Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Case Report - (2015) Volume 3, Issue 2
Objective: To study the epidemiological, clinical, therapeutic and prognostic aspects of trauma in pregnancy at the Yalgado Ouedraogo teaching hospital in Ouagadougou.
Patients and Methods: A descriptive retrospective study was done over a period of three years from 1st January 2010 to 31st December 2012. Were included in our sample, all pregnant women admitted for trauma in pregnancy and eligible in three clinics: obstetrics/gynecology, orthopedics, general and visceral surgery. The data was collected using a structured questionnaire and were entered and processed using Epi data 3.1 and SPSS.
We recorded 224 emergency consultations for trauma in pregnancy out of 26,735 obstetric and gynecological consultations which gives a frequency of 0.8%. The mean age of our patients was 25.9 ± 5 years and mean parity was 1. Housewives accounted for 50% of patients and referrals were the mode of admission in 74.6% of cases. The causes of injury were dominated by road traffic accidents in 82.6% of cases, falls in 9.8% and assault in 7.6%. The mean gestational age of onset of trauma was 26.3 ± 7weeks amenorrhea. The management was multidisciplinary with a medical component in 99.1% of cases, obstetric component in 13% of cases, a visceral surgery component in 6.7% of cases and an orthopedic component in 4.2% case. Multiple traumas were found in 4 patients. The fetal prognosis showed in the 1st trimester 3 cases of abortion in the 2nd trimester 5 cases of intrauterine fetal death and in the 3rd trimester 10 cases of preterm labor
Conclusion: Traumas during pregnancy are relatively common. The complications of these traumas are severe and in their management are multidisciplinary. The establishment of a national strategy to prevent trauma in pregnancy will improve the prognosis for mother and child.
<Keywords: Trauma in pregnancy; Maternal and fetal prognosis;Ouagadougou
Trauma complicates up to 7% of all pregnancies. It’s the leading cause of death none related to pregnancy. The consequence of these injuries varies according to the term of gestation and the mechanism of occurrence [1-3].
In Burkina Faso, we noticed more and more increase in number of vehicles and motorcycles. The management of a pregnant woman victim of trauma is delicate and must be multidisciplinary, including obstetricians, intensive care specialists, surgeons and pediatricians [2,4]. In the absence of previous studies on trauma during pregnancy in Burkina Faso, we propose to describe the epidemiological, clinical, prognostic and therapeutic pattern of these injuries during pregnancy at the Yalgado Ouedraogo Teaching Hospital in Ouagadougou, Burkina Faso.
A descriptive retrospective study was done over a period of three years from 1st January 2010 to 31st December 2012.The study was conducted within the departments of obstetrics and gynecology, orthopedics and general and digestive surgery of Yalgado Ouedraogo Teaching Hospital (CHU-YO).
Were included in our study, all pregnant women outpatient and hospitalized cases, admitted for trauma in pregnancy during the study period in the three sites. The study variables included socio demographic characteristics, type of trauma, mechanism of the trauma, clinical and laboratory data, therapeutic and prognostic data. A structured questionnaire was used to collect data. Data were collected from clinical records, admission records and operative reports records at the obstetrics gynecology, orthopedics and general surgery.
The data were entered and analyzed on a personal computer by Epi data 3.1 and SPSS (Statistical Package for Social Science). Descriptive statistics for constant variables were defined as mean ± standard deviation, minimum and maximum values, and categorical variables were defined as number and percent.
Anonymity and confidentiality of collected data were respected.
Frequency
During the study period, we recorded 224 admissions for trauma in pregnancy for a total of 26,735 admissions representing a frequency of 0.8%.
Socio demographic characteristics
Age and parity: The mean age of our patients was 25.9 ± 5 years with a range of 17 to 42 years. The age group of 20-24 years accounted for 35.3% of cases. The average parity was 1 with a range of 0 to 8.
Professional and marital status socio: Housewives accounted for 50% of the sample, students 18.3%, employee with income 13.4%, the informal sector 10.3%, seamstresses and hairdressers 8%. Married women accounted for 62% of our patients, those living with a partner 25% and singles 13%.
