Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2015) Volume 3, Issue 3
Background: Egg precursor cells can be readily isolated from the protective outer lining of the ovarian cortex. Studies have demonstrated that mitochondria isolated from these cells are of high quality. The AUGMENTSM treatment is a proprietary new technology based on previous clinical use demonstrating that the addition of mitochondria during in vitro fertilization (IVF) is safe, improves embryo quality, and increases the success of IVF. Subsequently published animal studies also confirmed the role of mitochondria in improved outcomes. This report represents the earliest global observations of the AUGMENTSM treatment in routine clinical practice from two distinct international centers.
Methods and results: The AUGMENTSM treatment was initially used in a population of difficult-to-treat patients with a poor prognosis for success with standard IVF who were likely moving to donor egg as a next step. Each group reported marked improvements in pregnancy rates above the historic IVF success rate for these patients (e.g., 11- and 18- fold increase in ongoing clinical pregnancy rates in the UAE and Canada, respectively). In a 25 patient subset, retrieved eggs from each woman were allocated to two treatment groups; one group underwent the AUGMENTSM treatment at the time of ICSI while the other group underwent conventional ICSI. Embryos were selected for fresh-embryo transfer based on standard criteria including embryo morphology and the results of preimplantation genetic testing. Morphogenetic embryo selection and transfer from the AUGMENTSM treatment group was significantly higher, suggesting that improved embryo quality may have resulted in the improved pregnancy rates observed in these women.
Conclusions: Based on these findings, the AUGMENTSM treatment may be a viable treatment option to address an unmet need for women with poor reproductive histories, history of poor egg quality, poor embryo development, previously failed IVF, and those seeking—despite repeated failures-to conceive genetically-related offspring.
<Keywords: Infertility; IVF; ICSI; Egg precursor cells; Mitochondria; AUGMENT treatment
Infertility treatment prior to 1978 proved challenging to both patients and their physicians. The birth of Louise Brown through in vitro fertilization (IVF) was the result of decades-long research in both the basic and clinical sciences and followed hundreds of failed attempts at human IVF [1]. With IVF’s successful introduction, related and supportive technologies soon emerged including IVF and the use of donor eggs, cryopreservation and frozen embryo transfer (FET), gamete intra-fallopian transfer (GIFT), zygote intra-fallopian transfer (ZIFT), intra-cytoplasmic sperm injection (ICSI) and less invasive procedures aided by enhancements in equipment, such as transvaginal ultrasound guided oocyte retrieval. It may be hard to recall now that technologies such as IVF, the use of donor eggs, and ICSI were, at first, controversial but so successful in improving outcomes that they were most often adopted into clinical practice without any demonstrated benefit in randomized controlled clinical trials [2].
Despite the technical enhancements introduced over time that have resulted in unprecedented cumulative IVF pregnancy rates, a significant percentage of women continue to fail repeated attempts at IVF. While cumulative pregnancy rates increase with increasing cycle number (approximately 75% of women will achieve a live birth by the sixth IVF cycle), per cycle IVF success rates tend to decrease with increasing cycle number. The age blended probability of a live birth is approximately 25% in a woman’s first cycle (range [9-33%]), 20% per cycle during her second and third cycles and decreases to less than 20% per cycle during cycles four through six [3]. IVF success rates drop dramatically as women age. Therefore, a patient population exists that will fail to respond to all lines of treatment, including repeated cycles of IVF. For this patient population, IVF using a donor egg or adoption have, until recently, represented the only remaining option(s) [4].
