Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2016) Volume 6, Issue 4
Acute pancreatitis (AP) is an inflammatory disorder of the pancreas. Majority of cases will recover without complications, but the remainder will have severe disease. It is the most common gastrointestinal disorder that requires hospitalisation. Gallstones and alcohol are the leading culprits. Stratifying severity using the revised Atlanta Classification is of paramount importance. Important aspects of management include fluid resuscitation in the first 24 hours and adequate opiate analgesia. Endoscopic retrograde cholangio pancreatography (ERCP) should be performed within 24 hours in patients with biliary pancreatitis and concurrent cholangitis. Cholecystectomy should be performed in the index admission in cases of mild biliary pancreatitis. Complications of severe pancreatitis should be managed in a multidisciplinary centre with expertise in management of the more complex aspects of the condition including pseudocysts and walled off pancreatic necrosis. This article will explore the aetiology, diagnosis and current advances in the treatment of acute pancreatitis.
<Keywords: Acute pancreatitis, Pancreatic necrosis, Causes of pancreatitis, Pancreatitis treatment
Acute pancreatitis (AP) is an inflammatory disorder of the pancreas. Majority of cases (up to 80%) will recover without complications, but the remainder will have severe disease [1] and require a multidisciplinary approach to their care, ideally in specialist high volume centres. Overall mortality of acute pancreatitis is 5% [2], with severe pancreatitis having a considerably higher mortality rate which has not reduced over the last decades despite advances in understanding of the disease.
This article will explore the aetiology, diagnosis and current advances in the treatment of acute pancreatitis.
Aetiology
The incidence of pancreatitis is increasing [3] but up to 15% will have no cause of their pancreatitis identified.
The two main causes for pancreatitis are gallstones (38%) and alcohol (36%) but the risk of biliary pancreatitis is unlikely to be more than 2% in patients with asymptomatic gallstones [4] and alcoholic pancreatitis does not develop in more than 3% of heavy drinkers [5]. Biliary disease as the cause of pancreatitis is more common in women, with alcohol the precipitant more often in men [6-8].
There are other less common causes of acute pancreatitis. Hypertriglyceridemia can precipitate attacks of acute pancreatitis when serum concentrations are above 1000 mg/Dl (11 mmol/L). It accounts for about 1-4% of causes of acute pancreatitis [9]. Hypercalcemia can also cause acute pancreatitis through accumulation of secretory proteins, secretory block and possibly activation of proteases.
Autoimmune pancreatitis can sometimes present as acute pancreatitis (particularly in type II), although the usual presentation is one of weight loss, jaundice, and pancreatic enlargement on imaging, mimicking a neoplasm.
A pancreatic tumor should be considered as a possible cause of acute pancreatitis in patients over 40 years old. In a recent study, in patients after an episode of acute pancreatitis, 1.5% were eventually diagnosed with cancer compared to 0.13% without a prior episode. In addition, 12 % of patients with pancreatic cancer had an episode of acute pancreatitis prior to the diagnosis of their cancer. As pancreatic cancer is almost always diagnosed in advanced stages, patients over the age of 40 with acute pancreatitis should be evaluated for a pancreatic malignancy [10]. There are recognised genetic mutations and abnormalities that have an association with acute pancreatitis. Mutations of the cystic fibrosis trans membrane conductance regulator (CFTR) have been associated with an autosomal recessively inherited pancreatitis. Mutations (gain of function) in the serine protease 1 gene (PRSS1) on chromosome 7q35 results in an autosomal dominantly inherited form of hereditary pancreatitis. Recurrent acute pancreatitis can occur in cases of pancreas divisum (failure of the ventral and dorsal pancreatic duct to fuse). While pancreas divisum can be seen in up to 7% of patients in autopsy series, only a small percentage of these cases will go on to develop AP.
There are a wide variety of drug classes that have been known to cause pancreatitis. The mechanism of their effect varies. Immune mediated toxicity is thought to be the cause in amino salicylates and sulfonamides, direct toxicity with diuretics and accumulation of toxic metabolites with valproate and pentamidine. Common drugs that have been associated with pancreatitis include azathioprine, erythromycin, simvastatin, itraconazole, lamivudine, olanzapine and sulfasalazine. Infectious agents including viruses (mumps, cocksackie, Hepatitis B, HIV) and bacteria (mycoplasma, legionella, shigella) or parasites (Ascaris) can cause pancreatitis but their frequency is unclear. How often these viruses are responsible for idiopathic acute pancreatitis is unclear [11].
