Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2015) Volume 0, Issue 0
In 10 JAK2V617F positive patients with early myeloproliferative essential thrombocythemia (ET) or polycythemia vera (PV) we sequentially used the Polycythemia Vera Study Group (PVSG), the Thrombocythemia Vera Study Group (TVSG) and the 2008 WHO criteria for the clinical diagnosis of essential thrombocythemia (ET) ad polycythemia vera (PV). Subsequently, we evaluated bone marrow features and laboratory and molecular markers including endogenous erythroid colony (EEC), serum erythropoietine (EPO) mutation for the classification of early MPD. Six symptomatic patients had a delayed diagnosis of slow onset latent (masked) ET and 4 patients presented with rapid onset PV associated with thrombocythemia. We could clearly distinguish three phenotypes of ET when the 2008 European clinical, molecular and pathological (2008 WHO-ECMP) criteria for ET and PV are applied. These include ET phenotype 1, ET phenotype type 2 with features of early polycythemia vera (PV) and normal red cell mass, and ET phenotype 3 associated with megakaryocytic granulocytic myeloproliferation (ET-MGM) in the absence of characteristic features of primary myelofibrosis (PMF). Through the presentation of a number of highly illustrative clinical cases during long-term follow-up we could demonstrate that diagnostic differentiation of three phenotypes of ET is important, because natural history clearly differ.
Keywords: Myeloproliferative disorders; Essential thrombocythemia; Polycythemia vera; Chronic idiopathic myelofibrosis; JAK2V617F mutation; Bone marrow pathology.
As the classifications of the Polycythemia Vera Study Group (PVSG) and the World Health Organisation (2001 WHO) used a platelet count of 600 × 109/l as the minimum criterion for the diagnosis of essential thrombocythemia (ET) the early prefibrotic stages of myeloproliferative disorders (MPD) with platelet counts below 600 × 109/l are overlooked by the PVSG and WHO [1,2]. This comprises about 30% of masked MPD indicating the need to lower the platelet count cut-off to 400 × 109/l as the upper limit of normal counts for the clinical diagnosis of ET in prefibrotic MPDs [3]. The criteria of the Thrombocythemia Vera Study Group (TVSG) for the diagnosis of ET introduced a platelet count above 400 × 109/l and the presence of enlarged megakaryocytes in bone marrow smear and biopsy as pathognomonic clues to ET in various prefibrotic MPDs [4-6], whereas the PVSG criteria for ET exclude all variants of thrombocythemia associated with classic PV, primary myelofibrosis (PMF) or myeloid metaplasia with myelofibrosis, myelodysplastic syndrome and Philadelphia chromosome positive chronic myeloid leukemia [1]. The 2008 WHO investigators reduced the minimum platelet count to 450 × 109/l for the diagnosis of ET. In the present study we demonstrate that the TVSG, PVSG and 2008 WHO criteria for JAK2V617F mutated ET comprises three phenotypes of ET when the 2008 European clinical molecular and pathological (2008 WHO-ECMP) criteria are applied [5,6]. The importance to distinguish three phenotypes of ET as manifestations of prefibrotic MPDs because natural history and treatment options differ.
Blood cell counts, laboratory investigations, and bone marrow aspiration were performed routinely. Red cell mass and plasma volume were measured using Cr51-labeled autologous erythrocytes and J131-labeled albumin respectively. Blood and bone marrow smears were stained by the May-Grünwald-Giemsa method and processed for the periodic acid-Schiff (PAS) reaction. The leukocyte alkaline phosphatase (LAP) score was determined with the cytochemical technic of Hayhoe and Quaglino [7]. Bone marrow biopsies were done with a Jamshidi needle and embedded in glycol methylcrylate without decalcification.
Sections were stained with hematoxylin-azophyloxin, PAS, gallamine-Giemsa, and Gomori’s reticulin method. Detection of the Philadelphia chromsome was performed using the FISH technique. Detection of the JAK2V617F mutation was performed using PCR technique as described [8]. Heterozygous JAK2V617F mutation was defined as a mutant band of clearly less intensity as compared to JAK2 wild type band.
