Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2013) Volume 1, Issue 4
Hyperthyroidism is associated with altered endothelial dysfunction and increased risk of arterial thromboembolism and cardiovascular disease. Von Willebrand factor (vWF) is a marker of endothelial dysfunction. There is controversy in reports that have been published concerning the concentrations of vWF in hyperthyroidism. The aim of this study was to investigate the plasma vWF levels in clinical hyperthyroid patients, as well as its relationship to thyroid hormones fT3, fT4 and TSH compared to control subjects. In this study forty recently diagnosed, non-treated clinical hyperthyroid patients (f=37, m=3) and twenty normal volunteers control (f=18, m=2) were included, and subjected to determination of plasma vWF by ELISA technique and serum fT3, fT4 and TSH by Elecsys cobas e 601 analyzer. The data was statistically analysed by SPSS-10 and p values less than 0.05 were considered significant. Our results showed that there were a significant increase of vWF, fT4 and fT3 levels by 100%, 285% and 100%, respectively, and a significant decrease of TSH levels by 12.9-folds in hyperthyroid patients than in control group. For vWF (mean ± SD, 252.2 ± 66.4 vs 126.4 ± 29.9%, repectively; p=0.001). vWF was significantly positively correlated with fT4 and negatively correlated with TSH. In conclusion, we confirmed that hyperthyroidism was associated with increased vWF levels, a novel marker of endothelial dysfunction, FT4 levels being a predictive of vWF levels. Endothelial dysfunction could contribute to higher risk for thromboembolic and cardiovascular disease.
Keywords: Hyperthyroidism; Endothelial dysfunction; vWF; Thromboembolism; Thyroxine; Triiodothyronine; Thyroid stimulating hormone
Hyperthyroidism is associated with altered endothelial dysfunction [1], and increased risk of arterial thromboembolism [2], and cardiovascular manifestations [3,4], such as tachycardia, systolic hypertension, heart failure and increased probability of cardiovascular mortality. Clinical studies suggested that endothelial dysfunction was the possible cause of such cardiovascular manifestations [5]. Endothelial dysfunction represents an early stage of atherosclerosis, and can be regarded as a predictor of cardiovascular events [6]. Endothelial dysfunction is characterized by a reduction in the bioavailability of vasodilators, particularly nitric oxide (NO), leading to impairment of endothelium-dependent vasodilation, or by an increase in endothelium-derived contracting factors [7]. Endothelial dysfunction is prominent in atherosclerosis [8], but also has been described in diabetes, preeclampsia, hypertension, uremia and other diseases [9]. In a broader sense, endothelial dysfunction encompasses proinflammatory and procoagulant changes, as well as apoptotic cell death [10]. Von Willebrand factor (vWF) is a large multimeric glycoprotein that plays an important role in primary haemostasis by promoting platelet adhesion, by forming a bridge between platelet glycoprotein and exposed collagen in the subendothelium at sites of vascular injury [11]. It also acts as plasma carrier for factor VIII, protecting it from premature destruction or rapid proteolysis. vWF is synthesised exclusively in endothelial cells and megakaryocytes, and stored in Weibel-Palade bodies and platelet a-granules, respectively. Most of plasma vWf is derived from endothelial cells rather than from platelets under normal circumstances [12]. vWF is a marker of endothelial dysfunction. Numerous clinical and experimental reports suggest that a high vWf level reflects endothelial damage or endothelial dysfunction [13-15]. There is controversy concerning the concentrations of vWF in hyperthyroidism, increased or decreased vWF levels have been reported in several papers [2,16,17]. In the present study, we evaluated the plasma vWF levels in clinical hyperthyroid patients, as well as its relationship to thyroid hormones, fT3, fT4 and TSH compared to control subjects.
