Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2013) Volume 3, Issue 2
Vascularized pancreas transplantation was initially developed as a means to re-establish endogenous insulin secretion responsive to normal feedback controls and has evolved over time to a form of auto-regulating total pancreatic endocrine replacement therapy that reliably achieves a euglycemic state and normal glucose homeostasis without the need for either exogenous insulin therapy or close glucose monitoring.
<Keywords: Pancreas transplantation; Organ retrieval; Segmental pancreatic grafts
As of December 2010, more than 35,000 pancreas transplants were reported to the International Pancreas Transplant Registry and nearly 9,000 to the Collaborative Transplant Study databases [1,2]. Pancreas transplantation in diabetic patients is divided into 3 major categories; those performed simultaneously with a kidney (SPK) transplant, usually from a deceased donor; those performed after a successful kidney (PAK) transplant in which the kidney came from either a living or deceased donor; and pancreas transplantation alone (PTA) in the complete absence of a kidney transplant. The latter 2 (PAK and PTA) categories are usually combined together as solitary pancreas transplants. The total number of pancreas transplants steadily increased until 2004 but has since declined, particularly in the PAK category [1,3]. In the last decade, era analyses have demonstrated that deceased donor recovery rates and additions to the waiting list have decreased; discard rates and waiting times have increased; and the proportion of recipients who are older, black, have a higher body mass index, or are characterized as having type 2 diabetes have all increased [1,3]. The majority (75%) of pancreas transplants are performed as SPK transplants whereas approximately 16% are performed as PAK and 9% as PTA transplants, respectively [1,3].
With improvements in organ retrieval and preservation technology, refinements in diagnostic and therapeutic technologies, advances in clinical immunosuppression and antimicrobial prophylaxis, and increased experience in donor and recipient selection, success rates for pancreas transplantation have steadily improved [1,3]. For recipients of primary deceased donor pancreas transplants, one-year patient survival is more than 95% in all 3 categories; unadjusted fiveyear patient survival rates are 87% in SPK, 83% in PAK, and 89% in PTA recipients; and more than 70% of patients are alive at ten years post-transplant [1,3]. One-year pancreas graft survival (insulin-free) rates are 85.5% in SPK (93% kidney graft survival), 80% in PAK, and 78% in PTA recipients, which translates to pancreas graft halflives approaching 14 years in SPK and 10 years in solitary pancreas transplant recipients [1,3].
The history of pancreas transplantation has been largely defined by the evolution in surgical techniques. Segmental pancreatic grafts were predominant in the late 1970s and early 1980s until techniques were worked out to safely manage the exocrine secretions [4]. Since this time, the vast majority of pancreas transplants are performed as whole organ grafts with a variable length of donor duodenum. Currently, segmental pancreas grafts are rarely obtained from deceased donors while they remain the only technical possibility in pancreas transplantation from living donors [4,5]. According to Registry data, most whole organ pancreas transplants are performed with systemic venous delivery of insulin and either bladder (systemic-bladder) or enteric (systemicenteric) drainage of the exocrine secretions [1]. Prior to 1995, more than 90% of pancreas transplants were performed by the standard technique of systemic-bladder drainage, usually using a duodenal segment conduit for exocrine drainage. Since 1995, the number of pancreas transplants performed with primary enteric exocrine drainage has increased dramatically and currently accounts for 91% of SPK, 89% of PAK, and 85% of PTA cases [1]. Over 80% of enteric drained pancreas transplants are performed with systemic (iliac or vena cava) venous delivery of insulin, resulting in peripheral hyperinsulinemia [1]. In the non-transplant setting, chronic hyperinsulinemia has been associated with insulin resistance, dyslipidemia, accelerated atherosclerosis, and macroangiopathy. To improve the physiology of pancreas transplantation, a surgical technique of intraperitoneal portal venous drainage using the superior mesenteric vein (SMV) was developed by Gaber et al and subsequently refined to a “retroperitoneal” approach by Boggi et al combining portal venous delivery of insulin with enteric drainage of the exocrine secretions (portal-enteric technique) [6,7]. However, the potential of portal-enteric drainage has never been fully realized as it currently accounts for only 18% of SPK and PAK and 10% of PTA transplants [1]. A number of studies have demonstrated no major or consistent differences in outcomes for bladder-drained or enteric-drained pancreas transplants with either portal or systemic venous drainage [8-13]. Although nearly all pancreas transplants are currently performed with one of the three above techniques, current philosophy dictates that the most appropriate technique to be performed is the one with which the individual surgeon feels most comfortable. The remaining focus of this overview will be on the technical aspects of whole organ pancreatico-duodenal transplantation with portal venous and enteric exocrine drainage.