AP occurs in approximately 5% of patients undergoing therapeutic endoscopic retrograde cholangiopancreatography (ERCP) and up to 25% undergoing sphincter of Oddi manometric studies followed by ERCP. The increased incidence in the latter group is not due to manometry itself but by the subgroup of patients with suspected sphincter of Oddi dysfunction in which manometry and ERCP is performed [12]. Risk factors for those who are at increased risk of ERCP related pancreatitis include being female, of young age, Sphincter of Oddi dysfunction, a small common bile duct and technique. Minimal injection of contrast into the pancreatic duct (PD) and insertion of a prophylactic PD stent have reduced the rates of pancreatitis by two thirds. A single rectal dose of Indomethacin at the time of the ERCP has been shown to reduce incidence and severity of post ERCP pancreatitis [13].
Multiple studies have suggested that cigarette smoking is an independent risk factor for acute and chronic pancreatitis for mechanisms which are unclear [14].
Pathogenesis
Pancreatic duct obstruction leads to upstream blockage of pancreatic secretions, impeding exocytosis of zymogen granules from acinar cells [15]. Consequently, the zymogen granules coalesce with intracellular lyososomes to form autophagic vacuoles containing an admixture of digestive and lysosomal enzymes [15]. There is an accumulation of active trypsin within vacuoles activating a cascade of digestive enzymes leading to an autodigestive injury [15].
Acinar injury due to this autodigestive process stimulates an inflammatory response within the parenchyma of the pancreas. Acute pancreatitis arises when intracellular mechanisms to prevent trypsinogen activation or to reduce trypsin activity are overwhelmed.
Once trypsinogen is activated into trypsin within acinar cells, many pathways are activated including the complement and kinin systems. Local production of mediators including interlukin 1, interlukin 6 and interlukin 8 from neutrophils, macrophages and lymphocytes occur as well as the production of tumour necrosis factor alpha from macrophages [16,17].
Ultimately, the severity of pancreatic damage is related to injury of acinar cells and to activation of inflammatory and endothelial cells [6]. Thus, the mechanism of complications can be understood – local complications of acinar cell necrosis, psuedocyst formation and injury to remote (extra pancreatic) organs through inflammatory mediators often accompanied by a systemic inflammatory response syndrome (SIRS).
Diagnosis
AP is diagnosed if 2 of the 3 criteria are fulfilled. These are 1) typical abdominal pain: an acute onset of severe epigastric pain often radiating through to the back 2) an elevated serum lipase (or amylase) at least three times the upper limit of normal or 3) characteristic findings of acute pancreatitis on contrast enhanced CT (CECT) or MRI or transabdominal ultrasonography.
Pancreatic enzyme activity (lipase or amylase) concentrations while are one of the criteria used to diagnose acute pancreatitis are not a marker of disease severity or a monitoring tool [18]. Serum lipase remains elevated for a longer period of time as compared with amylase, which is useful in delayed presentations. The sensitivity of amylase in the diagnosis of acute pancreatitis is 67 to 83%. The main pitfall of amylase is its poor specificity in comparison to lipase which has a sensitivity and specificity from 82 to 100% [19].
Initial biochemical assessment on admission include a full blood count, electrolytes, urea, creatinine, liver function tests, blood sugar, coagulation profile and total albumin.
An alanine aminotransferase (ALT)>150 IU/L is highly suggestive of a biliary cause. A meta-analysis found that an elevated serum alanine aminotransferase (ALT) concentration was the most clinically useful parameter in predicting a gallstone aetiology in patients with acute pancreatitis [20] with a positive predictive value of 95%. The aspartate aminotransferase (AST) concentration was nearly as useful as ALT, while the total bilirubin and alkaline phosphatase concentrations did not assist in making the diagnosis [20].
A chest x-ray on admission may show pleural effusions, pulmonary infiltrates or oedema, a marker of severe disease. An abdominal x-ray maybe performed which reveals a localised ileus in severe disease.
Transabdominal ultrasound should be performed on admission to exclude gallstones. The size of offending stones are up to 5 mm; gallstones with a diameter of 8 mm or more often remain in the gallbladder [21]. Alternative imaging modalities to detect CBD stones include MRCP and EUS and help avoid the inappropriate use of a diagnostic ERCP. Endoscopic ultrasonography is the best single test to assess for common bile duct stones [22,23] and should be employed if there is a strong clinical suspicion but it’s use is dependent upon availability making MRCP and EUS equally useful in a real world setting.
