---|---|---|---|
| Pain management | Fracture type | Total | |||||
| Head and neck | Intertroc and prox | shaft | distal | ||||
| FNB | sex | female | 2 | 1 | 3 | 1 | 7 |
| male | 1 | 3 | 8 | 1 | 13 | ||
| Total | 3 | 4 | 11 | 2 | 20 | ||
| morphine | sex | female | 0 | 1 | 2 | 0 | 3 |
| male | 4 | 1 | 10 | 2 | 17 | ||
| Total | 4 | 2 | 12 | 2 | 20 | ||
Table 5: Sex *fracture type *pain management.
Pain scores at initial of study was the same (mean=8.35, FNB. Std. Deviation=0.813, Morphine Std. Deviation=1.182) (Table 6).
| Pain management | Mean | N | Std. Deviation | |
|---|---|---|---|---|
| FNB | 8.35 | 20 | .813 | |
| Morphine | 8.35 | 20 | 1.182 | |
| Total | 8.35 | 40 | 1.001 | |
Table 6: VAS.0min.
Additional morphine requirement and satisfaction with patient position were significantly increased between the patients treatment alone with morphine. Pain score at 15, 30, 60, 90 minutes after intervention and parenteral morphine during dorsi-flexion were significantly different with 95% confidence interval between the FNB group and morphine group ( P-value<0.05 ) Sig. (2-tailed) (Tables 7 and 8).
| Pain management | N | Mean | Std. Deviation | Std. Error Mean | ||
|---|---|---|---|---|---|---|
| VAS.15min | dimension1 | FNB | 20 | 5.20 | 1.005 | .225 |
| Morphine | 20 | 6.70 | .979 | .219 | ||
| VAS.30min | dimension1 | FNB | 20 | 4.30 | 1.081 | .242 |
| Morphine | 20 | 6.55 | 1.146 | .256 | ||
| VAS.60min | dimension1 | FNB | 20 | 4.50 | 1.318 | .295 |
| Morphine | 20 | 7.20 | 1.196 | .268 | ||
| VAS.90min | dimension1 | FNB | 20 | 5.40 | 1.095 | .245 |
| Morphine | 20 | 7.70 | 1.031 | .231 | ||
Table 7: FNB group.
| Levene's Test for Equality of Variances | t-test for Equality of Means | |||||||
|---|---|---|---|---|---|---|---|---|
| F | Sig. | t | df | Sig. (2-tailed) | Mean Difference | Std. Error Difference | 95% Confidence Interval of the Difference | |
| Lower | Upper | |||||||
| VASmin15.068 | .796 | -4.781 | 38 | .000 | -1.500 | .314 | -2.135 | -.865 |
| -4.781 | 37.973 | .000 | -1.500 | .314 | -2.135 | -.865 | ||
| VASmin30.028 | .867 | -6.388 | 38 | .000 | -2.250 | .352 | -2.963 | -1.537 |
| -6.388 | 37.871 | .000 | -2.250 | .352 | -2.963 | -1.537 | ||
| VASmin60.007 | .933 | -6.784 | 38 | .000 | -2.700 | .398 | -3.506 | -1.894 |
| -6.784 | 37.651 | .000 | -2.700 | .398 | -3.506 | -1.894 | ||
| VASmin90.051 | .823 | -6.837 | 38 | .000 | -2.300 | .336 | -2.981 | -1.619 |
| -6.837 | 37.862 | .000 | -2.300 | .336 | -2.981 | -1.619 | ||
Table 8: Morphine group.
No adverse systemic toxicity of lidocaine, such as seizure, arrhythmia, or cardiovascular collapse was noted in the FNB group. Neither vascular puncture nor paresthesia occurred. No complications, such as hematoma, infection, injury or compartment syndrome, or persistent paresthesia were observed within 48 hours after the nerve block. No patient in either group had hypoventilation (respiratory rate 10/min) or oxygen saturation<95%. 2 patients in morphine group vomited, 3 of them were confused and one patient with hypersensevity to morphine. Figure 1 displays the mean scores on the visual analog scale reported at each time-point for both groups. The pain scores did not differ at baseline, for the patients treated with the block and those treated with morphine .Subsequently, the patients who received the block significantly lower pain scores at all time-intervals. At 15 minutes, the average pain score was 5.20 for the patients treated with the block and 6.70 for those treated with morphine; the difference (1.5; 95% confidence interval) was significant (p<0.001). 30, 60 and 90 minutes after the femoral nerve block, the patients continued to report significantly lower pain scores than those who had received the morphine (4.30, 4.50, 5.40 in block versus 6.55, 7.20, 7.70 in morphine respectively ; 95% confidence interval) was significant (p<0.001).