Although bladder, renal pelvic, and ureteral drainage of the exocrine secretions of the pancreas are technically feasible concomitant with portal venous drainage [14,15], nearly all pancreas transplants with portal venous drainage are performed in conjunction with enteric drainage of the exocrine secretions (portal-enteric technique). In addition, although techniques of portal venous drainage have been described using either the recipient splenic vein [15-17], inferior mesenteric vein [18], or portal vein directly [14], “portal venous” drainage almost always implies use of the recipient’s SMV for venous drainage of the pancreas allograft with the head of the pancreas directed cephalad and the body and tail directed caudad in the recipient.
Most pancreas transplants are performed through a vertical midline abdominal incision, which preserves all possible options for transplantation of the pancreas as well as simultaneous placement of a kidney through the same incision when applicable. In general, midline incisions are associated with fewer wound infections although the key concepts are taking advantage of the intraperitoneal lymphatic circulation and permeability for internal absorption of peri-pancreatic secretions in conjunction with preventing proximity between the healing wound and the reperfused pancreas [19]. In the absence of a kidney transplant, the incision may extend from the mid-epigastrium to 2-3 cm above the symphysis pubis; with a simultaneous kidney transplant the incision should extend to the symphysis pubis for better pelvic exposure. When the pancreas is placed in the pelvis, the right side is preferred because of the favorable disposition of the right iliac vessels. In SPK transplantation, the kidney can either be placed contralateral to the pancreas in the left iliac fossa or ipsilateral but distal on the right side using the external iliac vessels [20]. With either technique, revascularization of the pancreas first is recommended because of constraints of cold ischemia. Unlike other methods of pancreas transplantation, however, the portal-enteric technique is a mid-abdominal rather than a pelvic procedure. For this reason, it tends to make the venous and enteric anastomoses “easier” because the pancreas is positioned more cephalad and anterior in the abdominal midline. However, the arterial anastomosis and exposure may be more challenging because of the need for a long “Y” graft that traverses through the distal ileal mesentery.
The procedure can also be performed through a transverse abdominal [19,21] or J-shaped iliac incision; with the latter it is recommended that if an extraperitoneal approach is taken, then a peritoneal window be created after the vascular anastomoses for performance of the bowel anastomosis and to facilitate absorption of potential leaks and peri-graft fluid collections. An alternative or hybrid technique involves a midline intraperitoneal approach followed by access to the SMV through the right retrocolic region (Figure 1) [7]. Potential advantages of this “retroperitoneal” portal-enteric technique are good graft fixation in the right paracolic space, improved accessibility for ultrasonographic imaging and percutaneous biopsy, and use of a short interposition arterial graft. However, only a minority of portal-enteric pancreas transplants are performed using this novel technique.
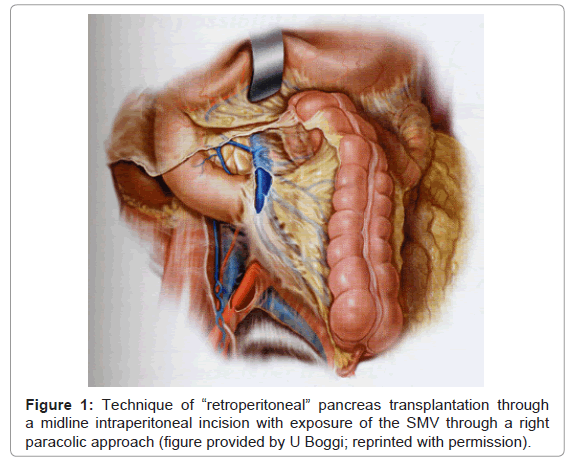
Figure 1: Technique of “retroperitoneal” pancreas transplantation through a midline intraperitoneal incision with exposure of the SMV through a right paracolic approach (figure provided by U Boggi; reprinted with permission).