The causes of repeated IVF failure are often complex and poorly understood. In contrast, the decrease in fertility observed in women with increasing maternal age has been attributed to a decline in egg and embryo quality as well as increased rates of aneuploidy [5]. Other causes of poor egg/embryo quality beyond age-related factors include medical conditions such as type II diabetes, obesity, polycystic ovary syndrome (PCOS), as well as other genetic and environmental factors [6,7]. Over the past 25 years, an increasing body of clinical and preclinical data has demonstrated that the decline in egg quality is largely due to a reduction in energy production [8-11]. In the 1990s, there were attempts at improving egg and embryo quality by injecting cytoplasm from young, healthy, donor eggs into the eggs of women with a history of reproductive failures [12-14]. The cytoplasm injection procedure involved the injection of third-party mitochondria obtained from younger donor eggs and resulted in the birth of approximately 50 seemingly healthy babies [12-14]. This groundbreaking work was not pursued as more study was required [11].
In 2004, an autologous source of germline mitochondria was discovered [15]. These mitochondria were found in egg precursor cells that resided in the protective, avascular outer lining of the ovarian cortex [15,16]. Egg precursor cells can be readily isolated from ovarian cortical tissue of reproductive-age women through the use of antibodies specific to the human VASA analogue, a cell surface protein found on human egg precursor cells [16]. Studies have demonstrated that mitochondria isolated from egg precursor cells are of high quality and can therefore serve as an autologous source of mitochondria for women [17].
The AUGMENT treatment is a proprietary new technology. Egg precursor cells of women are isolated, mitochondria from those precursor cells are extracted, and these autologous mitochondria are injected into the patient’s own oocyte at the time of ICSI. The support and use of the AUGMENT treatment is based upon case reports of clinical success using human donor egg cytoplasm injection as well as multiple published animal studies that have demonstrated that the addition of mitochondria during IVF treatment is safe, improves the quality of the embryos, and increases the success of IVF [18].
The current report summarizes the initial global patient experience with the AUGMENT treatment and describes the clinical effectiveness observed in a subset of AUGMENT-treated patients who have consented to participate in the OvaScience Global Registry.
Centers and patients
Two global centers agreed to report their experience using the AUGMENT treatment. These included TCART Fertility Partners of Toronto, ON, Canada and FAKIH IVF, Dubai, UAE. Written informed consent was obtained at both centers from all patients and their partners (when applicable).
Ovarian stimulation and oocyte collection
The menstrual cycles of patients were stimulated using recombinant FSH (Gonal-F®, Merck Serono, Mississauga, ON, Puregon, Merck, Kirkland, QC) and HMG (Menopur®, Ferring Pharmaceutical, York Mills, ON) according to standard gonadotropin releasing hormone (GnRH) antagonist (Ganerelix, Merck or Cetrotide, EMD-Serono) stimulation protocols and starting on day 3 of the menstrual cycle until at least three follicles reached ~20 mm in diameter. The oocyte pickup was performed by vaginal ultrasound 36 h after the subcutaneous injection of human chorionic gonadotropin, hCG (Pregnyl®, Merck). The oocyte retrieval was performed under local anesthesia and with the patient receiving intravenous sedation with fentanyl (Jannsen, Don Mills, ON) 50 to 100 mcg and midazolam (Sandoz, Boucherville, QC) 1-2 mg. During the follicular aspiration procedure, the oocytes were recovered in Global®-HEPES-buffered medium (IV Fonline, Canada) supplemented with 10% vol/vol Serum Substitute Supplement (SSS; Irvine Scientific, USA). The luteal phase was supported by vaginal progesterone suppositories (Kingsway Pharmacy, Toronto, ON) 200 mg twice daily until the day of the pregnancy test or until 10 weeks of gestation.
Egg precursor cell mitochondrial isolation and preparation
Previously cryopreserved autologous ovarian cortical tissue was thawed based on method of cryopreservation. The tissue was placed in an enzymatic solution and physically dissociated to a single cell suspension. The single cell suspension was incubated with a monoclonal anti-VASA antibody. Labeled cells were then isolated by fluorescence-activated cell sorting (FACS). Standard slow rate cooling cryopreservation procedure for freezing each patient batch of egg precursor cells was performed. On the day of ICSI the cryopreserved egg precursor cells were thawed and mitochondria were isolated by differential centrifugation and maintained in standard respiration buffer.
