Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Case Report - (2015) Volume 3, Issue 5
T lymphoblastic leukaemia (T-ALL) is a neoplasm of lymphoblasts committed to T-cell lineage and T-ALL is diagnosed by identification of immaturity markers and the lineage specific Cluster of Differentiation (CD) marker, CD3 in the leukemic cells. Here we report a 20 year old male who was diagnosed as case of T-ALL, whose leukemic blasts on morphology resembled the lymphoid cells seen in hairy cell leukemia (HCL) resulting in a diagnostic dilemma which was resolved subsequently by immunophenotyping. Even though the presence of cells with hairy projections is rarely reported in haematological malignancies other than HCL, ours is a first of its kind in TALL.
Keywords: Hairy cells; T-ALL; Hairy cell leukemia; Immunophenotyping
T lymphoblastic leukaemia (T-ALL) is a neoplasm of lymphoblasts committed to the T-cell lineage, typically composed of small to medium-sized blast cells with scant cytoplasm, moderately condensed to dispersed chromatin and inconspicuous nucleoli, involving bone marrow and peripheral blood.
The diagnosis of T-ALL is based on the expression of immaturity markers such as Cluster of Differentiation (CD) marker CD34, Terminal deoxynucleotidyl transferase (TdT), Human Leucocyte Antigen (HLA) DR and the lineage specific cytoplasmic or surface CD3 in the leukemic cells [1].
The cytoplasmic features of T-ALL include, pale blue cytoplasm with occasional presence of vacuoles on Romanowsky stain, however presence of fine hairy cytoplasmic projections is so far not mentioned in the literature. Here we report a case of T-ALL, which on morphology resembled hairy cell leukemia (HCL) resulting in diagnostic difficulty.
A 20 year old male, resident of Bihar (India) presented with three months history of left sided upper abdominal mass, fever and generalised weakness. On examination, he had pallor, massive Splenomegaly of 20 cms below left costal margin. There was no icterus, lymphadenopathy or hepatomegaly. Other systemic examination was within normal limits. Laboratory parameters revealed hemoglobin of 92 g/L, total leucocyte count of 20 × 109/L and platelet count of 45 × 109/L.
Jenner Giemsa stained peripheral smear examination (PS) revealed many smudge cells, mononuclear cells with spongy nuclear chromatin and some showing nucleoli. The cells had moderate amount of cytoplasm with circumferential fine hairy projections resembling cells seen in HCL. In addition, some cells with open nuclear chromatin resembling blasts and without the hairy projections were also noted (Figure 1).
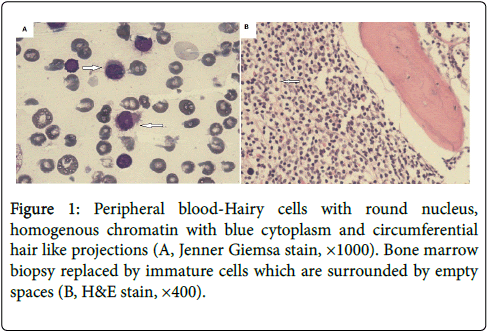
Figure 1: Peripheral blood-Hairy cells with round nucleus, homogenous chromatin with blue cytoplasm and circumferential hair like projections (A, Jenner Giemsa stain, ×1000). Bone marrow biopsy replaced by immature cells which are surrounded by empty spaces (B, H&E stain, ×400).
Bone marrow smears also revealed similar dual population of cells. Massive Splenomegaly, many smudge cells and hairy cells on PS, directed us towards a diagnosis of HCL. Subsequently cytochemistry and immunophenotyping (IPT) were carried out.
On cytochemistry, these cells were Tartrate resistant acid phosphatase (TRAP) negative and on IPT, the cells were negative for CD19, CD20, CD11c, CD25 and CD103 ruling out the diagnosis of HCL.
To our surprise on CD45/side scatter dot plot in flow cytometry, almost all of these atypical cells showed dim expression of CD45 and were found to lie in the blast region (Figure 2) and hence antibody panel for acute leukemia was applied.