Ten MPD patients with either ET or early stage PV according to TVSG6 and PVSG1 criteria (Table 1) were referred to us between January 1 2003 to August 2007 for diagnostic evaluation according to WHO classifications [2,5] and treatment recommendation. Diagnostic evaluation included a complete clinical history, physical examination, retrospective laboratory data collection from hospital records, actual complete peripheral blood cell counts, white blood differential count, leukocyte alkaline phosphatase (LAP) score, peripheral blood (PB) morphology for the presence large platelets, tear drop red cells, erythroblasts, screening for the JAK2V617F mutation using PCR test8, bone marrow aspirate for morphology, endogenous erythroid colony (EEC), red cell mass measurement, spleen size on echogram and bone marrow histopathology from biopsies taken from the iliac crest.
| Inclusion criteria proposed by the TVSG [13,18] and WHO-ECMP [12,20] | |
| Platelet count in excess of 350 to 400×109/l and no known cause of reactive thrombocytosis | |
| Presence of large platelets in a peripheral blood smear and enlarged (giant), mature megakaryocytes with hyperploid nuclei in a bone marrow smear. No dry tap. | |
| Presence of the JAKV617F or MPL515 mutation | |
| Increase and clustering of enlarged mature or pleiomorphic megakaryocytes with hyperploid nuclei in bone marrow biopsy material and no slight or moderate increase of reticulin fibrosis (RF) and no increase of collagen fibrosis in bone marrow biopsy sections (Wilkins, Blood). | |
| Splenomegaly on palpation, or on ultrasound scan (echogram) | |
| Spontaneous endogenous erythroid colony (EEC) formation and/or spontaneous megakaryocytic colony formation (CFU-Meg) | |
| Exclusion criteria proposed by the PVSG [10,11] | |
| Known cause of reactive thrombocytosis | |
| Hematocrit (ht) >0.48 females and >0.51 males, or increased red cell mass (RCM gold standard to differentiate between ET and PV in type 2 ET) |
|
| Ph-chromosome or brc/abl rearrangement to exclude CML | |
| Tear drop erythrocytes and no leuko-erythroblastosis | |
| Features of MDS in bone marrow smear and biopsy | |
| No stainable iron bone marrow, low ferritine and low mean red cell volume (MCV) | |
| Dry tap due to moderate reticulin or collagen fibrosis of the bone marrow in biopsy sections | |
Table 1: Inclusion and exclusion criteria for the clinical diagnosis of essential thrombocythemia (ET) proposed by the Thrombocythemia Vera Study Group (TVSG) [13,18] Polycythemia Vera Study Group (PVSG) [10,11] and WHO-ECMP [12,20].
Personal experiences and previous reports produced very good evidence that the TVSG and PVSG criteria for the clinical diagnosis of ET (Table 1) comprises three phenotypes of ET when the 2008 WHO-ECMP criteria for ET are applied: ET phenotype 1, ET phenotype 2 with features of early PV (prodromal PV) and ET phenotype 3 with chronic megakaryocytic granulocytic myeloproliferation (ET-MGM) (Table 2) [5,9-11]. In the present study we compare the TVSG, PVSG and 2008 WHO criteria for ET with the WHO-ECMP criteria for ET in patients with early stages of prefibrotic MPD to detect the predicted three phenotypes of ET [4,9].
| Clinical and molecular criteria | WHO bone marrow criteria |
| ET type 1 | True ET |
| Platelet count of >400 ×109/l and the presence of large platelets in a blood smear Presence of JAK2-V617F or MPL515 mutation in about 50-60% Normal hematocrit: male <51 %, female <48 % |
Predominant proliferation of enlarged mature megakaryocytes with hyperlobulated nuclei and mature cytoplasm, lacking conspicuous morphological abnormalities. No increase, proliferation or immaturity of granulopoiesis or erythropoiesis. No progression to myelofibrosis. |
| ET type 2 | Early PV |
| Platelet count of >400 ×109/l and hematocrit in normal or upper normal range: male <51 %, female <48 % (normal RCM optional) Presence of JAK2-V617F mutation is mandatory Low serum EPO level and/or increased LAP score Spontaneous EEC. |