Details related to the number of egg precursor cells isolated and the number of mitochondria microinjected are proprietary. In general terms, the number of egg precursor cells obtained per patient falls within a consistent range unless the quality of the biopsy and of freezing is compromised. The number of mitochondria microinjected is based on previous reports of the cytoplasmic volume microinjected during human ooplasmic transplantations and an estimate of mitochondrial quantity within this volume [12,18-20]. More than enough mitochondria are isolated from egg precursor cells during this process to supply all retrieved oocytes per patient
ICSI, AUGMENT, and cell culture
Clinic standard procedures were followed for oocyte retrieval and oocytes were prepared for ICSI as the method of insemination. After retrieval, cumulus-oocyte complexes were manually trimmed of excess cumulus cells and group cultured in ~1.0 mL Global®-HTF medium (IVF online, Canada) plus 10% SSS (Irvine Scientific, USA) under oil at 37°C and an atmosphere containing 5.5% CO2 before the ICSI procedure. In every patient, all oocytes in metaphase II were injected 5 hours after aspiration. At the time of ICSI, the mitochondrial solution was concentrated into a ~250 nl droplet on the ICSI plate. The autologous mitochondrial solution was aspirated into the ICSI pipette along with a selected sperm and approximately 1-2 pL was injected and delivered to the MII oocyte during ICSI. After ICSI AUGMENT procedure (Day 0), all injected oocytes were cultured individually in 20 μL droplets of Global® media (IVF online, Canada) supplemented with 10% vol/vol LGPS under mineral oil at 37°C in an atmosphere of 6% CO2.
The fertilization was evaluated 16-18 hours post injection by the presence of two pronuclei (Day 1). Zygotes were continuously cultured to Day 6 with neither medium refreshment nor exchange.
Embryo selection and embryo transfer
Standard clinic selection criteria including morphology, morphokinetic analysis (TCART and FAKIH IVF) and pre-implantation genetic testing (FAKIH IVF only) were utilized in selecting the embryos with the best implantation potential. Morphology evaluations and assessments were consistent with the Society for Assisted Reproductive Technology’s (SART) criteria (see supplement). Using clinic standard culture procedures, embryos were cultured to blastocyst stage for embryo transfer selection unless there were selectivity or patient scheduling limitations.
Pregnancy determinations
Patients were monitored post transfer for a rise in human chorionic gonadotropin beta subunit (bHCG) to detect pregnancy. Biochemical pregnancy was assessed approximately 12 days after the embryo transfer by measuring the (bHCG) in blood. Clinical pregnancy was determined by transvaginal ultrasonography to detect gestational sacs and fetal heartbeats at approximately 21 and 28 days after transfer, and patient care was then referred to an obstetrician.
MBEST at FAKIH IVF
At FAKIH IVF, eggs from a subset of women who underwent successful egg retrieval were allocated to two treatment groups; one group of a patient’s eggs underwent the AUGMENT treatment at the time of ICSI while the other group of that woman’s eggs underwent conventional ICSI only. The eggs and embryos obtained from both the AUGMENT group and ICSI-only group were maintained under identical culture, environmental, and embryo management conditions. Morphokinetic analysis was performed using the EmbryScope® (VitroLife, formerly Fertilitech) and standard morphology metrics were observed along with the timing of cellular developments from post AUGMENT injection until the time of embryo selection. Embryos were selected from one of these two treatment groups based on standard laboratory, prognostic criteria including embryo morphology and the results of pre-implantation genetic testing. Embryo transfer for a given patient was not performed if none of the embryos from either treatment group met these criteria for transfer. To facilitate further discussion, we have termed this approach Matched, Best Embryo Selection and Transfer (MBEST).
Analyses
All data was prospectively collected and reported by the physicians of each clinical site. Statistical analyses were performed on the reported data using Microsoft Excel 2013 and SAS 9.3.