A CT scan on admission solely for severity assessment is not warranted as clinical scoring systems are as reliable as radiological scoring systems [24] and an early CT scan should therefore be considered when the initial ultrasound is non-diagnostic or there is doubt about the diagnosis [25]. Performing a CT scan too early will often misguide the clinician to under-estimate the severity of presentation as necrosis occurs later in the course. A multi-detector CT scan using a pancreatic protocol (thin slices 5 mm or less ) and intravenous contrast performed 3-5 days after diagnosis is useful to assess for local complications including collections in patients with severe disease and in those with evidence organ failure.
Assessing severity
The Modified 2012 Atlanta Classification is the standard classification for severity of pancreatitis, using a three staged classification. Severity is stratified into mild, moderate and severe. Mild pancreatitis, meaning no organ failure or systemic or local complications often requires no imaging and most patients are discharged within one week. Moderately severe pancreatitis is defined as transient organ failure lasting no more than 48 hours and/or local or systemic complications without persisting organ failure, often have a longer hospital stay and higher mortality. Severe acute pancreatitis is characterised by the presence of persistent organ dysfunction lasting longer than 48 hours. These patients often have pancreatic necrosis with a mortality of at least 30%. Persistent organ dysfunction as determined by the modified Marshall score, usually accompanied by local complications is the hallmark of severe pancreatitis.
Another classification system, known as the Determinant Based Severity Classification looks at two factors – firstly, distant organ failure and secondly, local complications, namely necrosis of pancreatic or peri-pancreatic tissue. Using these two determinants, the DBSC subtypes pancreatitis into four categories; mild, moderate, severe and critical.
Either the Atlanta Classification or DBSC (Table 1) can be used and it is unclear which classification is better in predicting outcomes [26].
| Revised Atlanta Classification 2012 | Determinant Based Classification 2012 | |
|---|---|---|
| Mild | No organ failure and no local or systemic complications | No peripancreatic necrosis and organ failure |
| Moderately Severe | Transient organ failure (<48hrs) and/or local or systemic complications without persistent organ failure (>48hrs) | Sterile peripancreatic necrosis and/or transient organ failure (<48hrs) |
| Severe | Persistent organ failure (>48hrs) – single organ or multiple organ failure | Infected peripancreatic necrosis or persistent organ failure (>48hrs) |
| Critical | Infected peripancreatic necrosis and persistent organ failure |
Table 1: Comparison of Revised Atlanta Classification and Determinant Based Classification in regards to grading severity in acute pancreatitis.
Clinical scoring systems
Correct assessment as to the severity of pancreatitis is paramount as it directs aggressiveness of therapy. There are several clinical scoring systems available, but many are cumbersome to use in daily practice. Scoring systems available include the Modified Marshall Score, the APACHE II, SOFA, BISAP and Ranson criteria (Table 2). There are large variations in these scoring systems to predict severity with recent guidelines suggesting that existing scoring systems have limited value as they all have a good negative predictive value but low positive predictive value [27].
| Ranson’s Criteria | One of the earliest scoring systems in AP There are 11 parameters - 5 parameters are assessed on admissionand 6 during the next 48 hours Mortality increases with increasing score – 0-3% with score < 3, 11-15% score ≥3, and 40 % when the score was ≥6 [2]
|
||||||||||||||
| APACHE II | 12 physiologic measures of temperature, mean arterial pressure, heart rate,respiratory rate, oxygenation, arterial pH, serum sodium, potassium, creatinine, haematocrit, WCC, and Glasgow coma scale Extra points are given for age and presence of chronic disease Studies suggest that mortality is less than 4%percent with a score <8 and is 11 to 18 %with a score>8 [2] |
||||||||||||||
| CT Severity Index | Score is determined by degree of necrosis, inflammation, and the presence of fluid collections The first score is derived from non-contrast CT findings and the second score based on the percentage of necrosis seen on contrast enhanced CT A score of ≥6 indicates severe disease [29] |
Table 2: Scoring systems in AP.
The Modified Marshall score determines if there is organ failure by looking at renal, respiratory and cardiovascular parameters and is the scoring system utilised in the modified Atlanta Classification.
