Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 5
Objective: Nocturnal bruxism, the repetitive grinding, clenching, and chewing movements of the jaw during sleep, can occur in both children and adults. Case series and anecdotal reports suggest that botulinum toxin type A injection may provide effective treatment of nocturnal bruxism and its sequelae. Open-label trials for patients with nocturnal bruxism indicate that it may confer reduction in pain medication use and migraine headache frequency. This study is an open label, pilot study to establish 'proof of principle' for the use of Onabotulinum toxin A (BOTOX, Allergan) to treat nocturnal bruxism with associated craniofacial pain.
Methods: Five consenting subjects with nocturnal bruxism and craniofacial pain who have tried dental prosthetics, and have failed trials of at least two prophylactic headache medications were enrolled. Four completed the trial. No serious adverse events were experienced by any subject. The primary outcome measure of this study was the change in number of EMG bursts in the temporalis and masseter muscles as measured during nocturnal polysomnography in an accredited sleep laboratory. Polysomnograms were administered once for baseline measurement and at weeks 4, and 8 after injection of 100-150 U of Onabotulinum Toxin A (BOTOX, Allergan) in a fixed site pattern including temporalis and masseter muscles.
Results: Average number of bruxism events decreased through Week 4 after treatment. One of four participants' polysomnograph showed consistent decrease inbruxism events in the weeks following treatment but overall the trends did not reach statistical significance. Secondary outcome measures which demonstrated a trend for improvement included bed partner survey of bruxing activity and sleep interruption, and daily subject craniofacial pain diary. MIDAS scores showed statistical improvement at week 4 after injection. Sleep efficiency and percent rapid eye movement (REM) sleep on polysomnograms demonstrated a trend towards improvement after injection but did not reach statistical significance.
Keywords: Nocturnal bruxism; Sleep bruxism; Migraine; Facial pain; Botulinum toxin; Polysomnography; Oromandibular dystonia; Sleep efficiency; Headache; Parasomnia
Case series and anecdotal reports suggest that onabotulinum toxin type A (BOTOX, Allergan) injection may provide effective treatment of nocturnal bruxism and its sequelae. Open-label and placebo controlled trials for patients with nocturnal bruxism indicate that it may reduce bruxing frequency, [1] pain medication use and migraine headache frequency [2].
Bruxism is associated with headaches and migraine [3,4]. Onabotulinum toxin type A has been shown to be safe and effective in the treatment of headache syndromes such as migraine [5,6] and chronic cervical-associated headache [7,8].
Onabotulinum toxin type A (BTX A) has been used to treat a variety of movement disorders including segmental dystonias and oromandibular dystonias, spasticity, muscle spasm, cervical sprain, TMJ syndromes, and bruxism related to a variety of acquired and congenital conditions [9]. Onabotulinum toxin type A is currently FDA approved in the United States for use in intractable migraine, chronic daily headache, and segmental dystonia such as cervical dystonia, but remains “off label” in the treatment of Bruxism.
This pilot study is a “proof of principle trial” using polysomnography to explore the potential of onabotulinum toxin type A in the treatment of sleep related bruxism and associated craniofacial pain and headache.
Bruxism, the repetitive grinding, clenching, and chewing movements of the jaw, can occur as a “parafunctional” (uncommon activity of a specific body part, in this case the jaw) nocturnal behavior in normal children and adults, or as diurnal behavior in those with oromandibular dystonia [10], developmental disorders [11], and traumatic brain injury [12]. Some have postulated a pathophysiological relationship to cranial-cervical dystonia [13,14]. Sleep bruxism can be associated with craniofacial pain, headache, symptoms of temporomandibular joint dysfunction (TMJ), tooth wear, and cosmetically unsightly masseter hypertrophy [15-18].
This is an open label uncontrolled pilot trial. The protocol was approved by the Western Institutional Review Board. Enrollment in the trial occurred after written informed consent performed by a board certified neurologist. Onabotulinum toxin injections were performed by a board certified neurologist.