Descriptive statistics were computed for the data sets submitted by each participating center. Data summaries are presented as mean, range, and percentages. The clinical pregnancy rate per cycle initiated was calculated by dividing the total number of patients identified with at least one documented gestational sac by the total number of cycles initiated. The clinical pregnancy rate per embryo transfer was calculated by dividing the total number of patients with at least one documented gestational sac by the total number of embryo transfers performed. Ongoing clinical pregnancy rates per cycle initiated and per embryo transfer were similarly calculated except the numerator applied was the total number of patients with at least one documented fetal heartbeat and at least 12 weeks of gestation. Included in this latter group were several women whose pregnancies resulted in a live birth.
To determine the effectiveness of the AUGMENT treatment, a subgroup of patients who underwent MBEST was first identified. To identify patients who underwent MBEST, a search was performed of patients who had consented to participate in the OvaScience Global Registry. Patients were included for analysis if they had a documented history of ≥ 1 failed IVF cycle, if their retrieved eggs were allocated to the two aforementioned treatment groups, if embryo selection was based on morphogenetic criteria, and if fresh embryo transfer for a given patient was limited to embryos from only one treatment group or no transfer was performed due to poor embryo quality or aneuploidy.
Intent-to- treat (ITT) analysis was performed on the two MBEST treatment groups. Specifically, ITT analyses was undertaken of embryo transfer, pregnancy, and clinical pregnancy rates (per embryo transfer and per initiated cycle), and ongoing clinical pregnancy rates (per embryo transfer and per initiated cycle). In addition, analyses of fertilization rates and the rate of 5-day blastocyst formation from two-pronuclear (2PN) zygotes were performed for both treatment groups. The fertilization rate was calculated as the number of ICSIderived 2PN zygotes divided by the number of oocytes injected. The rate of formation of 5-day blastocysts derived from 2PN zygotes was calculated by dividing the number of 5-day blastocysts formed by the number of 2PN zygotes.
To further assess the effectiveness of the AUGMENT treatment in the MBEST treatment group, the ongoing clinical pregnancy rate per cycle initiated with the AUGMENT treatment was compared to the group’s historical IVF live-birth rate per cycle initiated (number of live births/number of prior IVF cycles initiated).
Tests for statistical significance were performed using either the two-tailed Fisher’s Exact Test or the paired t-test, as appropriate.
The results reported here are based on the observations of 93 patients managed in AUGMENT treatment centers in Canada (TCART; n = 34) and the UAE (FAKIH IVF; n = 59), as summarized in Tables 1-4. There were differences in background diagnoses and number of prior IVF cycles among the patients treated in these centers. Prior to the AUGMENT treatment, the 93 patients underwent 328 IVF cycles, collectively. The pregnancy outcomes of the 328 cycles were poor for patients in both centers and ranged from 4% - 11% clinical pregnancy rate per IVF cycle initiated and 1.4% - 2% ongoing pregnancy rate per IVF cycle initiated. Following the AUGMENT treatment, both groups observed marked improvements in pregnancy rates above these historic IVF success rates with a 3- and 6- fold increase in clinical pregnancy rate per initiated cycle observed in Canada and the UAE, respectively, and an 11- and 18- fold increase in ongoing clinical pregnancy rates per initiated cycle observed in the UAE and Canada, respectively.
| AUGMENT TREATMENT CENTERS | ||
|---|---|---|
| TCART | FAKIH IVF | |
| PATIENT HISTORY | ||
| Number of patients | 34 | 59 |
| Average current age | 36.0 (Range: 26-44) | 37.3 (Range: 20-48) |
| Background/Diagnoses | Poor oocyte and embryo quality with one of the following diagnoses: Diminished Ovarian Reserve, Ovulatory Dysfunction, Polycystic Ovarian Syndrome, Tubal Factor, Endometriosis, Unexplained |
Poor oocyte and embryo quality: Diminished Ovarian Reserve, Ovulatory Dysfunction, Severe Male Factor |
| PRIOR IVF HISTORY | ||
| Total previous IVF cycles initiated | 71 | 257 |
| Average cycles per patient | 2 (Range: 1-5) | 4.3 (Range: 1-16) |
| Total previous embryo transfers | 79 | Unknown due to international patient base |
| Historical clinical pregnancy rate: • per cycle initiated • per embryo transfer |
8/71 (11%) 8/79 (10%) |
9/257 (4%) |
| Historical live birth rate: • per cycle initiated • per embryo transfer |
1/71 (1.4%) 1/79 (1.3%) |
4/257 (2%) |
Table 1: Patient characteristics across the select AUGMENT treatment centers.