A simpler tool known as the bedside index of severity in acute pancreatitis (BISAP) is also useful and has been validated in a large cohort of patients for determining in hospital mortality [28]. Patients are assigned one point each for a BUN>25 mg/dl (8.9 mmol/L), altered mental status with a Glasgow Coma Scale<15, evidence of a systemic inflammatory response syndrome (when two of the following criteria are met 1) temperature<36°C or >38°C 2) respirations>20/min or PaCO2<32 mmHg 3) heart rate>90/min 4) WBC<4000/mm3 or WBC>12,000/mm3 or more than 10% bands found on blood smear), patient age>60 years or the presence of a pleural effusion over the first 24 hours. Those patients who have a score of zero have a less than 1% mortality whereas a score of 5 confers a 22% mortality rate.
Although the BISAP score maybe less cumbersome than the acute physiology and chronic health examination (APACHE) APACHE II, Ranson or Modified Marshall it has not been validated for predicting outcomes such as length of hospital stay or intensive care requirement.
The Balthazar CT Severity Index helps quantify severity of disease by assessing any morphological changes to the pancreas, presence of fluid collections and necrosis [29]. CT is the most important imaging modality tool that can help predict severity of disease and clinical outcomes [30]. A score of ≥6 indicates severe disease which has shown to reflect increased morbidity and mortality. In addition to these scoring systems, simple tests that are able to predict disease severity include CRP after 48 hours [31] and BUN/urea [32]. They have been found to be independent risk factors for disease severity.
Several studies have concluded that older age is a predictor of a worse prognosis, although the age cut off has varied from 55 to 75 years in different reports [2]. A retrospective study by Losurdo showed that older patients (age>65) undergo a more severe course of pancreatitis but without any increase in mortality. The study showed that the older patients had more co-morbidities which likely contributed to their more severe course [33].
Alcohol as a cause of pancreatitis has been associated with an increased risk of pancreatic necrosis and need for intubation in some reports. Infection is an important risk factor for adverse outcome in severe pancreatitis with a morality of 11% [34]. Persistent organ dysfunction has recently been accepted as a key determinant of prognosis being associated with a mortality of 36-50% [35] a combination of both had the highest impact factor [36]. Other clinical factor identified to negatively affect the outcome is obesity [37].
Course and complications
More than 80% of pancreatitis cases are mild and self-limiting known as interstitial oedematous pancreatitis. This is characterised by diffuse enlargement of the pancreas due to pancreatic oedema (Figure 1).
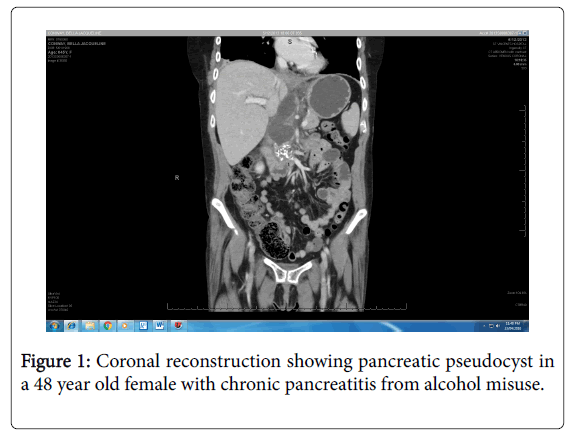
Figure 1: Coronal reconstruction showing pancreatic pseudocyst in a 48 year old female with chronic pancreatitis from alcohol misuse.
Acute pancreatitis fluid collection refers to development of a peripancreatic fluid collection within 4 weeks from the onset of acute pancreatitis and it is homogenous without an encapsulated wall. It occurs in the setting of interstitial pancreatitis. A pancreatic pseudocyst is a well-defined, encapsulated, homogenous peripancreatic collection that occurs after 4 weeks from the onset of pancreatitis (Figure 2).
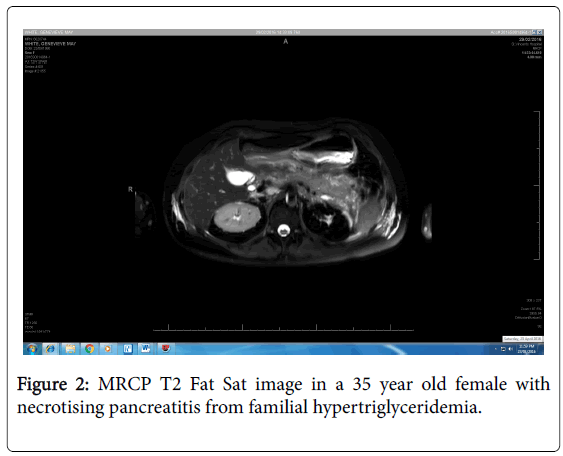
Figure 2: MRCP T2 Fat Sat image in a 35 year old female with necrotising pancreatitis from familial hypertriglyceridemia.