Following an initial time-out and incision, a formal abdominal exploration is performed, a nasogastric tube is positioned in the gastric antrum, and we document position of the urethral catheter balloon in the bladder. We typically use a first-generation cephalosporin for surgical site prophylaxis, with doses repeated every 3 hours intra-operatively and two additional doses administered at 8-hour intervals post-operatively. Pre-operative enemas are given but no formal bowel preparation is performed. Although we have used the standard midline intraperitoneal anterior approach to the SMV for the past 15 years, in approximately 10% of cases we switch to an alternative technique based on recipient (or rarely donor) anatomy and intra-operative findings. For example, if the recipient has sclerosing encapsulating peritonitis or severe adhesions from multiple previous laparotomies, then an enteric anastomosis may not be safe [11]. However, we make every attempt to perform a complete enterolysis and carefully define the visceral anatomy prior to any vascular dissection. We no longer perform an “incidental cholecystectomy” if gallstones are identified unless there is evidence for acute or chronic cholecystitis. If a Meckel’s diverticulum is noted, we may elect to resect this lesion and perform the enteric anastomosis at this site [22]. An “incidental appendectomy” is not performed unless the appendix is clearly abnormal. If a gastrointestinal or other tumor is discovered, a localized resection and frozen section examination is performed prior to proceeding with the transplant.
Other “contraindications” to portal venous drainage include a small SMV (<6 mm in diameter); a deep, buried SMV (usually associated with central obesity, particularly in recipients with a BMI >30 kg/m2), a sclerotic or partially thrombosed SMV or history of venous thrombosis from a previous pancreas transplant with portal venous outflow, portal hypertension, an SMV that lies deep to the SMA and is not easily accessible, or an arterial “Y” graft that will not reach the iliac artery or aorta. For example, there may be concentric hard calcification of the distal aorta and common iliac arteries that precludes use of these vessels for arterializations of the pancreas. If the arterial “Y” graft cannot safely reach the external iliac artery (or a soft spot on the common iliac artery), then one may need to convert to systemic venous drainage [12]. In obese or large patients (usually males over 6 feet tall and weighing more than 90 kg) or patients with a thickened mesentery, on occasion the arterial “Y” graft may be too short even with the use of a distal external iliac artery extension graft anastomosed to the donor common iliac artery conduit to safely accommodate portal venous drainage.
For these reasons, after the initial abdominal exploration and enterolysis (when indicated) are completed, a careful assessment of the quality and anatomy of the SMV and (usually) right common iliac artery is next performed. The transverse mesocolon is placed on cephalad traction using rolled laparotomy sponges and a self-retaining retractor system; the remaining viscera are retracted using laparotomy sponges to expose the base of the transverse mesocolon. The native duodenum is identified and preserved. In most cases, the SMV can be visualized through the flattened out mesentery between the duodenum and SMA, which is identified by palpation. Alternatively, the SMV may be found just to the right of the SMA. Rarely, a Doppler probe may be required to identify the mesenteric vein and artery in obese patients with a thickened mesentery. The base of the mesentery is divided longitudinally overlying the SMV and a 3-4 cm length of vein is exposed (Figure 2). Small branches are ligated and large branches are preserved. If the SMV is >6 mm in diameter, further cephalad dissection is not necessary. However, in at least half of cases, cephalad dissection is required up to a branch of the SMA that courses across and anterior to the SMV and this usually defines the proximal extent of dissection. Depending on the size of the SMV, one may not necessarily need to perform a circumferential dissection as it can be controlled with a small side-biting vascular clamp; large branches may be controlled with small spring vascular clamps or suture material/vessel loops applied in a tourniquet fashion. Manipulation of the SMV may cause vasospasm so an accurate assessment of diameter should be made prior to dissection; application of topical papaverine may assist in cases of vasospasm. Mesenteric lymphatic drainage can be controlled with ligation or suture ligation; in cases of a thickened mesentery and deep vein, traction sutures may be applied medially and laterally in the mesentery to improve exposure. This area can then be packed off with sponges and the retractors removed.
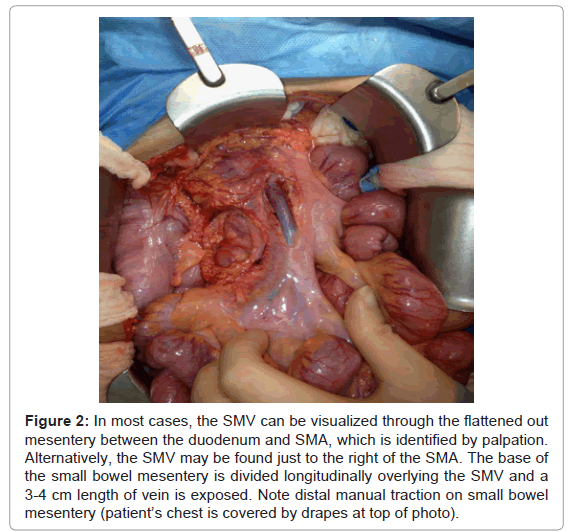
Figure 2: In most cases, the SMV can be visualized through the flattened out mesentery between the duodenum and SMA, which is identified by palpation. Alternatively, the SMV may be found just to the right of the SMA. The base of the small bowel mesentery is divided longitudinally overlying the SMV and a 3-4 cm length of vein is exposed. Note distal manual traction on small bowel mesentery (patient’s chest is covered by drapes at top of photo).