Increased cellularity with trilineage myeloproliferation (i.e. panmyelosis). Proliferation and clustering of small to giant (pleomorphic) megakaryocytes. No pronounced inflammatory reaction (plasmacytosis, cellular debris). Absence bone marrow features consistent with congenital polycythemia and secondary erythrocytosis. Progression to low risk PV during follow-up. |
| ET type 3 | ET MGM |
| Platelet count of>400 ×109/l and no signs of leuko-erythroblastosis Slight splenomegaly on ultrasound No anemia with Hb and ht in the normal or lower range of normal: >12g/dl Presence of JAK2-V617F or MPL515 mutation in about 50-60% No preceding or allied of CML, PV, RARS-T or MDS. |
Increased cellularity due to chronic megakaryocytic and granulocytic myeloproliferation (CMGM) and normal or slightly reduced erythroid precursors. Loose to dense clustering of giant pleiomorphic megakaryocytes with hyperploid nuclei and the presence of atypical small medium and giant immature megakaryocytes containing clumsy (cloud-like) lobulated nuclei. Progression to post-ET myelofibrosis in about 10 to 15% after more than 10 years follow-up. |
Table 2: Classification of TVSG-PVSG defined ET according to WHO and European clinical molecular pathological (WHO/ECMP) criteria into 3 phenotypes; important to differentiate because natural history
differs. Minimal criteria for the diagnosis according to WHO/ECMP criteria [9]: ET type 1 or True ET: 1 and ET bone marrow features ET type 2 or Early PV: 1 and 2 plus PV bone marrow features; 3 and 4 are confirmative for PV. ET type 3 or ET-MGM: 1 and 2 plus CMGM bone marrow features. EEC, JAK2V617F and/or MPL515 mutations confirm clonal MPD. Masked MPD: normal platelets, leukocytes and hematocrit, but slight splenomegaly on echogram with the presence of JAK2V617F mutation and/or a WHO bone marrow is rare (rather frequent in patients with splanchnic vein thrombosis and/or Budd Chiari syndrome).
Ten patients with early stage MPD presented with atypical cerebral ischemic attacks: 6 with ET in various prefibrotic MPDs and 4 with PV. The ages of patients at time of first symptoms and increased platelet count ranged from 21 to 53 years for ET and from 39 to 50 years for PV. The atypical TIAs in 6 ET patients ranged from transients attacks of transient blindness, diplopia and scotomas to migraine-like attacks followed by throbbing headaches, nausea, vomiting or even seizures. The time lapse between the first symptoms of migraine-like TIAs and the delay in diagnosis of ET in 5 patients ranged from 4 to 12 years. Three ET patients with features of early PV in the initial bone marrow biopsy indeed developed overt PV after a follow-up period of more than 10 years (cases 3, 4 and 5, Figure 1 and Table 3).
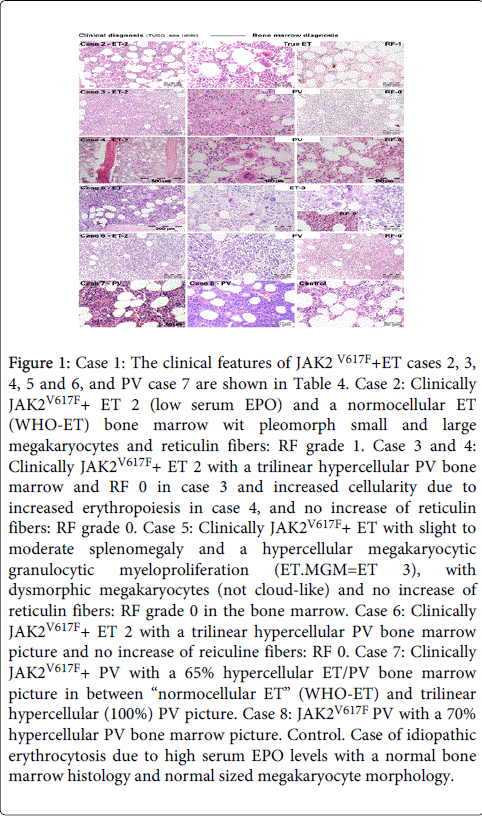
Figure 1: Case 1: The clinical features of JAK2V617F+ET cases 2, 3, 4, 5 and 6, and PV case 7 are shown in Table 4. Case 2: Clinically JAK2V617F+ ET 2 (low serum EPO) and a normocellular ET (WHO-ET) bone marrow wit pleomorph small and large megakaryocytes and reticulin fibers: RF grade 1. Case 3 and 4: Clinically JAK2V617F+ ET 2 with a trilinear hypercellular PV bone marrow and RF 0 in case 3 and increased cellularity due to increased erythropoiesis in case 4, and no increase of reticulin fibers: RF grade 0. Case 5: Clinically JAK2V617F+ ET with slight to moderate splenomegaly and a hypercellular megakaryocytic granulocytic myeloproliferation (ET.MGM=ET 3), with dysmorphic megakaryocytes (not cloud-like) and no increase of reticulin fibers: RF grade 0 in the bone marrow. Case 6: Clinically JAK2V617F+ ET 2 with a trilinear hypercellular PV bone marrow picture and no increase of reiculine fibers: RF 0. Case 7: Clinically JAK2V617F+ PV with a 65% hypercellular ET/PV bone marrow picture in between “normocellular ET” (WHO-ET) and trilinear hypercellular (100%) PV picture. Case 8: JAK2V617F PV with a 70% hypercellular PV bone marrow picture. Control. Case of idiopathic erythrocytosis due to high serum EPO levels with a normal bone marrow histology and normal sized megakaryocyte morphology.
