Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 1
Study objectives: To assess the validity and reliability of the Persian translated version of the Occupational Impact of Sleep Questionnaire (OISQ).
Design: This observational and case-control study performed in two stages along with about one to two-month period.
Setting: We used the Persian version of the Pittsburg Sleep Questionnaire Index (PSQI-P) as a valid and reliable scientific tool to differentiate cases and controls.
Participants: From 150 people - all had official works - eventually, 121 persons (81 female and 40 male) were eligible for participation.
Measurements and Results: The α-Cronbach’s validity coefficient of translated OISQ was 0.786 at the level of 1% (p<0.001). The α-Cronbach’s correlation coefficients for reliability were 0.972 and 0.976 in stage one and two, respectively. It was found that scoring ≤12 and ≥20 from OISQ-P were compatible with good sleeper and poor sleeper, respectively.
Conclusion: The Persian version of the OISQ was a valid and reliable questionnaire. It also could differentiate good and poor sleepers.
Keywords: OISQ-P; PSQI-P; Reliability; Screening tool; Sleep; Validity
Sleep and its effects on daytime activity, level of intelligence, health, body fitness and life quality have demonstrated strong straight and bidirectional relations [1]. According to these wide interrelations, quality and quantity of doing works in different jobs are not exclusive. Inadequate sleep and/or undiagnosed sleep disturbances in, specifically, working population could lead to occur unintentional work accidents and even death [1]. Although, having normal sleep has specific definition for each person, but there are common and clear definitions of signs and symptoms contributing to diagnose different disorders. In large communities with prominent working population is very important to have effective workers and advanced economy. Achieving these goals needs fast, easy, advantageous, accurate and scientific approach to screen target population, continuously. Screening methods always were beneficial approaches to distinguish healthy from the sufferer. Occupational Impact of Sleep Questionnaire (OISQ) is one of most popular self-rating questionnaires, evaluating the impact of sleep on diurnal working function. We planned to assess validity and reliability of a Persian translated version of this questionnaire.
The study was done as an observational and case control in fall, 2013. Primary sample size involving 150 people, 52 (34.7%) men and 98 (65.3%) women, all with official works in different units under supervision of the University of Medical Sciences. All samples were chosen by simple random selecting method. We did our study in two stages along with a period of time between 30 and 60 days. We made two similar files containing three attached questionnaires, including Pittsburg’s Sleep Questionnaire Index (PSQI), Occupational Impact of Sleep Questionnaire (OISQ) and Mini Sleep Questionnaire (MSQ), all in Persian, for each stage and each participant. During first stage, we described goals and two-time process of fully filling triple questionnaires in each stage. Fortunately, all selected accepted to take part in study. We took a verbal consent from each one and promised to save data privacy. We gave a number to each participant in order to compare two stages results, personally. After finishing second stage 121 persons were eligible based on meeting all criteria, including having daily works, not to do nocturnal or shift works, no supervising child and/or old, no pregnancy for women and answering all questions in both stages.
Persian version of Pittsburg’s sleep questionnaire index (PSQI-P)
The eighteen questions in a self-rating questionnaire with Likert answering system, first time translated into Persian by Moghaddam et al in March, 2012. The α-Cronbach’s coefficient for reliability measured 0.77 among all 258 participants of that study [2]. They also reported sensitivity and specificity of their questionnaire in differentiating cases, and controls were 94% and 72% respectively [2]. Consequently, they proved their work had enough reliability to distinguish some sleep disorders such as primary insomnia, major depression and daytime over sleepiness. The PSQI-P contains seven sections designing based on international classification of sleep disorders to find involved people in at least last four weeks [2,3]. These sections categorized as subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, daytime dysfunction and hypnotic medication use. Each part of these categories could score from zero to 3 points; as a result, a fully filled PSQI-P score rated from zero to 21 [2,3]. Classification of these seven sections into three major factors also performed. Factor 1 which also named as sleep efficiency included sleep duration and sleep efficiency. Factor 2 (perceived sleep quality) included sleep latency, subjective sleep quality and hypnotic medication use. Factor 3 that also stated as daily disturbances included sleep disturbances and daytime dysfunction [2,3]. Scoring ≥ 5 in PSQI-P considered as low sleep quality or being a poor sleeper and scoring < 5 considered as being a good sleeper or having good sleep quality [2]. We applied PSQI-P as a reliable scientific tool in order to differentiate cases, and controls. Similarly, David and Morgan used this method to evaluate Dutch version of OISQ in 2008 [4]. The PSQI has been translated in many languages, including Spanish, Chinese, Hebrew, French, German and Japanese [3].