Attention is then directed to the right lower quadrant as medial and cephalad retraction is placed on the distal ileum and cecum and the retroperitoneum is entered using electocautery dissection. Care is taken to identify and preserve the right gonadal vein and right ureter although it is not always necessary to preserve the former structure. Further dissection of the right colon along the lateral peritoneum is sometimes necessary to improve exposure by entering the right paracolic space. The right common iliac artery is identified and a towel roll, laparotomy packs, and self-retaining retractors are placed to provide exposure. The iliac arterial circulation is then palpated and a decision is made on the best site for the arterial anastomosis. Most patients will have some degree of iliac atherosclerosis, especially posterior plaque, and a 3-4 cm length of artery must be identified that can be safely clamped and ideally is soft anteriorly. The arterial dissection may or may not be circumferential depending on the diameter of the artery and burden of atherosclerosis. Because the dissection is being performed intraperitoneal, meticulous ligation of lymphatics is not necessary although ligation of large lymphatic vessels is recommended. Care must be taken not to injure the left common iliac vein or distal vena cava if the common iliac artery is encircled; both of these venous structures may be adherent to the artery because of atherosclerosis. On occasion, small left-sided lateral branches off of the cava may need to be controlled. The right native ureter is usually encircled and retracted away from the area of arterial dissection (Figure 3). When this dissection is completed and an adequate target identified on the iliac artery for vascular anastomosis, the towel roll and laparotomy packs can be removed and a small window is made in an avascular area of the distal ileal mesentery just antero-cephalad to the iliac artery for passage of the “Y” graft. An umbilical tape or vessel loop is then passed through this window, which is located to the right and lateral of the SMV. Care must be taken not to damage small bowel, mesenteric vessels or the duodenum while creating this window.
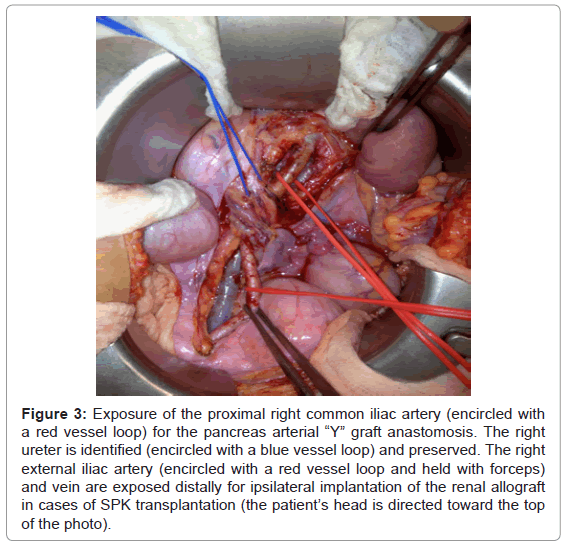
Figure 3: Exposure of the proximal right common iliac artery (encircled with a red vessel loop) for the pancreas arterial “Y” graft anastomosis. The right ureter is identified (encircled with a blue vessel loop) and preserved. The right external iliac artery (encircled with a red vessel loop and held with forceps) and vein are exposed distally for ipsilateral implantation of the renal allograft in cases of SPK transplantation (the patient’s head is directed toward the top of the photo).
Alternatively, one can make a larger window in the ileal mesentery at this time and expose the dissected right common iliac artery through the mesentery using an antero-cephalad approach. This approach may be possible in a thin patient and has the advantage of allowing for completion of both the venous and arterial anastomoses on the same (antero-cephalad) side of the mesentery. However, if the mesentery is thickened, foreshortened, or the patient is large, adequately exposing the iliac artery through the enlarged mesenteric window is not always possible. With this approach, one must remember to partially close the mesenteric window prior to wound closure to avoid the development of an internal hernia. A third technique involves sewing an isolated segment of vascular (donor) arterial graft end-to-side to the iliac artery prior to bringing the pancreas into the operative field. This arterial graft is marked anteriorly and then brought retrograde through the mesenteric window so that it is available on the antero-cephalad side of the mesentery for an end-to-end anastomosis to the “Y” graft of the pancreas.