Subjects
This study was conducted in Sana’a, Yemen, from April to May, 2013. It included 60 subjects aged 23 to 61 years. The patient’s group consisted of 40 recently diagnosed, non-treated hyperthyroid patients (37 females and 3 males) (mean age ± SD, 39.6 8.7; median, 38.5; ranged from 28 to 61; 95% CI, 36.8-42.4 years old). These patients were selected randomly each day from subjects referred to the out-patient’s, and inpatient’s clinics of medical and general surgery departments (n=7) of Kuwait University Hospital (KUH), and from subjects referred to the specialized medical laboratories, Aulaqi (n=12), Med-Lab.(n=11) and Al-Dubhani (n=10), for ELISA thyroid hormones measurements, the diagnosis of clinical hyperthyroidism was based on increased levels of serum fT4 and/or fT3, and decreased TSH levels. The control group included 20 subjects (18 females and 2 males) (mean age ± SD, 30.4 ± 5.9; median, 28.5; ranged from 23-43; 95% CI, 27.6-33.1 years old), as normal non-hyperthyroid volunteers from the workers and students of KUH. All participants gave their informed consent to participate in this study.
Sample collection
Five millimetres (5 ml) of venous blood were withdrawn under complete aseptic condition from each of patient and control group. From this 5 ml, 3 ml were put in plain tube and 2 ml in sodium citrated tube. Citrated samples were mixed well and separated by centrifugation within 20 minutes of collection at 3500×g for 5 minutes. The separated plasma was stored frozen at -70°C for later analysis and estimation of vWF concentrations. Sample of plain tube was left to clot for 30 minutes and serum was separated by centrifugation at 3500×g for 5 minutes. Determination of serum fT3, fT4 and TSH concentrations were carried out immediately and the remaining serum samples were stored at -70°C.
Biochemical methods
Determination of Free Triiodothyronine (FT3): Serum fT3 concentration was measured using the electrochemiluminescence immunoassay (ECLIA) technique, intended for use on the Elecsys fT3 reagent kit supplied by Roche Diagnostics GmbH (Mannheim, Germany), and run on cobas e 601 immunoassay analyzer from Roche Diagnostics Ltd, Switzerland. The intermediate precision CV of the method was 2.5% for a mean value 2.70 pg/mL. The Elecsys fT3 assay employed a competitive principle between fT3 in a test specimen and specific anti-T3 antibody labelled with a ruthenium complex. The reference range for serum fT3 was 2.0-4.4 pg/mL [18].
Determination of Free Thyroxine (FT4): Serum fT4 concentration was measured using the electrochemiluminescence immunoassay (ECLIA) technique, intended for use on the Elecsys fT4 reagent kit supplied by Roche Diagnostics GmbH (Mannheim, Germany), and run on cobas e 601 immunoassay analyzer from Roche Diagnostics Ltd, Switzerland. The total precision CV of the method was 2.6% for a mean value 1.31 ng/dL and the analytical sensitivity of the assay was 0.023 ng/ dL. The Elecsys fT4 assay employed a competitive principle between fT4 in a test specimen and specific anti-T4 antibody labelled with a ruthenium complex. The reference range for serum fT4 was 0.93-1.7 ng/dL [18].
Determination of Thyrotropin (TSH): Serum TSH concentration was measured using the electrochemiluminesce-immunoassay (ECLIA) technique intended for use on the Elecsys TSH reagent kit supplied by Roche Diagnostics GmbH (Mannheim, Germany), and run on cobas e 601 immunoassay analyzer from Roche Diagnostics Ltd, Switzerland. The intermediate precision CV of the method was 3.2% for a mean value 0.092 mIU/ml, and the functional sensitivity of the assay was 0.014 mIU/mL. The Elecsys TSH assay employed a sandwich principle between TSH in a test specimen and specific monoclonal antibodies labelled with a ruthenium complex. The reference range for serum TSH was 0.27-4.20 mIU/mL [19].
Determination of von Willebrand factor (vWF): Plasma vWF concentrations were measured using AssayMax vWF ELISA kit supplied by Assaypro Llc. (Missouri, USA), and run on Multiscan EX from Labsystem, Finland. The intraassay and interassay coefficients of variation were 4.9% and 7.6%, respectively. The average recovery was 100%. The minimum detectable level was less than 1 IU/ml (%). The assay employed a quantitative sandwich enzyme immunoassay technique by which a murine antibody specific for vWF has been precoated onto a microplate. Human vWF in standards and samples was sandwiched by the immobilized monoclonal antibody and biotinylated polyclonal antibody specific for vWF. The reference values of the assay were 60-200% [20].