Occupational impact of sleep questionnaire (OISQ)
The English version of OISQ designed by David and Morgan firstly in 2005 and late was translated to Dutch version in 2008 by primary designers [4]. It was a self-rating 24 questions questionnaire, basically evaluating impacts of sleep on daytime working quality during last four weeks. Each question had 5 different qualitative answering items based on Likert answering system. The items included Never/Not applicable (0), a little bit of the time (1), Some of the time (2), Most of the time (3) and All of the time (4). Thus, each fully filled questionnaire scores between zero and 96. The higher scores imply on higher probability of inadequate working dysfunction due to poor sleep quality and/or quantity [4]. In order to choose more true words transferring more accurate concept, we have a sequential process to translate the source English questionnaire into target language, Persian. Initially, three copies of source questionnaire forwarded to three medical students in different levels of graduation -whom spoke Persian as their mother tongue language- for making primary translations. Then all three translated questionnaires were given to another medical student in order to synthetize the best primary questionnaire by choosing proper translated words for each line. After that, this preferred questionnaire posted to two different English language experts to translate it back into English, without mailing the source one. They made the work blindly. Eventually, we achieved to a general consensus on the final translated questionnaire after a meeting with three medical specialists and two English language experts. The α-Cronbach’s coefficient for reliability in Dutch version reported 0.93 and cut points to differentiate good and poor sleeper were ≤ 10 and ≥ 20 respectively.
Data analysis
This study had eventually 121 eligible daytime office workers, who all were compatible with including criteria. We used the 18 version of Statistical Program of Social Sciences (SPSS). Mean and standard deviation was computed for each variable. To analyze α-Cronbach’s coefficient for reliability and Guttman Split-half coefficient for internal consistency was done. We measured repeatability by performing Test re-test exam. Using this exam help us to check consistency of repeating OISQ-P since it was expected to not to change over time. As this questionnaire needs at least four weeks interval to evaluate repeatability, we considered a period of 30-60 days interval between refilling the questionnaires. On the other hand, Test re-test exam is able to show method defects, as the data of test and re-test have wide difference, it shows something else except every considered one is missed. Although, it is a proven psychological examination formula tests stable traits too. While sleep disorders in shift or night workers are stable problem, using Test re-test method help to be reassured of participants responds and not to have something missed or incompatible. Inter-item correlation measurement was done for validity value by examining OISQ and PSQI answers. We used ANOVA exam to define cut points of translated OISQ. We considered level of significant p less than 0.05. We also calculated equation of continuity of OISQ-P response rate and found the R-square for this equation.
This study performed completely in two predicted stages. While from all 150 primary participants (98 women and 52 men), eventually 121 persons within 20 to 68 years of age with mean (±SD) age of 31.7 ± 9.5 matched with all inclusion criteria, mentioned above. Totally, 81 (67%) women by 20-62 years of age with mean (±SD) age of 29.7 ± 7.87 and 40 (33%) men by 24-68 years of age with mean (±SD) age of 35.8 ± 11.31 were eligible to take part in the study. Men were older than women (p<0.001, %95CI: 2.60-9.60). Twenty nine (19.4%) of all removed due to incomplete answering (10, 6.7%), leaving study (7, 4.4%), pregnancy or supervising children (4, 2.7%) and others (2, 1.3%). According to analysis, we found no difference in time of getting slept (p=0.08), interval between going to bed until getting slept (p=0.97), time of awakening in the morning (p=0.69) and nocturnal sleep duration (p=0.49) between two genders. Thus, there was no significant subjective difference in quantitative parameters of nocturnal sleep between men and women. Probability values and some score findings reported in Table 1. According to findings, there were four significant correlations. First, it showed direct relation between OISQ-P score and gender (p=0.029) with Pearson’s correlation coefficient 0.173, implying on women experience the little impact of inadequate sleep quality on their working function. Second, there was a positive direct correlation between Factor 1 (sleep efficiency) and age (p=0.03) with Pearson’s correlation coefficient 0.171 which meant older people influenced more from sleep disturbances. Third, we found strong correlation between Factor 3 (daily disturbances) and gender (p=0.008) with Pearson’s correlation coefficient 0.231, implying on males were at risk of daily disturbances due to their sleep disorders. Fourth, there was a negative correlation coefficient (-0.208) between Factor 3 and age, that meant older people had the lesser sense of daily disturbances. Reliability analysis was performed by measuring α-Cronbach’s coefficient. It showed a great internal consistency in our translated version of OISQ-P. It measured 0.972 and 0.976 in stage one and two respectively. We calculated this value for PSQI-P as 0.789 and 0.805 in initial and additional stages, respectively. However, analysis of the Guttman Split-half coefficient as 0.906 in first stage and 0.925 in second one, again implied on reliability of our translated questionnaire OISQ-P. We found validity value of OISQ-P as 0.847 (p<0.001) and 0.786 (p<0.001), at the significant level of 1%, in primary and secondary stage, respectively.