| Case | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| Age years F/M56/M | 60/M | 66/F | 47/F | 40/F | 31/F | 43/F | 50/M | 47/F | 38 | |
| Platelets ×10/L 575 | 814 | 544 | 553 | 425 | 576 | 405 | 397 | 924 | 450 | |
| JAK2V617F mutation | nt | + | + | + | + | + | + | + | + | + |
| Serum EPO zero | nt | zero | 2 ↓ | nt | nt | 3↓ | 2 | zero | zero | |
| Leukocytes x10/l10.8 | 6.7 | 5.3 | 12.9 | 8.2 | 6.1 | 6.2 | 14.3 | 7.3 | 13.1 | |
| LAP score (N=<100) | nt | 160 | 197 | N | N | 186 | 263 | ↑ | 232 | 284 |
| Hemoglobin g/dl n19.8 | 13.6 | 15.5 | 14.2 | 14.4 | 8.4 | 14.0 | 17.3 | 18.6 | 16.3 | |
| Hematocrit 0.64 | 0.40 | 0.45 | 0.44 | 0.44 | 0.40 | 0.41 | 0.52 | 0.63 | 0.53 | |
| Erythrocytes x1012/L | nt | 5.3 | 4.8 | 4.6 | 5.9 | nt | 6.3 | 7.4 | 9.2 | |
| EEC | nt | + | + | nt | nt | + | nt | + | + | + |
| Red cell mass↑↑ | nt | nt | N | nt | N | nt | nt | ↑ | ↑ | |
| Spleen, echogram cm | nt | 13 | 16 | 13 | 13.7 | 11.8 | 6.5 | 13 | 14.3 | 13 |
| Diagnosis according to Clinical no BMB | ET | ET | ET | ET | ET | ET | PV | PV | PV | PV |
| BM pathology alone | ET | ET | PV | PV M |
PV MG |
U | PV | PV | PV | |
| PVSG | U | ET | U | U | U | U | IE | IE | PV | PV |
| TVSG/PVSG | ET | ET | ET | ET | ET | ET | PV | PV | PV | PV |
| 2007 WHO | ET | ET | U | U | U | U | PV | PV | PV | PV |
| WHO-ECMP | ET-1 | ET-1 | ET-2 | ET-2 | ET-2 | ET-3 | PV | PV | PV | PV |
| MPD sequence - | - | PV | PV | PV | - | - | - | - | - | |
| Follow-up, years | 4 | >12 | >10 | 10 | 8 | >11 | 1 | 1 | 1 | 1 |
Table 3: Clinical, molecular and pathological features of 10 patients with either essential thrombocythemia (ET), early or overt polycythemia vera (PV) diagnosed according to various classification systems PVSG, TVSG/PVSG, 2007 WHO and 2008 WHO-ECMP.
One ET patient (case 5) presented with ET type 3 with no progression of reticulin fibrosis during more than 11 years follow-up. In one PV patient bone marrow biopsy was inadequate for making a corret diagnosis. Three PV patients (cases 8,9 and 10) had a documented short history of about 1 year with increased values for blood cell counts (hemoglobin, leukocytes and platelets) and presented with fatigue, atypical cerebral disturbances and vertigo, which were reversible after blood letting.
One PV patient (case 8) developed aspirin-responsive microvascular circulation disturbances during follow-up at increased platelet counts and intraabdominal bleeding at platelet count around 1250 × 109/l while on low dose aspirin.
In all patients bone marrow smears and biopsy samples showed clustering and increase of mature or pleiomorphic enlarged megakaryocytes and no increase of reticulin fibers as a pathognomonic clue to the diagnosis of MPD. Spleen size on echogram (normal value <12 cm length diameter was slightly increased in all ET and PV patients. The spleen was palpable in two who had a spleen length diameter on echogram of about 16 cm on echogram.