| THE AUGMENT EXPERIENCE | ||
|---|---|---|
| TCART | FAKIH IVF | |
| Total AUGMENT cycles initiated | 34 | 60 |
| Average cycles per patient | 1 | 1 |
| Total embryo transfers | 26 | 34 |
| Clinical pregnancy rate: • per cycle initiated • per embryo transfer |
12/34 (35%) 12/26 (46% ) |
13/60 (22%) 13/34 (38%) |
| Ongoing clinical pregnancy and live birth rate: • per cycle initiated • per embryo transfer |
9/34 (26%)* 9/26 (35%)* |
11/60 (18%)** 11/34 (32%)** |
*includes 1 live birth
**includes 2 live births (two sets of twins)
Note: All on-going clinical pregnancies reported here were continuously on-going pregnancies at the time of publication submission
Table 2: Summary of center specific AUGMENT treatment experiences.
| Patient History | Previous Clinical Pregnancy Rate per Initiated Cycle | Clinical Pregnancy Rate per Initiated AUGMENT Cycle | Clinical Pregnancy Rate per AUGMENT Embryo Transfer | Previous Ongoing Clinical Pregnancy Rate/Live Birth Rate per Initiated Cycle | Ongoing Clinical Pregnancy Rate/Live Birth Rate per Initiated AUGMENT Cycle | Ongoing Clinical Pregnancy/ Live Birth Rate per AUGMENT Embryo Transfer |
|
|---|---|---|---|---|---|---|---|
| Canada | • Average age: 36.0 • 1-5 prior IVF cycles |
11% | 35%* | 46%* | 1.4% | 26% | 35% |
| United Arab Emirates | • Average age: 37.3 • 1-16 prior IVF cycles |
4% | 22% | 38% | 2.0% | 18% | 32% |
*9 patients with 23 embryos cryopreserved for future use
Table 3: Center-specific clinical and ongoing clinical pregnancy rates.
| TCART | FAKIH IVF | |||||||
|---|---|---|---|---|---|---|---|---|
| Age (years) |
# of Patients | # bHCG + | # Clinical Pregnancies | # Ongoing Clinical Pregnancies | # of Patients | # bHCG + | # Clinical Pregnancies | # Ongoing Clinical Pregnancies |
| 20-30 | 5 | 3* | 3* | 2* | 5 | 3 | 2 | 2 |
| 31-35 | 10 | 7* | 6* | 6* | 12 | 3 | 3 | 3 |
| 36-40 | 14 | 5 | 3 | 1 | 28 | 7 | 7 | 5 |
| 41-45 | 5 | - | - | - | 10 | 2 | 1 | 1 |
| 46-48 | - | - | - | - | 4 | - | - | - |
| Totals | 34 | 15 | 12 | 9 | 59 | 15 | 13 | 11 |
*Includes one pregnancy each from a subsequent frozen embryo transfer
Table 4: Age related outcomes by center.