Living area: Among our patients, 93.3% (209 cases) were living in urban areas and 6.7% in rural areas.
Clinical pattern
Mode of admission: Patients were brought in by ambulance in 74.6% cases, referred in 11.6%, and reported themselves in 13.8% of cases.
Reason for admission: The distribution of patients according to the reason for admission is presented in Table 1. The trauma has led to initial loss of consciousness in 25 cases, representing 11.2%.
| Reason for Admission Number | % | |
|---|---|---|
| RTA without ILC in pregnancy | 168 | 75 |
| RTA with ILC in pregnancy | 17 | 7,5 |
| Assault without ILC in pregnancy | 14 | 6,3 |
| Fall by herself without ILC in pregnancy | 12 | 5,4 |
| Fall from a tree without ILC in pregnancy | 5 | 2,3 |
| Assault with ILC in pregnancy | 3 | 1,3 |
| Fall from a tree with ILC in pregnancy | 3 | 1,3 |
| Fall by herself with ILC in pregnancy | 2 | 0,9 |
| Total | 224 | 100 |
RTA: Road Traffic Accident; ILC: Initial loss of consciousness
Table 1: Distribution of patients according to the reason for admission (n = 224).
Gestational age: The mean gestational age at the onset of trauma was 26.3 ± 7.7 weeks amenorrhea which range of 8 to 40.6. Trauma occurring in the first trimester accounted for 12.5%, 45.1% for the second trimester and 42.4% for the third.
Circumstances of injury: The distribution of patients according to the circumstances of the injury is shown in Table 2. The assaults and falls accounted for 17.4% of the circumstances of injury.
| Causes of traumas | Number | % |
|---|---|---|
| Road traffic Accident | 185 | 82,6 |
| Fall | ||
| • By herself | 14 | 6,2 |
| • From a tree | 8 | 3,6 |
| Assaults | ||
| • Violence among couples | 9 | 4 |
| Other assaults | 8 | 3,6 |
Table 2: Distribution of patients according to the circumstances of traumas (n=224).
Type of means of transport: Table 3 shows the distribution of road traffic accidents according to the means of transport involved. Motorcycle was involved in 99.5% of cases.
| Mean of transport involved | Number | % |
|---|---|---|
| Motorcycle-Motorcycle | 119 | 64,3 |
| Motorcycle -Car | 32 | 17,4 |
| Motorcycle-Pedestrian | 8 | 4,3 |
| Motorcycle only | 25 | 13,5 |
| Car-Car | 1 | 0,5 |
| Total | 185 | 100 |
Table 3: Distribution of Road Traffic Accident according to the mode of transport involved.
Seasonality of trauma: The distribution of patients according to the season and the type of trauma is shown in Figure 1.
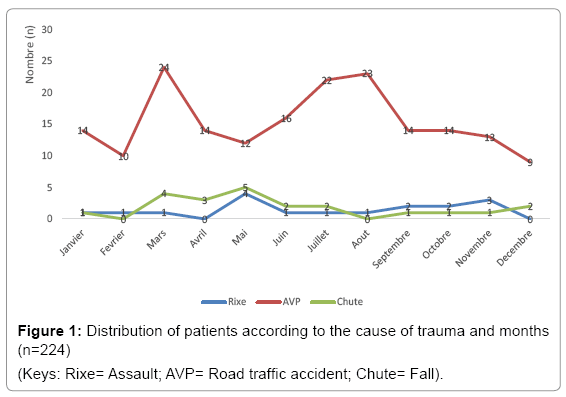
Figure 1: Distribution of patients according to the cause of trauma and months (n=224)
(Keys: Rixe= Assault; AVP= Road traffic accident; Chute= Fall).
Type of injury: The distribution of patients according to the type of injury has been shown in Table 4. Four cases of multiple injuries were noted including 2 by falls from a tree and 2 by road traffic accident.
| Type of trauma | Number | % |
|---|---|---|
| Abdominal contusion without viscous lesion | 79 | 35,3 |
| Limbs trauma | 67 | 30 |
| Head injury | 29 | 12,9 |
| Trauma of the pelvic | 15 | 6,7 |
| Maxillo-facial’s trauma | 13 | 5,8 |
| Spinal injury | 11 | 4,9 |
| Chest trauma | 5 | 2,2 |
Table 4: Distribution of patients according to the type of trauma.