The remainder of patients will develop severe disease i.e. necrotising pancreatitis. This involves necrosis of pancreatic parenchyma, extrapancreatic tissue or both (Figure 3) [6].
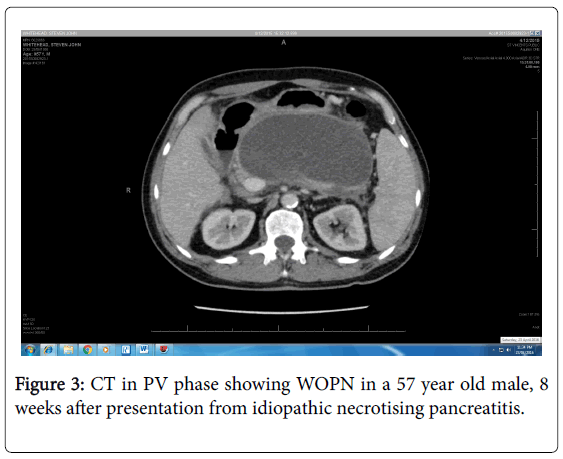
Figure 3: CT in PV phase showing WOPN in a 57 year old male, 8 weeks after presentation from idiopathic necrotising pancreatitis.
Pancreatic and peripancreatic necrosis can become infected or remain sterile. After the first week of the disease, a non-enhancing area of pancreatic parenchyma on CT is suggestive of pancreatic parenchymal necrosis. Acute necrotic collection is defined by a heterogenous, non-encapsulated collection containing fluid and necrotic material occurring within 4 weeks from onset of pancreatitis.
Walled off pancreatic necrosis (WOPN) is a mature, encapsulated collection of necrotic intra and peri-pancreatic material usually occurring after 4 weeks from the onset of acute necrotizing pancreatitis.
Pancreatic necrosis is the most severe local complication given the predisposition to infected necrosis, thought to be due to translocation of gut bacteria into the necrotic tissue. Infected necrosis occurs during the second or third week in up to 70% of severe pancreatitis patients with a large cohort study indicating the median time to development was 26 days [38]. Mortality can occur early (within 14 days), whereas delayed death (within 3 months) occur often as a result of the systemic inflammatory response from infected pancreatic necrosis [6]. Mortality in sterile and infected necrosis is 10 and 25% respectively [6].
The majority of infections are mono-microbial with gut-derived organisms such as Escherichia coli, Pseudomonas, Klebsiella, and Enterococcus. Fungal infections, usually with Candida carry a high mortality rate. Candida albicans is the most frequently isolated fungus in patients with necrotizing pancreatitis. Prolonged use of prophylactic antibiotics, prolonged placement of chronic indwelling devices, and minimally invasive or surgical interventions for pancreatic fluid collections further increase the risk of infection [39].
Systemic complications include respiratory problems, gastric outlet obstruction, splenic and portal vein thrombosis. Incidence of pulmonary complications is high in severe pancreatitis (between 15-55%) ranging from mild hypoexemia to acute respiratory distress syndrome [40] requiring intubation and intensive care monitoring. Also an episode of acute pancreatic can exacerbate patient’s previous medical problems such as coronary artery disease or COPD.
Management
Analgesia: Opioids are an appropriate choice in the treatment of acute pancreatitis pain. Compared with other analgesic options, opioids may decrease the need for supplementary analgesia. There is currently no difference in the risk of pancreatitis complications or clinically serious adverse events between opioids and other analgesia options [41]. Patient controlled analgesia (PCA) should be instituted early in the management of severe pancreatitis and analgesic requirements should be assessed daily.