| Variables | Stage one | Stage two |
|---|---|---|
| PSQI-P* score rate | 1-16 | 1-16 |
| OISQ-P** score rate | 0-90 | 0-92 |
| PSQI-P score mean (±SD) | 7.13 ± 3.46 | 6.74 ± 3.27 |
| OISQ-P score mean (±SD) | 52.21 ± 22.84 | 54.79 ± 23.69 |
| PSQI-P score and age | P=0.313 | P=0.274 |
| OISQ-P score and age | P=0.185 | P=0.134 |
| PSQI-P score and gender | P=0.130 | P=0.290 |
| OISQ-P score and gender | P=0.125 | P=0.029 |
| Factor 1 and age | P=0.283 | P=0.030 |
| Factor 1 and gender | P=0.434 | P=0.450 |
| Factor 2 and age | P=0.473 | P=0.400 |
| Factor 2 and gender | P=0.339 | P=0.292 |
| Factor 3 and age | P=0.011 | P=0.128 |
| Factor 3 and gender | P=0.008 | P=0.187 |
Table 1: Probability values and some score findings. (*Persian version of Pittsburg’s Sleep Questionnaire Index, **Persian version of Occupational Impact of Sleep Questionnaire).
Cut Points of OISQ-P
In order to find real cut points for translated questionnaire, we measured a mean of OISQ-P, MSQ-P and PISQ-P based on the latter subjective sleep quality answers. Table 2 shows measurement. According to our findings, founded good sleepers, who had proper sleep quality, scored ≤12.7 and ≤12.63, whether poor sleepers scored ≥19.38 and ≥18.75 from OISQ-P in first and second stage, respectively. Figures 1 and 2 show graphs of this finding.
| Stage one | Stage two | |||||||
|---|---|---|---|---|---|---|---|---|
| MSQ-P* | PSQI-P** | MSQ-P | PSQI-P | |||||
| mean | %95CI | mean | %95CI | mean | %95CI | Mean | %95CI | |
| Good sleepers | 21.47 | 19.28-23.65 | 3.93 | 3.55-4.31 | 21.33 | 19.24-23.43 | 3.92 | 3.55-4.28 |
| Poor sleepers | 29.74 | 27.89-31.57 | 9.03 | 8.36-9.69 | 28.9 | 27.05-30.76 | 8.59 | 7.93-9.25 |
| ANOVA | F=32.06 , P<0.000 | F=123.44 , P<0.000 | F=28.213 , P<0.000 | F=115.5 , P<0.000 | ||||
Table 2: Measurement of OISQ-P cut points. (*Persian version of Mini Sleep Questionnaire, **Persian version of Pittsburg’s Sleep Questionnaire Index).