Statistical analyses
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS software version 10.0 for Windows, Inc., Chicago, Illions, USA), to indicate the degree of significant between the mean values of the patient groups and the mean values of the corresponding controls. Descriptive data were given as mean ± standard deviation (SD). All tests were two-tailed and p values less than 0.05 were considered statistically significant. Pearson correlation coefficients (r) were calculated to quantify the relationship between vWF and other variables.
von Willebrand factor vWF
There was a significant increase mean vWF levels in hyperthyroid patients than in control group by 100% (Mean ± SD, 252.2 ± 66.4%; median, 260.5%; confidence interval (CI), 231.0-273.4% vs 126.4 ± 29.9%; median, 126.5%; 95% CI, 112.5-140.4%, respectively; p=0.001) (Table 1). In hyperthyroid patients, vWF was ranged from 1.10 to 3.42 compared to control 65 to 175 %. Thirty two of forty (80%) hyperthyroid patients had plasma vWF levels >200 %, the upper limit of the assay. Table 2 showed that vWF in hyperthyroid patients was significantly positively correlated with fT4 levels (p=0.013) and negatively correlated with TSH (r= -0.383; p=0.015), and no significant correlations with fT3 and age (Figure 1 and 2). In control group, non-significant correlations were observed between vWF and other variables.
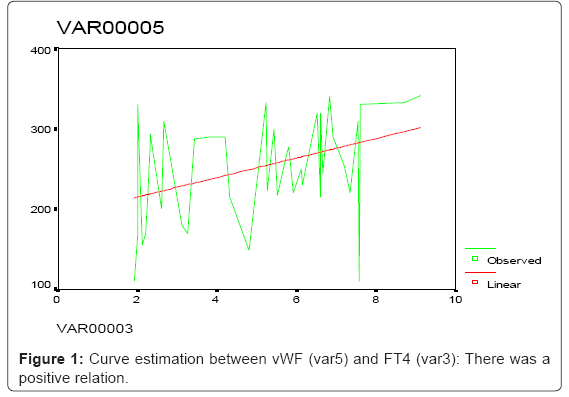
Figure 1: Curve estimation between vWF (var5) and FT4 (var3): There was a positive relation.
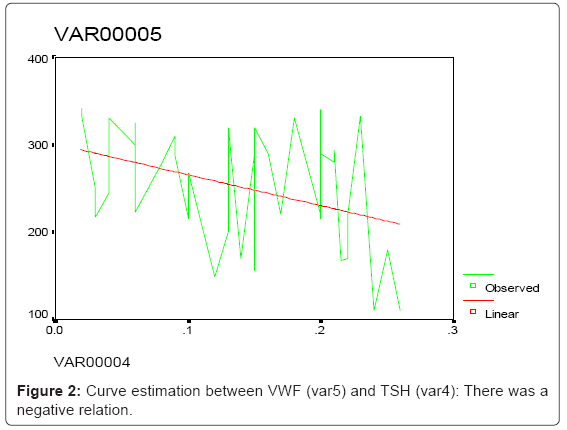
Figure 2: Curve estimation between VWF (var5) and TSH (var4): There was a negative relation.
| Groups | Hyperthyroid | Control | |
| patients (n=40) | Subjects (n=20) | P value | |
| Variables | (Mean ± SD) | (Mean ± SD) | |
| von Willebrand factor (vWF) (IU/ml) | 252.2 ± 66.4 | 126.4 ± 29.9 | 0.001 |
| Free triiodothyronine (FT3) (pg/ml) | 5.80 ± 1.94 | 2.90 ±0.55 | 0.001 |
| Free thyroxine (FT4) (ng/dL) | 5.05 ± 2.12 | 1.31± 0.15 | 0.001 |
| Thyroid-stimulating hormone (TSH) | 0.14 ± 0.07 | 1.95 ± 0.74 | 0.001 |
| (mlU/L) | |||
Table 1: Comparison between levels of vWF, FT3, FT4 and TSH in hyperthyroid patients and control subjects.
| Variable | Hyperthyroidism (n=40) | ||
| r | P† | ||
| TSH | -0.383 | 0.015 | |
| FT4 | 0.388 | 0.013 | |
| FT3 | 0.219 | 0.174 | |
| Age (Year) | -0.030 | 0.853 | |
Table 2: Correlations between plasma vWF and other variables in hyperthyroid patients.