Therapeutic
Emergency medical treatment: The medical treatment was provider in 99.1% of cases (222/224). It consisted of local skin care, administration of tetanus toxoid and tetanus immunoglobulin according to the vaccination status of the patient, the administration of antibiotics per os or intravenously in open wounds, the administration of antispasmodic orally or intravenously and anticoagulant administration for the prolonged immobilization cases.
Emergency obstetric treatment: Manual vacuum aspiration was performed in 1.3% of patients (3 cases). Tocolysis was performed in 3.2% of patients (7 cases) and fetal lung maturation in 3 cases representing 1.3%. Caesarean section was performed in 11 patients representing 4.9% of the sample and 8 patients (3.6%) delivered vaginally. The vaginal delivery was spontaneous in two cases and in 6 cases it was induced for intra uterine fetal death.
Orthopedic treatment: An orthopedic treatment was performed in 9 patients representing 4%. It was immobilization in 2 cases with POP, the insertion of Zimmer plate in 2 cases, the usage of a soft neck collar in 1 case, the installation of a mayo clinic in 1 case and a functional treatment in 3 cases due to non-displaced fracture of the obturator’s frame with or without of the pubic symphysis involvement.
Surgical treatment: Surgical treatment was provided in 15 patients representing 6.7%. It consisted of a chest tube insertion in a case of rib’s fracture with pleural effusion in the right chest; the incision and drainage of large hematoma of the left thigh with repair of perineal tear repair in 1 case; suture for vaginal tear in 3 cases and sutures in the skull, face or limbs in 10 cases.
Prognostic aspects
All patients benefited an emergency obstetrical ultrasound scan on admission to roll out a placental abruption, and were repeated after 48 hours in 93% of patients. The distribution of obstetric complications according to the term of pregnancy is shown in Table 5.
| Obstetrical consequences | 1st trimester | 2nd trimester | 3rd trimester | Total |
|---|---|---|---|---|
| Preterm labor | 10 | 10 | ||
| Placental Abruption | 4 | 4 | ||
| Intra uterine fetal death | 5 | 3 | 8 | |
| Abortion | 3 | 1 | 4 | |
| Threatened abortion | 2 | 2 | ||
| Uterine rupture | 1 | 1 | ||
| Total | 3 | 12 | 14 | 29 |
Table 5: Obstetrical complications according to the term of cyesis.
We noted 4 cases of multiple traumas and 1 case of uterine rupture with hemorrhagic shock. Among the 202 patients which were discharged with live intrauterine gestation, we were able to get in touch with 43 patients, and they were able to carry their pregnancies to term. The outcome was favorable in 97.8% of cases. No maternal death was recorded.
The average duration of hospital stay was 1.8 days ± 2, 4 hours with extremes of 0 and 24 days.
Epidemiology
Frequency: In our study, the frequency of trauma in pregnancy was 0.8%; it is higher than Kouame et al. [5] in Ivory Coast who reported a frequency of 0.02%. But lower than Traore et al. [6] in Mali who reported 1.9%. The frequency of trauma in pregnancy is steadily increasing. This increase may be related to several factors, including the increasing number of motorcycles and automobile fleet, the nonrespect of traffic regulations and the low economic status of women in poor countries. These traumas during pregnancy occur mostly among young women [5-8].
Circumstances of injury: In our study, the circumstances of the injury were dominated by road traffic accident in 82.6% of cases; falls in 9.8% and assaults in 7.6% of cases. Some authors have reported a predominance of road traffic accidents with frequencies between 49 and 74.3% [2,6,7]. The high frequency of road traffic accidents in Traore et al. [6] and our series, respectively 74, 3% and 82, 6% could be related to lack of strict implementation of the road traffic regulations. Indeed, motorcycles involved in 99.5% of accidents are ridded without obtaining the required driving license. In USA, domestic violence is a common cause of trauma during pregnancy. Intimate partner violence ranged from 1% - 20% and prevalence of domestic violence in pregnancy is 8307 to 100 000 live births [3,9].