Fluid resuscitation
Early fluid resuscitation is vital in the first 12-24 hours [42]. Adequate fluid resuscitation is paramount to prevent intravascular volume depletion, hypoperfusion and organ failure, Most patients will need up to 4 L for resuscitation, but some may require even up to 10 L. Recommendations suggest 5-10 ml/kg/hr but consideration for cardiovascular and/or renal comorbidities should occur. Assessing fluid status every 6 hours is important with the goal of hydration to decrease the blood urea nitrogen. The response to fluid resuscitation is based on heart rate, mean arterial blood pressure target of 65-85 mmHg, urine output 0.5-1 ml/kg/hour and a haematocrit of 35-44%. It is always important to be guided by clinical response to resuscitation with frequent patient assessment. Under resuscitation versus over resuscitation [43] are equally deleterious and therefore a fine balance is required. Aggressive fluid resuscitation is thought to affect pancreatic microcirculation, and fluid overload could further impair pancreatic tissue perfusion, leading to necrosis of the pancreas. Recommended fluid of choice is similar between guidelines with isotonic crystalloid such as Ringer’s Lactate being preferred.
Bile duct management/ERCP
Early ERCP with sphincterotomy should be performed in patients with pancreatitis and co-existing cholangitis. This should occur within 24 hours of presentation. In a meta-analysis performed in 2012, trials that included patients with cholangitis revealed that early ERCP reduced mortality, local and systemic complications as defined by the Atlanta Classification [44]. The meta-analysis confirmed that there was no role for early routinePancreatic duct stents and/or post procedure rectal indomethacin suppositories should be utilised to lower the risk of severe post-ERCP pancreatitis in high-risk patients as described previously. EUS or MRCP should be used to assess moderate probability cases of CBD stones with diagnostic ERCP being avoided.
Nutritional support
In cases of mild AP, oral feeding with a low fat diet should be encouraged on admission if there is no nausea or vomiting with resolution of abdominal pain. In cases of predicted severe AP, oral feeding can be encouraged if a patient requests it i.e. “an on demand strategy”. There is no superiority in early enteral feeding compared with oral feeding in the first 72 hours in terms of infection risk or mortality [45]. If by 72 hours, there is inability to tolerate oral feeding, enteral feeding (elemental or polymeric enteral formulations) via a nasogastric or nasojejunal tube should be started [46]. Enteral probiotics have no role in severe acute pancreatitis [47]. Total parenteral nutrition when compared with enteral nutrition may have added morbidity related to length of stay and complications of infections [48,49] and should be avoided unless enteral nutrition cannot be tolerated.
Antibiotics
Routine use of prophylactic antibiotics in severe acute pancreatitis should not be used as it does not impact on the incidence of infected pancreatic necrosis A meta-analysis examining 841 patients in fourteen trials showed that the use of prophylactic antibiotics did not reduce mortality or the incidence of non-pancreatic infections [50]. Antibiotics should be given in proven extra pancreatic infection, such Routine use of prophylactic antibiotics in severe acute pancreatitis should not be used as it does not impact on the incidence of infected pancreatic necrosis A meta-analysis examining 841 patients in fourteen trials showed that the use of prophylactic antibiotics did not reduce mortality or the incidence of non-pancreatic infections [50]. Antibiotics should be given in proven extra pancreatic infection, such as cholangitis, catheter-acquired infections, urinary tract infections or pneumonia.
Treatment of local complications
The cornerstone to managing complications of severe pancreatitis is that they are managed in a multidisciplinary centre with experience in the condition. Expertise from advanced endoscopists, interventional radiologists and surgeons is vital in such a complex disease.