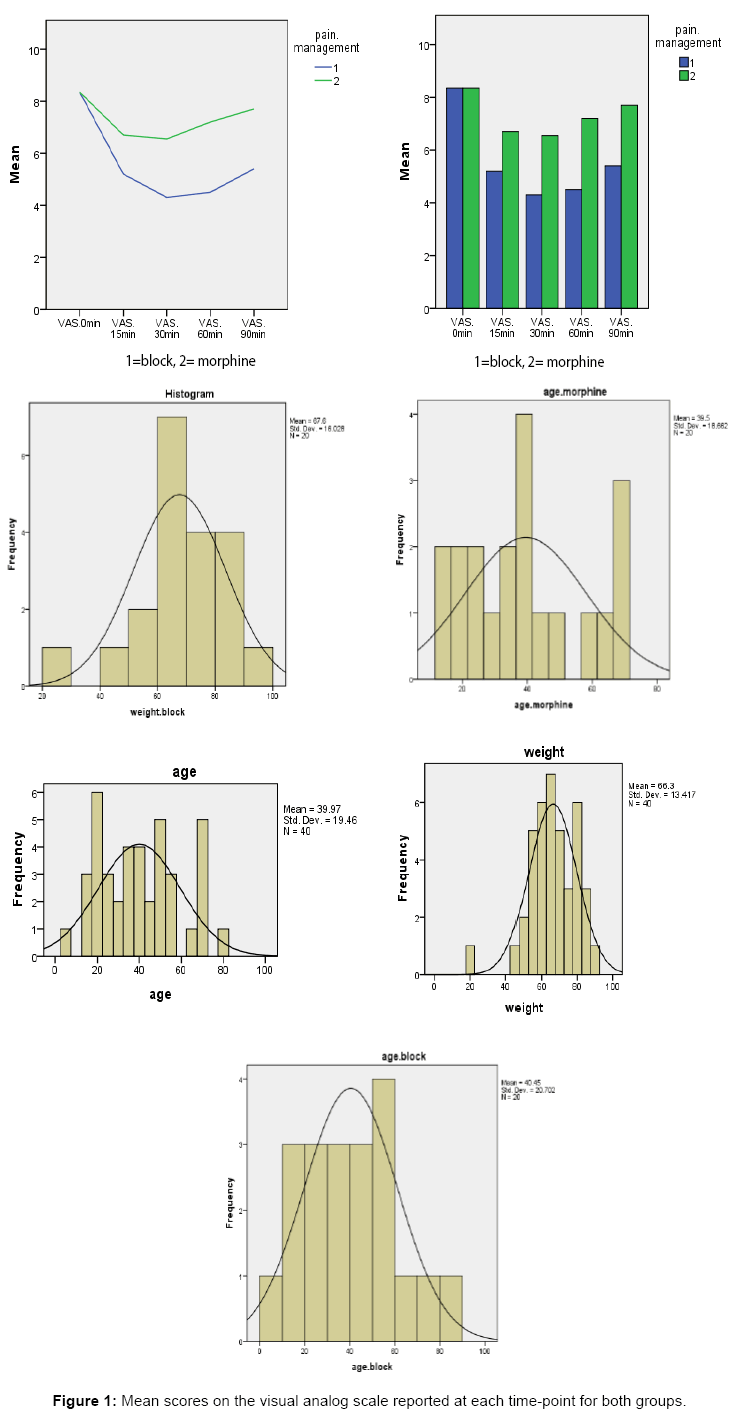
Figure 1: Mean scores on the visual analog scale reported at each time-point for both groups.