Clinical pattern and management
Pelvic trauma: We recorded 13% of cases of head injuries. Traore et al. [6] and Schiff et al. [10] noted respectively 3.3% and 1.7% of head injuries cases. The head injuries observed during road traffic accident are major source of morbidity and require a special management at the intensive care unit. The injuries have led to pelvic fracture in 1.8% of cases. This frequency was 6.6% in the study of Traore et al. [6] and 1.7% in the Schiff at al. [10] study. In the pelvic fractures, the risk of fetal injury is more important if the presentation is cephalic and fixed. A pelvic fracture is not a definite contraindication for vaginal delivery even in the presence of a slightly displaced pelvic fracture [2,3].
Abdominal trauma: In our study, we recorded 35.3% of abdominal trauma. Kouame et al. [5] in Ivory Coast, Traore et al. [6] in Mali, Schiff et al. [10] in the United States of America have reported respectively some frequencies of 14, 3%; 13.2% and 4.4% [5,6,10]. Abdominal contusions were mostly observed during road traffic accidents involving motorcycles and during assaults. Their maternal and fetal complications can be multiple and their severity depends mainly on the mechanism of injury. According to some authors the Kleihauer test must be performed in any abdominal trauma during pregnancy.
The Kleihauer test is an essential element for the proper management of all pregnant women who had abdominal trauma to detect a fetomaternal hemorrhage which could be responsible for ischemic and hypoxic fetal disorder and peri ventricular leukomalacia [7].
In our study we found 4% of cases having placental abruption. Schiff et al. [10] and Traore et al. [6] reported 10.5% and 6.8% respectively. The placental abruption is secondary to stretching or damage to the placental disc due to trauma on the gravid uterus. The tocographic recording and ultrasound scan should be repeated regularly during 48 hours following a severe injury because the separations can have slow onset, sometimes taking several days to build up.
The traumas during pregnancy have led to abortion in 1.8% in our study. The role of stress as a result of shock is discussed in the literature, due to the oxytocin like effects of released catecholamine, but adrenaline level should be much higher than the physiological levels for this contractile action to occur. We noted preterm delivery in 5.4% of cases in our study. Kouame et al. [6], and Schiff et al. [10] found 28.6% and 9.5% of cases having threatened preterm labor respectively. The onset of preterm labor after trauma may be secondary to several factors: premature rupture of membranes, uterine contractions in relation to direct trauma to the uterus, or stress, or anoxia or direct irritation of uterus during laparotomy.
Prognosis
In our study, like that of Kouame et al. [5], we did not notice any maternal death. Traore et al. [6] reported 1.7% of maternal deaths. The trauma was associated with an initial loss of consciousness in 11.2% of cases, what predetermine the possible occurrence of secondary complications. Morbidity and mortality in trauma are not negligible. In our study and those of other authors, the fetal prognosis is marked by the occurrence of abortions and intra uterine fetal death, [5,6,11]. For Weiss et al. [11], following trauma, fetal mortality is 9 times greater than the maternal mortality and accounts for about 0.5% of fetal deaths. The trauma was complicated by fetal death in 4.5% of cases in our study. Our result is higher than Kouame et al. [5] who reported 1.4%. Missing data in relation to the evolution of pregnancy in our series may explain this difference. Fetal death may be related to placental abruption, massive Feto maternal transfusion, uterine rupture, a fetal trauma, maternal hemorrhagic shock or maternal death.
To further improve maternal and fetal outcome in our context, a strengthening of road safety measures, medical transport of trauma victims as well an early, appropriate and multidisciplinary managements prove to be essential. Generally the maternal and fetal prognosis has been improved since the introduction of compulsory wearing of seat belts [12].
Traumas during pregnancy are relatively common. The complications of these traumas are severe and in their management are multidisciplinary. The establishment of a national strategy to prevent trauma in pregnancy will improve the prognosis for mother and child.