Participants
The five study participants ranged from 47 to 72 years of age. Four of the five patients (80%) were female. Participation required: completed minimal criteria for Sleep Bruxism questionnaire and had associated craniofacial pain, score greater than 5 on the Numerical Rating Scale of Pain (NRS), previous trials of dental prosthetics, and prior failed trials of at least two prophylactic headache medications, and stable pharmacological treatment of craniofacial pain, headache and bruxism for one month prior to injection.
Study design
Subjects were enrolled, and prophylactic medications held constant during the first four, pre-treatment, weeks. The primary outcome measure was the change in number of tonic and phasic EMG bursts/hour in the temporalis and masseter muscles as measured during nocturnal polysomnography in an accredited sleep laboratory at baseline pre-injection, and at 4, and 8 weeks after onabotulinum toxin type A injection.
Study interpretations were performed by a neurologist board certified in both neurology and sleep medicine. Participant enrollment and Injections were performed by the principle investigator, a board certified neurologist. The Secondary outcome measures include: daily craniofacial pain diary and daily bed partner self-reports of bruxing activity and sleep interruption, Headache Impact Test (HIT-6), Migraine Disability Assessment Scores (MIDAS), Beck Depression Inventory (BDI-II) at baseline, immediately prior to injection, and four, eight and twelve weeks after injection, and recorded use of prescription pharmaceuticals for prophylaxis and aborting headache, emergency department and urgent care visits.
Treatment procedure
Participants received 100-150 units of onabotulinum toxin type A (10 U/0.1mL, preservative-free, normal saline). Injections were given on day zero (immediately following the 30 day screening period). A fixed-site, bilateral, headache injection paradigm was expanded to include muscles of mastication and was used in the following muscles:
Masseter (bilateral, 10 units each)
Temporalis Superior (bilateral, 10 units each)
Temporalis Inferior (bilateral, 10 units each)
Levator Scapulae (bilateral, 0-20 units each)
Splenius capitus (bilateral, 0- 20 units each)
Frontalis (bilateral, 5 units each)
Procerus muscle (5 units)
Glabellar (bilateral, 2.5-5 units each
Statistical methods
Two-tailed student T-test analyses were performed to compare pre- and post-intervention data. For specific outcomes in which multiple pre-treatment data points were available for each participant (i.e. in which daily assessments were obtained in the 30 days prior to treatment), two-tailed T-tests were performed using the individual’s pre-intervention data as baseline for comparison with post-intervention outcomes.
Five subjects (N=5) were involved in the study. Data points for certain outcome measures were not available, because a participant was lost to follow-up or because the participant or his or her bed partner did not self-administer a qualitative assessment.
Of the five subjects enrolled, four were available for assessment of primary outcome after injection. Two participants did not complete self-assessments for secondary outcome measures; bed-partners of three participants provided incomplete reports of audible bruxing and sleep disruption.
Primary outcome measure
The average number of EMG bursts/hour in the temporalis and masseter muscles demonstrated a decreasing trend at Week 4 post injection (mean of 34 events/night to mean 30.4 events). The changes were not statistically significant (p>0.05, n=5) (Figure 1).
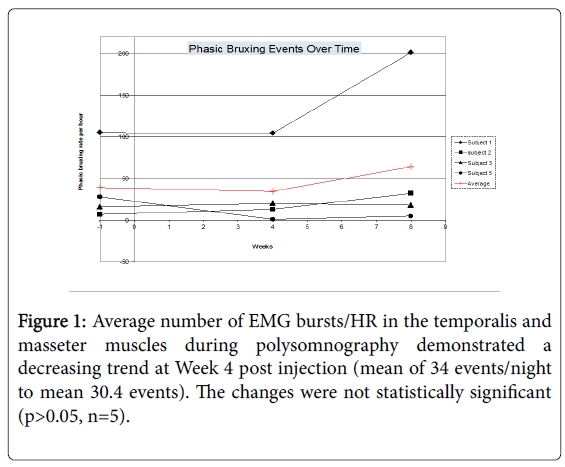
Figure 1: Average number of EMG bursts/HR in the temporalis and masseter muscles during polysomnography demonstrated a decreasing trend at Week 4 post injection (mean of 34 events/night to mean 30.4 events). The changes were not statistically significant (p>0.05, n=5).