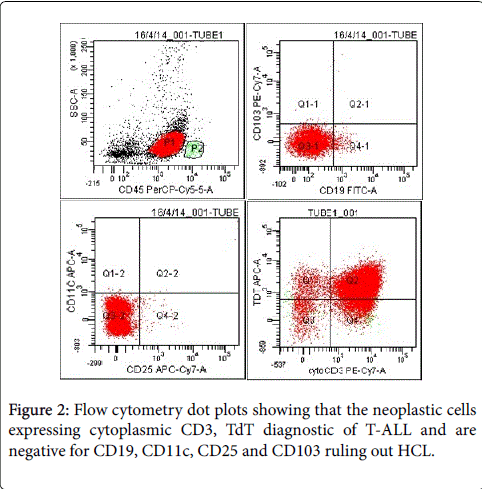
Figure 2: Flow cytometry dot plots showing that the neoplastic cells expressing cytoplasmic CD3, TdT diagnostic of T-ALL and are negative for CD19, CD11c, CD25 and CD103 ruling out HCL.
Divergent to the morphological features, these cells were positive for cytoplasmic CD3, TdT, CD2, CD5 and negative for myeloperoxidase (MPO), CD19, CD10, CD11c, CD64 confirming the diagnosis of TALL. On Hematoxylin and Eosin stain, bone marrow biopsy revealed a hypercellular marrow replaced by immature cells separated by empty spaces resembling the pattern noted in HCL. However reticulin stain done did not show increase in reticulin fibres. As morphology and immunophenotyping revealed contradictory findings, flow cytometry was repeated in the peripheral blood of the patient and we confirmed the diagnosis of T-ALL. Due to financial constraints patient went back to his native place, where he received chemotherapy at government hospital and further follow up is not available.
\Morphology plays a major role in diagnosis of hematolymphoid malignancy even though immunophenotyping is essential for confirmation in most of the cases. In a resource limited setting, morphology guides in setting up of panel of antibodies for diagnosis of acute leukemia/chronic lymphoproliferative disorders, either by flow cytometry (FCM) or immunohistochemistry (IHC). Thus morphology forms the basis for effective utilisation of more expensive techniques such as FCM or IHC. However morphology can be deceptive at times as brought out in this case. Even though the presence of hairy cells is a characteristic feature of HCL, cells with similar morphology are rarely reported in cases other than HCL. Tanioka et al. reported the presence of hairy cell morphology in a case of primary plasma cell leukemia [2]. Similarly presence of unusual hairy projections was noted by Ahluwalia et al. in a case of hepatosplenic T-cell non-Hodgkin lymphoma [3]. Our case also belongs to this category of non HCL cases showing the presence of circumferential hairy cytoplasmic projections resembling HCL and posing a diagnostic challenge. The issue was further complicated by several case reports in literature highlighting the coexistence of HCL in various haematological malignancies such as hepatosplenic T-cell non-Hodgkin lymphoma, Hodgkin lymphoma, peripheral T-cell lymphoma, multiple myeloma, chronic myeloid leukemia and chronic lymphocytic leukemia [4-9]. However in our case, immunophenotyping revealed most of the cells to be homogenously expressing the immaturity and T-cell phenotype marker confirming the diagnosis of T-ALL and ruling out the coexistence of HCL which otherwise could have contributed for this perplexing morphology. Since most of the cells in the blood and bone marrow turned out to be leukemic blasts on immunophenotyping, it can be safely assumed that the cells showing hairy cytoplasmic projections are leukemic blasts. No logical explanation could be offered for the presence of hairy projections in a case of T-ALL, however the presence of such morphology in leukemic blasts could have lead to misdiagnosis in the absence of imunophenotyping. Lee et al. observed that peripheral blood lymphocytes in patients infected with Coxiella burnetti were found to develop hairy projections when cultured [10] and may be a similar infection could have possibly contributed for the hairy projections in the leukemic blasts, even though the same cannot be said with certainty. This case is reported for the unusual morphology shown by the leukemic blasts, a first of its kind, in a case of T-ALL.