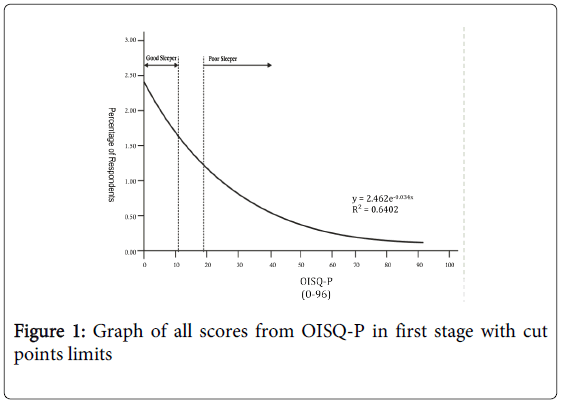
Figure 1: Graph of all scores from OISQ-P in first stage with cut points limits
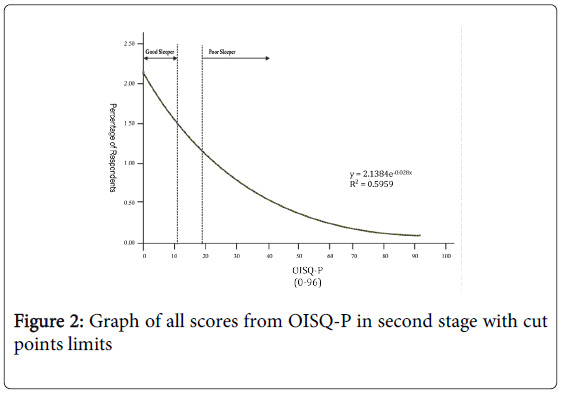
Figure 2: Graph of all scores from OISQ-P in second stage with cut points limits
Sleep disorders had extensive multi aspects side effects in both human and animal [5-8]. Negative impacts from simple but bothering symptoms such as bruxism and increasing appetite up to life threatening one such as cardiovascular disease, coronary artery calcification, respiratory dysfunction, immune system dysfunction and even death due to road and work accidents, all heightened morbidity and mortality in at least in last two decades which complain of low sleep quality increased up to 33% among 20-59 years-old population in the united states [5-7,9]. Unfortunately, such complications would fail performance cycles for family and whole society by making disasters, passive working population, handicaps and other irreversible miserable outcomes. In this study, we tried to prepare a fast, easy and scientific screening tool in order to find how sleep influences on worker functions and who is a good or a poor sleeper. Data analysis showed strong values for reliability and validity of our translated Persian version of OISQ, fortunately. This prepared tool for all who speak or understand Persian is now available also to detect whose sleep is good or not. It is possible by counting a fully filled OISQ-P score. Anybody who scores ≥ 20 consider as a poor sleeper that means his or her sleeping quality worsened his or her working function and who scores ≤12 consider as a good sleeper with good working function in last four weeks. Although, based on our study, older people daily functions influenced more negatively than younger because of sleep deficiency, but they suffered lesser from daily disturbance, which is compatible with another study [10]. The latter maybe due to its natural history of chronically event, getting consistent with gradually occurring daily disturbances lowers sense of bothering by that kind of disturbances and eventually would make it easier to ignore, in high probability. The fact that older people impact more from sleep efficiency maybe due to aging, other synchronous systemic diseases and/or drug complications–which did not include in our study as variables- affecting natural physiology of sleep. We found women experience daily disturbances much more than men; however, it doesn’t impact on their working functions, subjectively. It may be due to kind of easier jobs they should do, which perform by lower stress and responsibility or their higher self-assurance level. Unfortunately, data showed a vicious cycle between using hypnotic medications and poor sleep quality subjectively. As sleep-influencing medications lead to imbalance in the normal sleep cycles, it would make real sleep disorder in somebody who was not involved before. It seems very important to attend because of increased prevalence of self-ordered sleep medications and complaints of lower sleep quality in last years, based on reports of other study [5,11].
The process of translation from to any other language always would have some mistakes, as every language influenced deeply by bases and changes of history, culture and art. Therefore, we never claim our Persian translation transfers all concepts of its English version. Although, we had a previous model for performing the study,4 though OISQ is unable to detect all factors of PSQI except of sleep efficiency and especially sleep impacts on quality of daily working functions. Another limitation of study was absent from variables evaluating other factors, which could affect sleep characteristics as other basic systemic disorders.
This study was an adoption of the medical student’s thesis who was the corresponding author for this study, too. This study was done under supervision of the department of psychiatry in the University of Medical Sciences, Qom, Iran.