Thyroid hormones parameters
Serum TSH levels in all (100%) hyperthyroid patients were significantly lower than the control group by 12.9-folds (Mean ± SD, 0.14 ± 0.07; median, 0.14; ranged from 0.02 to 0.26 mIU/ml vs 1.95 ± 0.74, median, 1.90; ranged from 0.80 to 3.50 mIU/ml, respectively; p=0.001) (Table 1). Serum TSH level was significantly negatively correlated with both vWF (r=-0.383; p=0.015) and fT4 (r=-0.492; p=0.001), and non-significantly correlated with fT3 and age.
On the other hand, both fT4 and fT3 were observed to be significantly higher in the hyperthyroid patients by 285% and 100%, respectively, compared to the control group (Table 1). For fT4, the mean ± SD was 5.05 ± 2.12; median was 5.46; ranged from 1.90 to 9.10 ng/dl vs 1.31 0.15, median, 1.35; ranged from 1.00 to 1.50 ng/dl, respectively; p=0.001). Serum fT4 level was significantly positively correlated with vWF (r=0.388; p=0.013) and negatively correlated with TSH (r=-0.492; p=0.001), and non-significantly correlated with other variables. For fT3, the mean ± SD was 5.80 ± 1.94; median was 6.00; ranged from 2.10 to 10.60 pg/ml vs 2.90 ± 0.55, median, 2.80; ranged from 2.00 to 4.00 pg/ml, respectively; p=0.001). Serum fT3 level was non-significantly correlated with other variables. All hyperthyroid patients (100%) had fT4 levels >1.7 ng/dl, the upper limit of assay, whereas 28 of 40 (70%) had fT3 levels>4.4 pg/ml, the upper limit of assay.
In the present study, elevated plasma vWF was found to be associated with hyperthyroidism. vWF was elevated in 80% of hyperthyroid patients This observation of elevated plasma vWF was consistent with the results of other previous studies [1,16,21,22], but was not in agreement with other author [2], they demonstrated unchanged vWF values between hyperthyroidism and control group. In our study, plasma levels of vWF were significantly higher by 100% when compared with control subjects (p<0.001), and there were a direct significant relationship between vWF and fT4, and a significant, but inverse relationship between plasma vWF and TSH levels, with non-significant relations with fT3 and age. Therefore, fT4 levels being a predictive of vWF levels. Similar observation was found by other previous study [23]. They demonstrated a significant positive correlation between vWF with T4 and T3. In the opposite side, our observation of correlations was not in agreement with other study [21]. They reported that vWF did not correlate with fT3, fT4 and TSH.
In our study, increased vWF levels in hyperthyroid patients may reflect endothelial dysfunction that represent an early stage of atherosclerosis, and can be regarded as a predictor of cardiovascular events [6]. There are numerous clinical and experimental reports confirm that a high vWf level reflects endothelial damage or endothelial dysfunction [13,14]. Endothelial dysfunction, which is indicative of a proinflammatory and procoagulant state, may explain the association between hyperthyroidism and thromboembolism [10,22]. The increased vWF antigen (vWF:Ag) levels were associated with increased platelet plug formation in hyperthyroidism [17], which is mediated through beta-adrenergic receptors [24], and this may also explain the association between hyperthyroidism and thromboembolism. Taken together, these changes may contribute to a higher cardiovascular risk in hyperthyroid patients. Therefore, hyperthyroidism was associated with elevated plasma vWF levels that represent a novel marker of endothelial dysfunction, which may contribute to a higher risk for thromboembolic potential and cardiovascular diseases in these hyperthyroid patients.
In conclusion, we confirmed that overt hyperthyroidism was associated with increased vWF levels, a marker of endothelial dysfunction; FT4 levels being a predictive of vWF levels. Endothelial dysfunction could contribute to higher risk for thromboembolic and cardiovascular disease. We recommended the evaluation of plasma concentration of vWF in overt hyperthyroidism as a marker for endothelial dysfunction.
We would like to thank doctors of Lab., technician and the health workers in KUH and specialized medical laboratories, Al-Aulaqi, Med-Lab. and Al-Dubhani, for their help and cooperation.