There was a significant decrease in pain intensity (decrease VAS) in the patients in the FNB group over time (p<0.001). The patients with fractured femur significantly lower pain scores with 95% confidence interval at 15, 30, 60, 90 minute in mid-shaft fracture in both arm (p=0.001, p=0.035, p=0.032, p=0.014 in block, p<0.01, p=0.010, p=0.010, p=0.003 in morphine). There is no significant difference between two groups in distal, intertrochanteric and proximal femur fracture.
At many Emergency Department, parenteral opioid was used more frequently than FNB for fractured femur and nerve blocks were used infrequently. There is a lack of sufficient randomized controlled trials investigating the efficacy and safety of nerve blocks compared with systemic analgesia. This prospective, randomized study shows that FNB can provide more pain relief than parenteral morphine in patients with fractured femur with 95% confidence interval. In both groups, initial pain scores at rest were the same (8.35 ± 0.813 in block, 8.35 ± 1.182 in morphine), whereas after 15, 30, 60 and 90 minutes, FNB analgesia during foot dorsi- flexion positioning were significantly different. Only one small trial of 40 patients was included in this study.
This trial did not study on pain levels during procedures or transfers, but mean duration of analgesia was significantly greater in the FNB group. Schiferer et aldemonstrated that FNB provided analgesia after femoral fracture which was adequate for patient transport [24] whereas Arissara Iamaroon et al. [25] could not to demonstrate a benefit of FNB over IV fentanyl for patient positioning in fractured femur. Other studies have described the successful use of FNB as analgesia in the emergency department [17,26]. Parker et al reported that nerve blocks reduced pain score and analgesic requirements [27]. However, few studies have investigated FNB to facilitate positioning during conduct of regional anesthesia. Gosavi et al., [16] assessed pain during change of position from supine to sitting after FNB with lidocaine; VAS scores were 2.7 ± 1.1.13 Sia4 et al compared IV fentanyl with FNB using lidocaine. VAS values during placement in the sitting position were lower in the FNB group (0.5 ± 0.5 versus 3.3 ± 1.4 for FNB and IV fentanyl, respectively). Mosaffa et al. [24] compared IV fentanyl with fascia iliaca block using lidocaine. VAS values during placement in the lateral decubitus position were lower in the fascia iliaca block group [0.5 (0–1) versus 4 (2–6) for fascia iliaca block and IV fentanyl, respectively]. Haddad et al. [28] also demonstrated that the analgesic benefit of FNB in extra-capsular femoral neck fractures occurred at 15 minutes. The quality of the analgesia depends on the fracture site; excellent relief can be obtained for mid-shaft fractures, good relief for lower third fractures, and partial relief for upper third fractures [29]. In our study, the fracture sites were mostly at the mid-shaft. This study designed included patients with 4 type of femoral fracture with different types of fracture site were analyzed separately rather than being grouped together. To clarify the results further, a comparison of change in pain scores may have been useful, but we did not record baseline pain scores in this study at initial time. We believe that pain scores on foot dorsi-flexion of a fractured femur at baseline should ideally be. However, for ethical reasons, we decided not to measure baseline pain scores on movement and consider that baseline pain scores at rest would not be comparable with pain scores during foot dorsi-flexion.
We were able to demonstrate difference in an analgesic benefit between FNB and IV morphine in fractured femur patients. Further studies are required before definite conclusions can be reached. However, use of FNB can provide pain relief for patients with fractured femur. With regard to opioids, potential side effects must be considered and analgesic dosing should be titrated based on pain scores. It is important to highlight the training implications of any widespread recommendation for FNB, especially if guided by ultrasound. The use of ultrasound guidance with these techniques needs to be studied further to determine whether it improves outcomes. Regional nerve blockade, while widely trained, is not a core skill in all Emergency Medicine curricula. Point-of-care ultrasound is now included in most emergency medicine curricula; however, ultrasound-guided nerve blockade is considered to be an advanced or extended skill, making its widespread implementation more challenging, and suggesting that specific extracurricular training may be required. Since the imprecision of the results also lowers the quality of the evidence, we downgraded a further evidence level on that basis, so overall we judged the evidence to be of low quality, which means that further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.