PVSG defined clinical diagnosis of ET and PV can be made by the combined use of complete blood cell counts, peripheral blood and serum EPO levels in patients carrying JAKV617F mutation without the need of bone marrow biopsy (BMB) and red cell mass RCM) measurement. Bone marrow histology does not differentiate between ET and PV (Figure 1), whereas RCM is the gold standard to differentiate between ET and PV. Based on complete peripheral blood cell counts, laboratory features including red cell mass measurement, and bone marrow histopathology according to PVSG and TVSG criteria the diagnoses were ET in 6 and PV in 4 cases (Table 1).
According to 2008 WHO criteria the diagnoses are ET in 2, unclassifiable in 4, and early or overt PV in 4 patients. According to WHO-ECMP criteria the diagnosis were ET phenotype 1 in 1, ET phenotype 2 with features of early PV or prodromal PV with low serum EPO, the presence of EEC and normal values for hemoglobin, hematocrit and red cell mass in 3, ET phenotype 3 with features of MGM in the bone marrow biopsies and no leuko-erythroblastosis in 1, and PV in 4 patients.
Based on bone marrow histopathology alone for the classification of MPD by expert pathologists the diagnoses were ET in 2, ET type 3 MGM in one and early PV in 7 patients. Using the TVSG/PVSG inclusion and exclusion criteria subsequent bone marrow histopathology combined with complete blood cell counts, serum EPO levels according to 2008 WHO-ECMP criteria (Tables 2 and 3), we could distinguish 3 phenotypes of ET from early and overt stage PV carrying the JAK2 mutation without the need of RCM measurement. Bone marrow biopsy (BMB) for histopathological evaluation is a sensitive and specific clue and mandatory to pick up JAK2V617F mutated ET and PV and JAK2 wild type ET, PV and myelofibrosis (MF).
The latent and masked MPDs are underreported simple because the PVSG and 2008 WHO criteria for ET and PV do not define precisely and therefore frequently overlook the early stages of thrombocythemia in various MPDs. Several cases with occult or latent MPD went symptomatic usually microvascular disturbances for a few, several or even more than ten years [10,11] but are frequently not or never diagnosed until they are severely symptomatic including minor stroke, stroke, acute coronary syndrome [12], Budd-Chiari syndrome or splanchnic vein thrombosis [13-17]. The migraine-like TIAs in 6 of 7 presented ET patients responded to low dose aspirin and are identical to those reported in previous studies [18,19]. The migraine-likel TIAs as well as the diagnosis of ET in 4 of 6 symptomatic patients were not recognized because of unfamiliarity with its typical clinical appearances and their causal relationship. The link between long-lasting relief of erythromelalgia and migraine-like TIAs by aspirin in early stages of ET and PV can only be made by bone marrow histology as the diagnostic clue and proof of this causal relationshipbetween unrecognized erythromelalgia and migraine-like TIAs in thrombocythemia [19]. The time interval between onset of migraine-like TIAs and diagnosis of ET in cases 1, 3 and 4 ranged from 4, 6 and 9 years. The symptoms of migrainelike TIAs are the result of platelet activation, aggregation leading to transient ischemic disturbances in the cerebral microcirculation [19]. Such attacks of migraine like TIAs are very likely associated with overt signs of platelet activation as documented by increased levels of beta-thromboglobulin and platelet factor 4 as compared to much lower value outside the attacks [20]. The long-lasting effect given by aspirin is lacking in other types of migraine-like headaches. If left untreated migraine-like TIAs may progress to typical TIAs or minor strokes with cerebral functional defects may suddenly and unexpectedly occur during long-term follow-up.