In most instances, the portal vein of the pancreas and the common limb of the “Y” graft are anastomosed end-to-side to the recipient’s SMV and right common iliac artery, respectively, using a standard vascular running technique with fine polypropylene sutures. The pancreas is placed with the duodenal sweep and head positioned cephalad while the body and tail is directed caudad [6-13]. The venous anastomosis is usually performed first as the pancreas is wrapped in a laparotomy sponge surrounded by iced slush while retractors and laparotomy packs are repositioned to expose the SMV. The SMV and large branches are controlled proximally and distally. Prior to clamping the SMV, a decision must be made regarding the administration of systemic heparin intra-operatively. Indications for intravenous heparin may include solitary pancreas transplantation, preemptive SPK transplantation, history of thrombophilia or clotting disorder in the recipient, small or diseased donor or recipient vessels, prolonged pancreas cold ischemia, extended donor criteria, or history of prior pancreas graft thrombosis. The incidence of early vascular thrombosis, which in most cases is venous in origin, is similar regardless of surgical technique so portal venous outflow per se is not an indication for systemic heparinization. Local heparinized saline is used in nearly all cases unless the patient has a history of a heparin allergy. In cases in which a decision is made to administer intravenous heparin, we typically administer 2000-3000 units of heparin (30-50 units/kg), which is allowed to circulate for 3 minutes prior to clamping the SMV (Figure 4). After completion of the venous anastomosis, a spring clamp is placed on the graft portal vein and all clamps are released from the SMV to restore venous outflow in the native mesenteric circulation. This in effect tests the integrity of the venous anastomosis and additional interrupted sutures are placed as needed to secure adequate homeostasis.
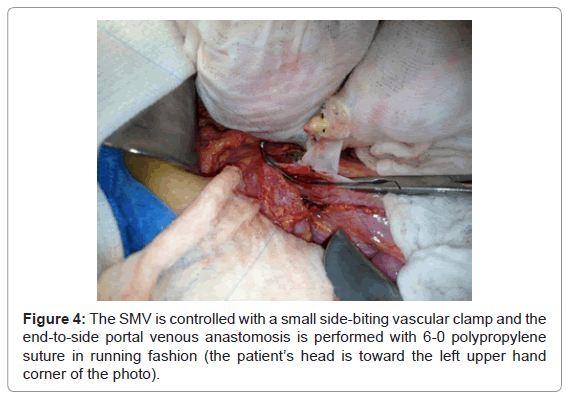
Figure 4: The SMV is controlled with a small side-biting vascular clamp and the end-to-side portal venous anastomosis is performed with 6-0 polypropylene suture in running fashion (the patient’s head is toward the left upper hand corner of the photo).
The interposition “Y” graft is then brought out of the sponge wrap and directed through the window in the distal ileal mesentery taking care not to create any torsion or twist. One can inject heparinized saline through the common iliac conduit to ensure that the “Y” graft is not twisted and the correct orientation of the conduit can be either tagged with a suture or marked with a pen. Laparotomy packs and retractors are repositioned to expose the site chosen for the arterial anastomosis, which may range from the distal aorta to either common iliac artery (Figure 5) or to the right external iliac artery. This part of the exposure may be somewhat challenging because the retractors are pulling cephalad on the distal ileum and cecum while the “Y” graft is being pulled caudad through the mesenteric window. The end of the conduit may be cut in an oblique or “fish-mouth” fashion to enlarge the size of the anastomosis. After completion of the arterial anastomosis, a vascular clamp is placed on the conduit and vascular clamps are released from the native arterial circulation to ensure adequate distal flow and to test the integrity of the arterial anastomosis. Once again, additional interrupted sutures are placed in the anastomosis as needed to secure adequate hemostasis. This technique of “pre-testing” both vascular anastomoses is helpful so that specific attention can be directed to achieving hemostasis solely on the pancreas graft once reperfusion occurs. Moreover, it may be more difficult to expose and repair anastomotic bleeding following reperfusion. It is useful to then place a vascular clamp on the “Y” graft on the antero-cephalad side of the mesentery adjacent to the pancreas and remove the initial clamp so that any leaks on the “Y” graft are identified and repaired. Alternatively, the arterial anastomosis can be performed through the mesenteric window either end-to-side to the iliac artery or end-to-end to a previously placed graft using the antero-cephalad techniques described above.