Secondary outcome measures
Craniofacial pain: Subjects recorded craniofacial pain using a daily diary of 0 (no pain) to 3 (most severe pain). On average, craniofacial pain decreased during the first eight weeks following injection, from a mean rating of 2.25 to 1.5 over the course of eight weeks, though the change was not shown to be statistical significant (n=4, p>0.05) (Figure 2).
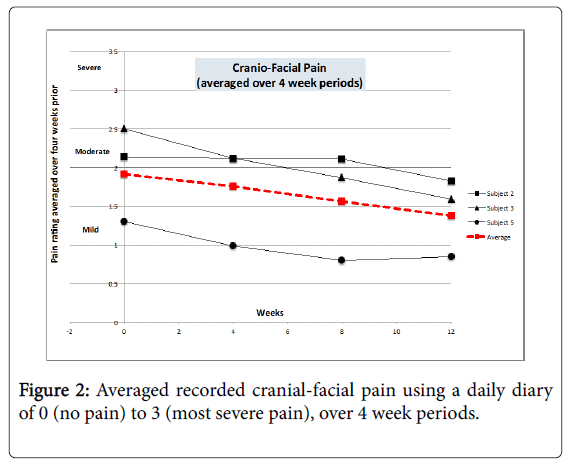
Figure 2: Averaged recorded cranial-facial pain using a daily diary of 0 (no pain) to 3 (most severe pain), over 4 week periods.
Jaw movements and sleep interruptions: Bed partners kept a daily self-reported diary of audible bruxing, and sleep interruption during the study. Per bed partner reports, four of the participants had detectable bruxism events six to seven times per night. Two partners completed the diaries. Both noted audible bruxing, and both noted a decline in these events prior to and after injection.
The average of both reported number of jaw movements and sleep interruptions decreased over the course of eight weeks following treatment. Average jaw movements decreased from 0.83 on Day 0 (averaged over the 30 days prior to treatment) to 0.69 at Week 8 (averaged over the 30 days prior to and including the first day of Week 8). While both subjects showed a decrease in this measure, the average change was not statistically significant (n=2, p>0.05).
Both subjects also experienced a decline in sleep interruptions. The average decreased from 1.7 interruptions per night to 1.3. For subject number 1, the decrease in interruptions between treatment and Week 4 was found to be statistically significant (p=0.035); for subject number 2, the decline in interruptions between Week 4 and Week 8 was found to be statistically significant (p=0.015) (Figure 3).
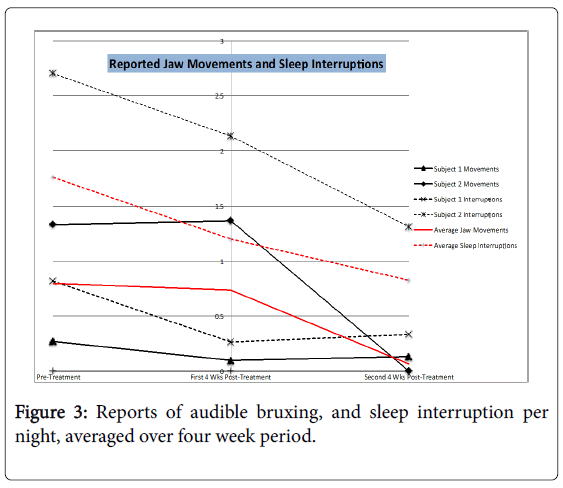
Figure 3: Reports of audible bruxing, and sleep interruption per night, averaged over four week period.
Percent rapid eye movement (REM) sleep increased from an average of 14.2% to 16.6% in the four weeks following treatment, approaching 20%, the expected percent REM sleep in the general population. The change in the participant population, however, did not reach statistical significance (n=4, p>0.05).
Average sleep efficiency increased from 0.76 to 0.81 during the first four weeks after treatment, remaining stable at 0.81 over the next four weeks (Figure 4). The change is not statistically significant but indicates a trend that warrants further study.