The 2008 WHO diagnostic criteria for MPD are a significant step forward as compared to the PVSG and 2001 WHO diagnostic MPD criteria but do not meet the needs of clinicians in daily practice for three main reasons [4]. First, the 2008 WHO criteria for ET only include normocellular ET at platelet count in excess of 450 × 109/L with a bone marrow histology showing a monolinear proliferation enlarged mature megakaryocytes with a normal or only slightly increased erythro/granulopoiesis and therefore do not define prodromal PV and exclude early stage masked PV. Second, the 2008 WHO criteria for the diagnosis of PV use the combination of increased hemoglobin and hemotocrit values and thepresence of the JAK2V617F mutation as major criteria and a hypercellular bone marrow and low serum erythropoietine as minor criteria. Consequently the 2008 WHO criteria will miss a large group of masked PV and early PV mimicking ET with increased platelet count, slight splenomegaly and normal hemoglobin (<18.5 for men and <16.5 for women) and increased trilinear myeloproliferation (panmyelosis), low serum erythropoietine and the presence of the JAK2 mutation. Red cell mass measurement still remains the objective method of choice to distinguish masked PV but the so-called “forme fruste PV mimicking ET” do not meet the 2008 WHO criteria for overt PV1 [21,22]. The identification of such cases is clinically and therapeutically relevant because the incidence of PV related symptoms thrombotic complications dramatically increase in PV patients at increasing hemoglobin, hematocrit and erythrocyte counts when not on aspirin. Third, the diagnostic differentiation of ET in various MPDs without leukoerythroblastosis from thrombocythemia associated with myelofibrosis (MF) or myeloid metaplasia with leukoerythroblastosis is clinically of huge importance, but has not been addressed by the 2008 WHO classification. Fourth, the 2008 WHO classification disregard increase of leukocytes, platelets, serum EPO levels and spleen size as typical presenting features of ET in various MPDs and in trilinear PV. Simple tests like blood cell counts including platelets, leukocytes, hematocrit and erythrocytes, spleen size on echogram, EEC, and LAP score are even not taken into account to distinguish the latent (masked), early and overt thrombocythemic and erythrocythemic stages of PV from the overt trilinear polycythemic stage of classic PV.
In the present article we prospectively evaluated the 2008 WHO-ECMP criteria in 10 cases of JAK3V617F positive prefibrotic MPD during follow-up of a few to more that 10 years. ET phenotype 1, ET phenotype 2 with features of early PV and ET phenotype 3 with MGM bone marrow have been recognized in the present study by using the 2008 WHO-ECMP criteria for diagnosis, classification, staging of ET and PV patients. The distinction of three phenotypes of ET has important implications for for prognosis prediction and treatment [6,23]. A set of relevant bone marrow criteria for the diagnosis of normocellular ET and its distinction from the early PV and prefibrotic hypercellular MGM has been proposed by Michiels et al in 2006 and 2007 (Table 4) [24-26]. By taking histopathological features from bone marrow biopsies into consideration three main types of prefibrotic MPDs are to be distinguished including true ET, early PV and ET with a hypercellular MGM bone marrow. The existence of ET phenotype 2 with features of early PV and increased erythropiesis at the bone marrow level has been confirmed [27-31]. Evidence accumulate for the existence of ET phenotype 3 with a MGM bone marrow with slight to moderate increased cellularity (60-80%) due to increased granulopoiesis with slight to moderate increased megakaropoiesis (with normal blood cell counts and no leukoerythroblastosis as defined in Table 2) is much more frequent than the early prefibrotic or overt fibrotic hypercellular (90-100%) MF meeting the 2008 WHO criteria. The so-called prefibrotic and early fibrotic chronic or primary megakaryocytic granulocytic myeloproliferation (CMGM/PMGM) in the complete absence of previous ET or PV was first described by Georgii in 1990 CMGM labeled by Thiele as CIMF clearly differs from ET phenotype 3 and can be decribed as JAK2 wild type primary megakaryopoiesis and granulopiesis myeloproliferation (PMGM), which usually presents with pronounced thrombocythemia, no or slight leukoerythroblastis, anemia and/or splenomegaly and bordeline inceased LDH. PMGM has never been observed as the presenting feature of JAK2V617 positive MPD and very likely reflect a third type of JAK2 wild type subacute MPD featured by significant loss of life expectancy due to a high risk of myelofibrotic progression and developing typical features of PMF as defined by the 2008 WHO classification [31,32].