As noted in Table 5, the baseline characteristics of the 25 patients comprising the MBEST subgroup were similar to the entire FAKIH IVF patient group. There were significantly more oocytes allocated to the AUGMENT treatment than to the ICSI-only group. Between the two treatment groups, there was no difference in the rate of 2PN and 5-day blastocyst formation. However, embryo transfer rates were significantly higher in the AUGMENT treatment group than in the ICSI-only group. When adjusting for the higher number of oocytes allocated to the AUGMENT treatment group, the higher rate of morphogenetic embryo selection and transfer observed with the AUGMENT treatment remained statistically significant (Fisher’s Exact Test; p = 0.0334) suggesting that the significant difference observed in embryo selection and transfer was not due to the differences in number of oocytes initially allocated but rather due to selection based on embryo quality. The higher rates of chemical, clinical, and ongoing clinical pregnancy rates observed with the AUGMENT treatment (n = 8) were higher than with ICSI-only treatment (n = 0) (Figure 1). This too remained statistically significant when adjusting for differences in oocyte allocation (Fisher’s Exact Test; p = 0.025). When comparing clinical and ongoing clinical pregnancy rates per cycle initiated to the patients’ previous history, a marked increase was observed with the AUGMENT treatment (32% vs. 0%).
| Baseline Characteristics | Total | Mean | Median | Range | |||
|---|---|---|---|---|---|---|---|
| Age | 36.16 | 36 | 28 to 48 | ||||
| Previous # Cycles | 102 | 4.00 | 2 | 1 to 12 | |||
| Previous Clinical Pregnancies | 4 | 0.16 | 0 | 0 to 2 | |||
| Previous Live Pregnancies | 0 | 0 | |||||
| Total Eggs Retrieved | 351 | 14.04 | 12 | 6 to 31 | |||
| Embryology | Treatment Groups | ||||||
| ICSI-only | AUGMENT | ||||||
| Eggs->ICSI | 106 | 171 | <0.0001* | ||||
| 2PN (2PN/ICSI) | 67 (63.21) | 118 (69.01) | 0.3588 | ||||
| 5-Day Blasts (5-D BL/2PN) | 20 (29.85) | 41 (34.75) | 0.3717 | ||||
| Embryo Transfers (of 25) | 2 | 14 | 0.0334 | ||||
| Fisher’s Exact Test has been used to determine all the p-values except otherwise noted. *The paired t-test has been used to determine the p-values. |
|||||||
| Embryo assessment* and embryo transfer by treatment groups based on morphogenetic criteria | |||||||
| Embryo Transfer | ICSI-Only Treatment | AUGMENT Treatment | |||||
| + | 2 | 14 | |||||
| - | 23** | 11** | |||||
| Total | 2 of 25 | 14 of 25 | |||||
| *SART Criteria **In nine patients, embryos from both treatment groups failed to meet the morphogenetic criteria for embryo transfer |
|||||||
Table 5: Baseline patient characteristics, embryology, morphogentic embryo assessment and embryo transfer of the MBEST Patient Group (n = 25).
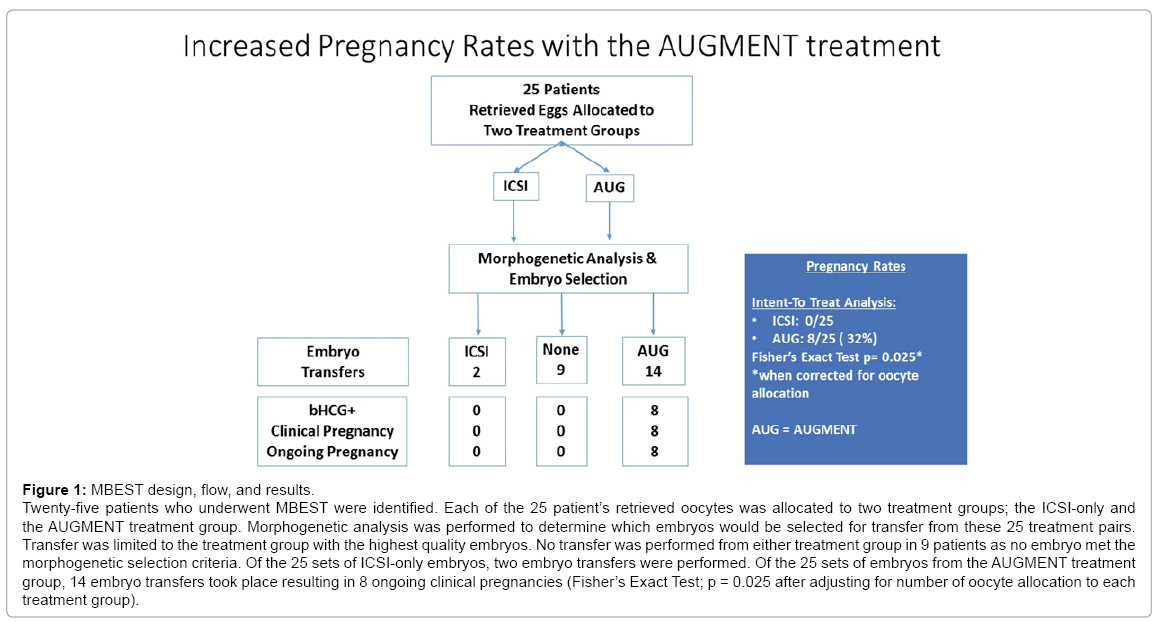
Figure 1: MBEST design, flow, and results.