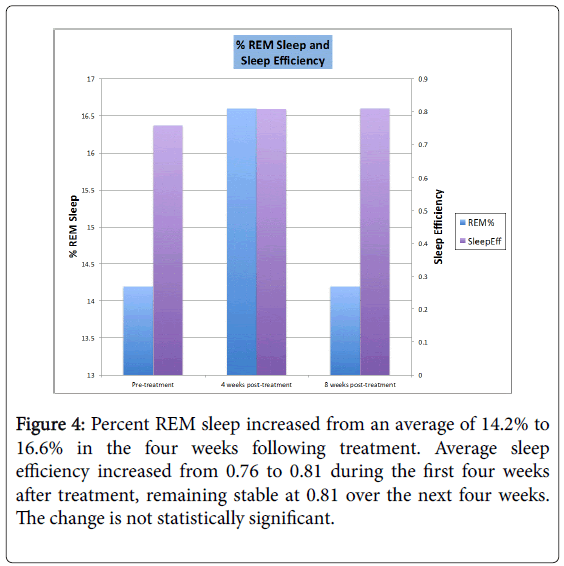
Figure 4: Percent REM sleep increased from an average of 14.2% to 16.6% in the four weeks following treatment. Average sleep efficiency increased from 0.76 to 0.81 during the first four weeks after treatment, remaining stable at 0.81 over the next four weeks. The change is not statistically significant.
These changes may indicate a possible treatment effect, or may be related to first-night effect in the sleep laboratory.
Headaches and migraine: HIT-6 scores quantify the disability subjects experienced as the result of headaches. Scores were taken at four-week intervals beginning during the pre-treatment phase. Four subjects self-administered the Headache Impact Test (HIT-6) immediately prior to treatment and at four-week intervals thereafter. The average HIT-6 score fell after treatment, dropping to 53 points by Week 8; these findings did not reach statistical significance (n=4, p>0.05 for each four week interval) (Figure 5).
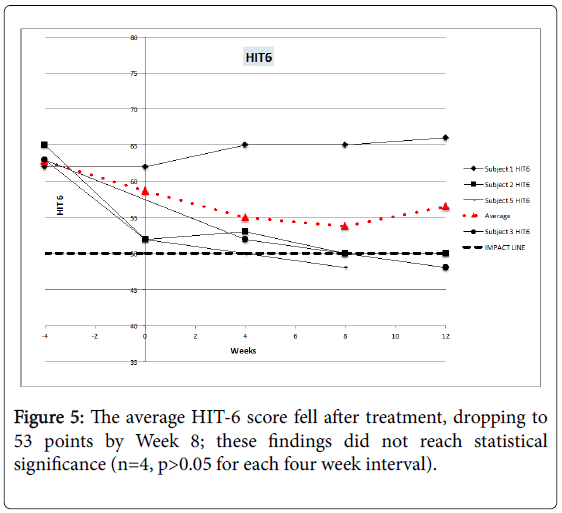
Figure 5: The average HIT-6 score fell after treatment, dropping to 53 points by Week 8; these findings did not reach statistical significance (n=4, p>0.05 for each four week interval).
Migraine Disability Assessment Scores range from 0 (no headache-related disability) to 21 and beyond (severe headache-related disability) were obtained for four subjects prior to and following injection at 4 week intervals. While there was notable variability among participants, the average score was 37.5 at Day 0 (prior to treatment) and dropped below 21 to 15.75 by the fourth week. This finding is statistically significant (n=4, p<0.036). Scores remain below 20 for the remainder of the study (n=4, p>0.05) (Figure 6).