Figure 5: The interposition “Y” graft is brought out of the sponge wrap and directed through a window created in the distal ileal mesentery taking care not to create any torsion or twist. The “Y” graft is marked anteriorly to maintain orientation as it traverses the mesenteric window. Laparotomy packs and retractors are repositioned to expose the site chosen for the arterial anastomosis, which may range from the distal aorta to either common iliac artery or the right external iliac artery. The proximal iliac artery is exposed in this case and an end-to-side anastomosis is being performed between the “Y” graft and right common iliac artery (patient’s head directed toward upper left hand corner of photo).
Prior to revascularization, the sponge wrap and iced slush are removed from around the pancreas as the retractors and sponges are removed from the pelvis and the pancreas graft is exposed. We typically administer 12.5-25 grams of mannitol, a free radical scavenger and colloid osmotic agent, in an attempt to minimize reperfusion pancreatitis. Initially, the pancreas is perfused retrograde as the spring clamp is removed from the portal vein; any venous bleeders are controlled with ligatures or suture ligatures. The vascular clamp on the “Y” graft is then released to reperfuse the pancreas (Figure 6); specific attention is directed to the major vessels and anastomoses, the tail of the pancreas, the root of the mesentery, and adjacent to the duodenum to identify any bleeding sites that require suture ligation. With gradual rewarming, additional bleeding sites may be noted. The orientation of the vessels must be checked to confirm that there is no torsion, twist, or tension of the inflow and outflow vessels. At this point one would typically perform a graft splenectomy but we advocate removing the spleen on the back bench because it is easier, safer, bloodless, and absence of the spleen makes the implantation and exposure less difficult.
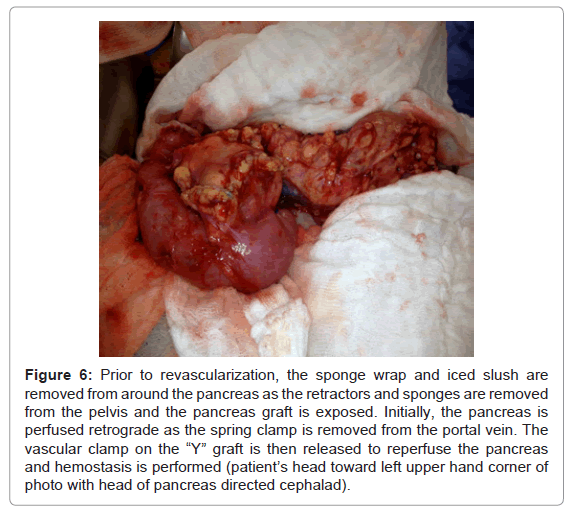
Figure 6: Prior to revascularization, the sponge wrap and iced slush are removed from around the pancreas as the retractors and sponges are removed from the pelvis and the pancreas graft is exposed. Initially, the pancreas is perfused retrograde as the spring clamp is removed from the portal vein. The vascular clamp on the “Y” graft is then released to reperfuse the pancreas and hemostasis is performed (patient’s head toward left upper hand corner of photo with head of pancreas directed cephalad).
Following revascularization and achieving hemostasis, a decision must be made regarding how to best position the duodenum and pancreatic parenchyma. Most commonly the pancreas has a vertical orientation just to the right of midline but on occasion the body and tail may be pointing towards the right or left lower quadrant or even have a transverse lie, depending on the orientation of the vessels. With reperfusion, the duodenum will soon become distended so a prompt decision must be made regarding the site of the enteric anastomosis both on the duodenal side as well as in the recipient’s small bowel. The enteric anastomosis can be created directly into a bowel loop that is not excluded from the transit of intestinal contents [6-13], in a Roux-en-Y limb that is diverted from the enteric stream with or without a venting jejunostomy [23], in an omega loop [24], or directly into the native duodenum or stomach [25-27]. The latter three options have been reported in small series whereas the former two options are most common. The main advantage of using the native duodenum or stomach is easy access for endoscopic surveillance and biopsy. However, considering that 5-10% of pancreas grafts are at risk for early technical failure, most surgeons prefer to avoid either the native duodenum or stomach for enteric drainage. If the graft duodenum does not appear well perfused, it is always safer to create a diverting Roux limb although this involves an additional enteric anastomosis.