Pancreatic necrosis: Prophylactic antibiotics are not indicated for sterile necrosis [51,52] and should be reserved for patients with established infection. Around 30% of patients will develop infected necrosis [53]. Infected necrosis should be considered in patients who deteriorate or fail to improve after a week of treatment. Routine percutaneous fine needle aspiration of peripancreatic collections to detect bacteria is not indicated, because clinical signs (persistent fever, increasing inflammatory markers) and imaging signs (appearance of gas within the collections) are accurate predictors of infected necrosis in the majority of patients [54]. Antibiotic treatment can alone heal infected necrosis in about two thirds of patients with a mortality of 7% [55]. Often multiple courses of antibiotics are necessary once infection is established. Antibiotics that have adequate pancreatic penetration include carbapenems, quinolones and metronidazole. The diagnosis of infection can be confirmed by EUS guided fine needle aspiration (FNA), although there is a risk of false-negative results Indications for intervention in necrotizing pancreatitis (either endoscopic, radiological or surgical) include clinical suspicion or documented infected necrosis not responding to antibiotics or in the absence of infection, persistent organ failure for several weeks after the onset of pancreatitis. Using a minimally invasive “step up” approach compared with open necrosectomy has been shown in a randomized controlled trial to reduce the rate of immediate complications (multiorgan failure, bleeding, perforation) and late complications (new onset diabetes, pancreatic insufficiency, hiatus hernia) and decrease cost by 12% [56]. In the step up approach the drain is inserted either percutaneously (CT guided) or endoscopically (EUS guided). At the time of the drainage procedure, fluid is aspirated and sent for bacterial and fungal analysis to further assist with choice of antibiotics. The timing of the intervention should be delayed where possible until 4 weeks after initial presentation to allow the collection to be walled off [54]. The PANTER trial showed that 35% of patients with infected necrotizing pancreatitis achieved complete recovery after percutaneous drainage only. If percutaneous drainage is utilised, then a retroperitoneal approach is preferred as it will help prevent fistula formation. Image guided catheter drainage and EUS guided drainage have similar outcome and both are superior to a minimally invasive surgical approach [56] as treatments for infected necrosis. The choice between image guided catheter drainage and EUS guided drainage depends upon the location of the collection, time from presentation, clinical condition of the patient and availability of local expertise. The position of the collection relative to the stomach, colon, liver, spleen and kidney is very important. In general, endoscopic drainage in preferred for retrogastric/retroduodenal collections and percutaneous approach for collections in the left or right flank behind the colon. Endoscopic approach is particularly advantageous when the pancreatic duct is obstructed or there the presence of a disconnected duct syndrome. In such cases, percutaneous approach is not recommended as it would result in protracted or indefinite external catheter placement. Due to complexity of the presentation, the aim is to provide a sound multidisciplinary approach involving interventional endoscopists, radiologists and surgeons [57]. If there is no clinical improvement, treatment can be escalated to EUS guided endoscopic necrosectomy or minimally invasive surgery (videoscopic assisted retroperitoneal debridement). The Penguin trial showed that endoscopic necrosectomy reduces the proinflammatory response and had lower rates of major complications (including multi-organ failure, intra-abdominal bleeding) as well as death compared to surgical necrosectomy (20% vs 80%) [58]. Most recently, lumen–apposing fully covered selfexpandable metal stent (LAMS) have become available for EUS guided drainage of peripancreatic fluid collections (WON and pseudocysts). Multicentre European and US studies have shown these stents to be a safe, easy to use and highly effective in managing pancreatic collections with a success rate of up to 88% in WOPN [59]. Open abdominal surgery is considered to be a last resort due to high morbidity and mortality.
Disconnected duct syndrome: Disconnected duct syndrome is a condition in which there is a full transection of the pancreatic duct following pancreatic necrosis that requires intervention, usually 6-8 weeks after the acute attack. In a study with 197 patients, it was found that up to 40% of patients with severe necrotising pancreatitis had disconnected duct syndrome and half of them required intervention [60].
Pseudocyst: Predictors of pseudocyst formation include alcohol as the cause of pancreatitis or initially severe disease [15]. Intervention should only occur if symptoms develop such as persistent abdominal pain, gastric outlet obstruction or biliary obstruction due to mass effect. EUS guided cystgastrostomy is the method of choice and should be performed at least 4-8 weeks after the onset of pancreatitis with a clinical success greater than 90%.
Abdominal compartment syndrome (ACS): ACS is defined as a sustained intra -abdominal pressure more than 20 mmHg that is associated with new onset organ failure. The incidence of intraabdominal hypertension is high, quoted to be nearly up to 85% [61] however most times the patients are asymptomatic. Medical management of ACS is preferred with options including nasogastric tube insertion, rectal decompression, diuretics and drainage of ascites. Surgical options include laparotomy, bilateral suboctal laparostomy or a subcutaneous linear alba fasciotomy.
Long term care/prevention
The prevention of recurrent attacks is aimed at treating the primary cause. Alcohol abstinence is key in preventing further episodes of acute pancreatitis due to alcohol misuse. In mild cases of biliary pancreatitis, cholecystectomy should be performed in the index admission [62-64]. In cases of necrotising pancreatitis cholecystectomy should be postponed until acute issues have resolved and fluid collections have stabilised (6 weeks or more).
Acute pancreatitis is one of the commonest presentations to emergency department of gastrointestinal disorders. Correct and timely assessment of severe cases leads to early intervention in specialized centered thus improving the mortality and morbidity associated with it.