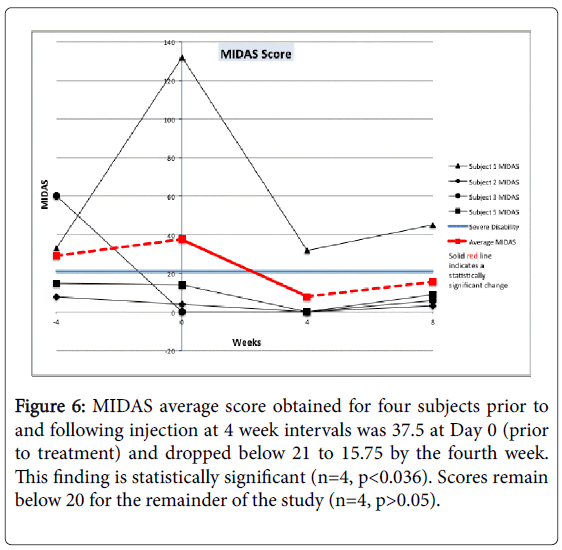
Figure 6: MIDAS average score obtained for four subjects prior to and following injection at 4 week intervals was 37.5 at Day 0 (prior to treatment) and dropped below 21 to 15.75 by the fourth week. This finding is statistically significant (n=4, p<0.036). Scores remain below 20 for the remainder of the study (n=4, p>0.05).
While use of headache prophylaxis did not change following treatment, medications used to abort headaches showed a decline shortly after treatment, followed by a return to pre-treatment levels.
Other secondary outcome measures
The Beck’s Depression Inventory II (BDI-II) BID-II scores were obtained during the screening period, on Day 0 (pre-treatment), and subsequent four-week intervals. Average participant scores decreased through the study, though starting and remaining within the “minimal depression” range (0-13). None of the participants were seen at an urgent care facility during the course of the study.
Adverse events
One participant was diagnosed with thyroiditis not attributable to the intervention.
Another participant experienced injection site pain that did not persist or have sequelae
Nocturnal or sleep related bruxism, has been considered a parasomnia, and was re-classified as a sleep related movement disorder in 2005 [19]. It can occur in both children and adults [20]. The frequency and duration of bruxism is highly variable night to night, week to week, even year to year [21] potentially limiting the usefulness of intermittent polysomnography to explore a treatment effect on the motor behavior itself. This study’s findings are consistent with others that have failed to show a statistically significant treatment response in EMG burst frequency or duration in Masseter and Temporalis recordings four weeks after injection [22]. The use of a portable EMG device has suggested a significant reduction in motor bruxing events after botulinum toxin injections [1] but evaluation of secondary sequelae were limited. Bruxism affects 3-35% of the adult population and 85-90% of the general population report experiencing bruxism in the course of their life time [1,4]. Prevalence estimates vary in part because sufferers are often unaware of the parasomnia [23], confounding diagnosis of associated morbidity [16] such as headache, sleep disruption and craniofacial pain [3]. The etiology of sleep bruxism remains obscure, but is likely centrally mediated [1,20]. This uncontrolled pilot study enrolled subjects who continued to experience chronic daily craniofacial pain despite the use of night guards and prophylactic treatments. This study was limited by small sample size, uncontrolled design, possible sampling error, “first night effect” in the sleep laboratory, and dosage limitations. Despite limitations, the trends indicate a possible treatment effect in bruxing behavior, craniofacial pain, migraine and associated sleep disruptions in subjects who have failed therapy with dental prosthetics, and headache prophylactic medications. Onabotulinum toxin A has shown efficacy for treatment of intractable migraine [6,24] and oromandibular dystonia [25]. As a pilot “proof of principle24” trial, the findings support the need for larger, placebo controlled trials investigating the use of onabotulinum toxin type A in the treatment of nocturnal bruxism and it’s sequelae. The impact of treatment on sleep disruption and sleep architecture should be further explored.
This uncontrolled pilot trial demonstrated statistical improvement in pain and headache outcome variables and a trend for, but no statistically significant reduction in, polysomnographic EMG bursts in temporalis and masseter muscles after Onabotulinum Toxin A injection in subjects with sleep bruxism who have failed conventional therapy. Larger, placebo controlled trials are indicated.
This study was funded by an unrestricted research grant from Allergan, Inc. Thanks are due to Ryan Irvine, Ph.D. for assistance with protocol development, Ina Roy-Faderman Ph.D. for assistance with writing, statistical analysis and graphics, Tiffany Olsen CMA for study coordination, Gerald Rich MD and the Pacific Sleep Center for montage development and sleep study interpretations, and Mathew Brodsky MD and the Pacific Northwest Basal Ganglia Coterie for critical review.