The enteric anastomosis can be stapled (employing either a linear [28] or circular device [29]) or hand-sewn although some surgeons believe that the anastomotic bleeding rate may be higher with a stapled enteric anastomosis. The most common technique is a 2-layer hand sewn anastomosis consisting of an external layer of interrupted non-absorbable sutures and an inner layer of running continuous absorbable suture to create a “watertight” closure. The site of enteric anastomosis can range from native stomach to distal ileum and the anastomosis can be constructed end-to-end, end-to-side, or side-to-side; the most common technique is a direct side-to-side anastomosis between the graft duodenum and small bowel. With the portal-enteric technique, the proximal graft duodenum can be used for anastomosis to the recipient’s jejunum whereas the distal graft duodenum can be used for anastomosis to the recipient’s ileum. We prefer the latter technique with placement of the enteric anastomosis on the posterior aspect of the 3rd or 4th portion of the graft duodenum to take advantage of dependent drainage of the denervated, atonic graft duodenum when the patient is either in the supine or erect position. A site is chosen in the proximal ileum approximately 5 feet from the ileo-cecal valve and a posterior row of interrupted non-absorbable sutures are placed between distal graft duodenum and loop of ileum aligned in a side-to-side fashion. The operative field is then packed off and side to side enterotomies are created with electrocautery after the afferent and efferent limbs of the ileum are controlled with non-crushing bowel clamps. The contents of the duodenum are evacuated and decompressed with suction taking care to minimize spillage. The color of the duodenal mucosa is inspected to ensure adequate perfusion as the duodenum is irrigated with antibiotic solution. We prefer to use an interlocking running absorbable suture on the inner layer to secure adequate hemostasis followed by an anterior row of interrupted non-absorbable suture to complete the 2-layer hand sewn side-to-side enteric anastomosis (Figure 7). The length of the anastomosis usually ranges from 3-5 cm and the bowel clamps are released following completion of the inner layer. With retroperitoneal placement of the pancreas behind the right colon, a window is needed in the right colon mesentery in order to create the enteric anastomosis, which is usually performed in a side-to-side fashion with or without a diverting Roux limb (Figure 8). One can always “start” with a side-to-side enteric anastomosis and then easily switch to a diverting Roux limb for whatever reason by staple dividing the afferent limb just proximal to the anastomosis and connecting this proximal end 40 cm or more distally to the efferent limb in either an end-to-side or side-to-side fashion.
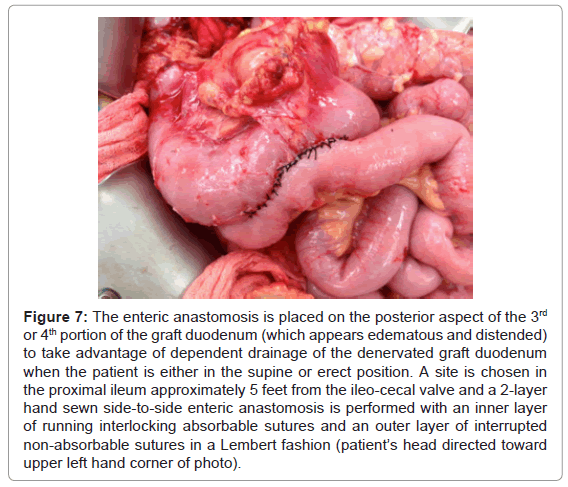
Figure 7: The enteric anastomosis is placed on the posterior aspect of the 3rd or 4th portion of the graft duodenum (which appears edematous and distended) to take advantage of dependent drainage of the denervated graft duodenum when the patient is either in the supine or erect position. A site is chosen in the proximal ileum approximately 5 feet from the ileo-cecal valve and a 2-layer hand sewn side-to-side enteric anastomosis is performed with an inner layer of running interlocking absorbable sutures and an outer layer of interrupted non-absorbable sutures in a Lembert fashion (patient’s head directed toward upper left hand corner of photo).