Twenty-five patients who underwent MBEST were identified. Each of the 25 patient’s retrieved oocytes was allocated to two treatment groups; the ICSI-only and the AUGMENT treatment group. Morphogenetic analysis was performed to determine which embryos would be selected for transfer from these 25 treatment pairs. Transfer was limited to the treatment group with the highest quality embryos. No transfer was performed from either treatment group in 9 patients as no embryo met the morphogenetic selection criteria. Of the 25 sets of ICSI-only embryos, two embryo transfers were performed. Of the 25 sets of embryos from the AUGMENT treatment group, 14 embryo transfers took place resulting in 8 ongoing clinical pregnancies (Fisher’s Exact Test; p = 0.025 after adjusting for number of oocyte allocation to each treatment group).
This report represents the earliest global observation of the AUGMENT treatment in routine clinical practice. Both centers reported marked improvement in pregnancy rates above the historic IVF success rate for these patients (e.g., a 3- and 6- fold increase in clinical pregnancy rates in Canada and the UAE, respectively; and an 11- and 18- fold increase in ongoing clinical pregnancy rates in the UAE and Canada, respectively). It is notable that this early clinical experience with the AUGMENT treatment was evaluated in a particularly difficult-to-treat patient population with a poor prognosis for success with standard IVF who were likely moving to donor egg as a next step. This suggests that the AUGMENT treatment may result in improved pregnancy rates among women with a poor reproductive history and previously failed IVF. The consistent and improved outcomes above the patients’ own historic rates as observed across the two centers are impressive given the lower per cycle success rates as cycle number and maternal age increase, and given the varied clinical and laboratory practices seen across countries and centers, as well as the different risk groups treated by these distinct clinical programs. As embryo cryopreservation was permissible in one center (TCART Fertility Partners), the potential for even greater pregnancy outcomes is feasible for that center where 9 patients have 23 embryos cryopreserved for future use.
There are several limitations to these findings. The two-center clinical observations are limited by the absence of a standard control group, though this is not unusual in a field where technologies have evolved and succeeded in the absence of randomized control trials for the most part, and where excessive repeated exposure to a failed intervention may be deemed unethical. Furthermore, patients may not volunteer for studies if they might be randomized into standard treatments that have previously failed them. Given these challenges, the use of matched historical controls may seem appealing. However, matching can prove challenging given the disparate biologic and medical complexity (both known and unknown) associated with individuals’ poor reproductive performance and given the wide variability in laboratory and clinical practice worldwide. A way to mitigate such concerns is the MBEST approach taken at FAKIH IVF.
To help evaluate the AUGMENT treatment in a controlled manner, the MBEST approach was undertaken as this allowed for the control, across two treatments, of known and unknown variables including the patient’s own biology, the environment, clinical practices, and laboratory procedures. The MBEST design is unique in that it applies a practical, real world approach to embryo selection and transfer, using accepted laboratory and clinical standards in the selection and transfer of embryos most likely to result in a live birth. The MBEST approach is also unique in being similar to an approach used in adaptive clinical trials, whereby treatments deemed futile are excluded and superior interventions are employed to better serve patients.