| Clinical and Molecular criteria | Pathological criteria (WHO) |
| Major PV criteria | P 1. Early PV Increased cellularity of bone marrow predominantly due to increased erythropoiesis and loose clusters of large megakaryocytes with hyperlobulated nuclei. No or slight increase of granulopoiesis and reticulin fibrosis. P 2. Overt PV Hypercellular (75-100%) bone marrowdue to trilinear increase of erythropoiesis, megakaryopoiesis and granulopoiesis and clustering of small to giant (pleomorph) megakaryocytes with hyperlobulated nuclei. Absence of stainable iron. P3. Erythrocytosis Selective increase of erythropoiesis, normal granulopoiesis and megakaryocytes of normal size, morphology and no clustering of megakaryocytes in primary or secondary erythrocytosis Grading of reticulin fibrosis (RF 0,1, 2, 3) |
| A0. Early PV. Hematocrit in the upper limit of normal: Ht: 0.45 to 0.51 in male and 0.43 to 0.48 in female23 A1. Classical WHO defined PV: Hematocrit >0.51/>0.48 in male/female A2. Presence of JAK2V617F mutation (sensitivity 95%) or exon 12 mutation A3. Low serum EPO level and/or spontaneous endogenous erythroid colony (EEC) formation |
|
| Minor MPD criteria | |
| B1. Persistent increase of platelet count: grade I: 400-1500, grade II: >1500 B2. Granulocytes >10 ×109/l or Leukocytes >12 ×109/l and/or raised LAP-score or increased PRV-1 expression in the absence of fever or infection B3. Splenomegaly on palpation or on ultrasound echogram (>12 cm length in diameter) |
Table 4: The 2008 WHO and European clinical, molecular and pathological (WHO-ECMP) Criteria for the Diagnosis of Polycythemia Vera (PV) and diagnostic differentiation between PV and congenital or acquired erythrocytosis [12]. WHO/ECMP criteria for early and overt PV [12]. A0, A2, B1 and P1 or P2 establish early PV (ET type 2) PV ECMP stage 0, or masked PV A1, A2, P1 and none of B establish so-called idiopathic erythrocytosis or erythrocythemic PV ECMP stage 1 A1, A2, P2 and one or more of B establish WHO defined classic and advanced PV ECMP stage 2 and 3 A1 and P3 with normal or increased values of serum EPO is consistent with congenital or secondary erythrocytosis. A3 confirms early and overt PV without the need of red cell mass measurement for clinicians who do not have access to a hematopathologist expert in MPD.
The proposed new 2008 WHO-ECMP criteria for the diagnosis and classification of thrombocythemia patients by using blood cell counts, spleen size on echogram, JAK2 mutation screening, serum EPO followed bone marrow biopsy and EEC have the great advantage to detect three phenotypes of ET as well as thrombocythemia associated with classic PV and prefibrotic or early fibrotic hypercellular PMF. As could be documented in the presented pilot study, the early stages of ET type 2 may precede PV for several up to more than 10 years. This type of slow onset PV clearly differs from acute onset of full blown PV without a previous history of MPD. Whether these two types of PV do differ at the biological level (hetero/homozygosity for the JAK2V617F mutation) and natural history with regard to progression to myeloid metaplasia and myelofibrosis remains to be established in prospective observational and basic research studies. Data on the natural history of JAK2V617F negative ET without features of PV are not considered in this pilot study but should be investigated separately in newly diagnosed patients. The 2008 WHO-ECMP classification and staging of MPD will have a major impact on the early detection of symptomatic ET and PV patients allowing clinicians to properly manage the platelet-mediated microvascular circulation disturbances and bleeding complications due to acquired von Willebrand syndrome thereby postponing or even preventing the occurrence of major thrombotic complication at increasing ages above 60 years.
We conclude that the 2008 WHO-ECMP inclusion and exclusion criteria for the diagnosis of ET indeed do include three variants of prefibrotic MPD (Tables 1 and 2): normocellular ET, early PV mimicking ET, and ET associated with a MGM bone marrow (Table 2). These three phenotypes of ET without leukoerythroblastosis do not differ significantly with regard to their clinical manifestation of thrombosis and bleeding and are to be treated similarly. In contrast to normocellular ET, ET with features of PV (prodromal PV do develop overt PV after 8 to more than 10 years follw-up, whereas ET.MGM very likely is a variant of masked PV with slight to moderate splenomegaly. Data on the natural history of 2008 WHO-ECMP defined normocellular ET, prodromal PV and ET.MGM as derived from large scale prospective studies are lacking.
Clinical diagnosis of ET and PV can be made by the combined use of complete blood cell counts, peripheral blood and bone marrow smears and serum EPO levels in patients carrying JAKv617F mutation without the need of bone marrow biopsy (BMB) and red cell mass RCM) measurement. BMB does not differentiate between ET and PV whereas RCM is the gold standard to differentiate between ET and PV. BMB combined with complete blood cell counts, serum EPO levels, is highly specific and sensitive to distinguish 3 phenotypes of ET from early and overt stage PV carrying the JAK2 mutation without the need of RCM measurement.