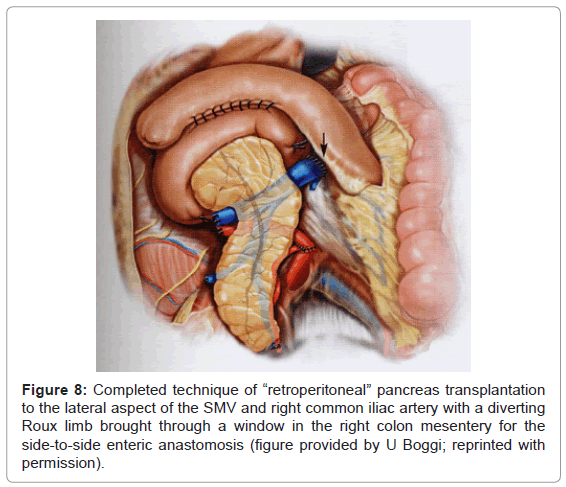
Figure 8: Completed technique of “retroperitoneal” pancreas transplantation to the lateral aspect of the SMV and right common iliac artery with a diverting Roux limb brought through a window in the right colon mesentery for the side-to-side enteric anastomosis (figure provided by U Boggi; reprinted with permission).
Following completion of the enteric anastomosis, gloves is changed and the operative field is copiously lavaged with antibiotic solution regardless of whether or not we are proceeding with a simultaneous kidney transplant or wound closure. Because we prefer to transplant the pancreas first in SPK transplantation in order to minimize pancreas cold ischemia, a simultaneous kidney transplant is then performed either ipsilateral on the right external iliac vessels or contralateral on the left side. We have adopted the ipsilateral technique [20], because it reduces operating time and leaves the left side available for future transplantation. When exposing the iliac vessels for kidney transplantation, care must be taken with retracting the viscera to avoid excessive traction on the pancreas graft; we attempt to expose the tail of the pancreas during this time to confirm and check perfusion. Following completion of the transplant procedure(s), peri-pancreatic drains can be avoided, employed selectively, or used routinely. We prefer placement of two drains; one posterior to the enteric anastomosis and the other adjacent to the iliac artery anastomosis/kidney transplant in a dependent position in the right pelvis.
A major advantage of portal venous outflow is that it is primarily a mid-abdominal rather than a pelvic procedure, which is beneficial in patients who have had previous transplants or pelvic procedures. Disadvantages, however, are that the arterial anastomosis may be difficult and require a long interposition “Y” graft (especially in patients with central, omental, or mesenteric obesity) and the pancreas graft is surrounded by bowel loops and may be poorly accessible for ultrasonographic imaging, percutaneous biopsy, and potentially at risk for venous torsion. Consequently, we usually attempt to anchor the tail of the pancreas graft to the anterior abdominal wall with interrupted non-absorbable sutures and “mark” this area externally by having one of the drains exit the abdominal wall at this location. These disadvantages can also be minimized by approaching the SMV from the lateral retroperitoneal aspect instead of from the anterior route, with the pancreas graft eventually situated posterior to the right colon. Because the distance between the graft and right iliac artery is not influenced by the thickness of the mesentery and there are no interposing bowel loops (other than the right colon) between the graft and lateral abdominal wall with this approach, the arterial anastomosis can be performed using a shorter interposition “Y” graft and the pancreas is more easily visualized and accessible for ultrasonographic imaging and percutaneous biopsy.
Prior to wound closure with either the anterior or lateral approaches to the SMV, it is important to position the efferent limb in such a way as to remove any traction or tension in order to avoid a functional bowel obstruction secondary to angulation of the bowel just distal to the enteric anastomosis, which could present as an enteric leak or anastomotic “blow-out”. Although some surgeons prefer to “wrap” the pancreas in an omental leaf or patch, we do not believe that this step is necessary because the arterial anastomosis is well protected from either pancreatic inflammation or enteric leakage by the small bowel mesentery. Moreover, any fat that comes in direct contact with the reperfused pancreas may result in liquefaction necrosis, which contributes to the development of peri-pancreatic fluid collections that could subsequently become infected or require drainage.
Purported benefits of pancreas transplantation with portal venous drainage include technical, metabolic, and immunologic “advantages” [6-13,30-32]. However, these benefits have not been confirmed by either prospective cohort studies, randomized controlled trials, or large analyses based on registry databases. Alternatively, there are likewise no well controlled studies to suggest any major disadvantages or unique risks associated with portal venous drainage other than the technical considerations, concerns, and contraindications discussed in this chapter. Although numerous variations exist in the basic surgical techniques of pancreas transplantation and nuances continue to be described, current philosophy dictates that the most appropriate technique to be performed is the one with which the individual surgeon feels most comfortable.