The MBEST results indicate that morphogenetic embryo selection and transfer from the AUGMENT treatment group was significantly higher than the ICSI–only group, suggesting that improved embryo quality may have resulted in the observed improved pregnancy rates among this group of women with poor reproductive histories and previously failed IVF cycles.
That the MBEST approach overwhelmingly resulted in the selection and transfer of embryos derived from the AUGMENT treatment group and that over 50% of such transfers resulted in ongoing clinical pregnancies appears to suggest improved egg and embryo quality that resulted from the AUGMENT treatment among patients with historically poor IVF performance (0% live birth rate). These observations are consistent with the finding of prior heteroplasmic mitochondrial injection reports lending further credence to the role of mitochondria in egg and embryo health.
There are several limitations to the MBEST observations. The number of eggs allocated for insemination in the AUGMENT treatment group was 1.7- fold higher than the number of eggs allocated for insemination in the ICSI-only group. For women who produced a low number of mature eggs in response to controlled ovarian hyper stimulation, it was deemed unethical to allocate her limited eggs evenly between the two groups, given their poor history of IVF success with ICSI alone. The significant increase in the number of eggs that received the AUGMENT treatment could have had a downstream effect and impacted embryo transfer and pregnancy rates. However, statistical testing took this imbalance into account and indicates that the statistically significant differences observed in embryo selection, embryo transfer, and pregnancy outcomes was not impacted by the higher egg allocation into the AUGMENT treatment group. Another potential bias is that embryologists were not blinded to the identity of the two treatment groups when selecting embryos for transfer and this too could have biased these observations. However, the lack of blinding in embryo selection does not account for the markedly improved pregnancy rates when compared to the patients’ historical performance. Nevertheless, we recognize this shortcoming and future approaches to minimize such potential bias could include the blinding of embryologists to the identity of the treatment groups or blinded assessments by an independent group of embryologists to confirm that un-blinded scoring has not inadvertently introduced such a bias. Despite these limitations, the MBEST adaptive design offers a controlled, ethical, pragmatic, and real-world clinical and laboratory alternative to randomized control trials in the evaluation of treatment effectiveness among patients who have failed standard therapies. Adaptive designs are acceptable as an ethical alternative to randomized control trials using an ineffective comparator. The MBEST approach has the added advantage of possibly offering a superior biologic, medical, clinical, and laboratory “control” setting when evaluating efficacy or effectiveness as almost all variables except the intervention under study are exactly matched.
The AUGMENT treatment represents the latest major innovation in assisted reproductive technologies and may help address an unmet need for women with consistently poor reproductive histories, poor ovarian response, previously failed IVF, and those seeking, despite repeated failure, to conceive their own genetic child. As this represents the earliest report of the AUGMENT treatment, technologic and methodologic optimization, procedural refinements, additional clinical experience and registry data capture and analyses, should all aid in adding to our understanding of the role that mitochondria can play in addressing infertility and may help further improve outcomes associated with this promising, new technology.
We would like to acknowledge the tireless support and dedication of the following individuals whose contributions toward this work have been invaluable: Navid Esfandiari DVM, PhD, Daniel Nayot MD, Yaakov Bentov MD, Paul Chang MD, Marjorie Dixon MD, Fay Weisberg MD, Deborah Meyers M.Mgt, CCPE and Sarah Catherine Lyndon, RN
Robert Casper MD is a member of the following Scientific Advisory Boards: OvaScience, Abbvie, Actavis/Allergan, Bayer, Ferring, Merck, EMD-Serono. He has stock ownership in OvaScience, Insception/Lifebank, Circadian-Zirclight and serves as Medical Director, TCART Fertility Partners, Insception/Lifebank. Colleen Burgess ELD (ABB) and Gabriel M Cohn, MD are both OvaScience employees.