Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2015) Volume 5, Issue 1
Patients with chronic pancreatitis (CP) may have presentations resembling pancreatic cancer (PaC) and are also high-risk for developing PaC. Surveillance of PaC in CP is therefore important but difficult and challenging. Candidates for PaC surveillance include hereditary pancreatitis, tropical chronic pancreatitis or any CP patients with clinical suspicions or the presence of pancreatic mass. Currently, the best potential surveillance tools are probably endoscopic ultrasonography with fine needle aspiration and positron emission tomography
<Keywords: Chronic pancreatitis, Pancreatic cancer, Surveillance
Patients with chronic pancreatitis (CP) commonly present with abdominal pain, steatorrhea, weight loss or obstructive jaundice, which resemble those of pancreatic cancer (PaC) from ductal adenocarcinoma and cause diagnostic confusion. Furthermore, CP of any type is a well known risk for developing PaC later in the course of the disease (Table 1) [1-4]. Since PaC is deadly and the only believed chance for cure is to detect it when it is as small and as early as possible. Thus, surveillance of patients with CP who are at risk for developing PaC seems to be reasonable, though it is unclear that surveillance will really improve patients’ survival or be just a lead time bias. The main obstacle is that the background of the pancreas with CP usually interferes the detection of PaC by any imaging tool. Thus, surveillance of PaC in CP is one of the most difficult issues in Pancreatology. Recently, there have been some discoveries that might improve what we can do. This article will summarize the current status and future hopes of how to surveillance PaC in CP.
| Etiologies of CP | Proportions in CP patients (%) | Relative risk for PaC (folds) | Lifetime risk (%) | Remarks |
|---|---|---|---|---|
| CP, unspecified types | 100 | 13 [1] | 2-4 [2] | 1% every 5 years |
| Hereditary pancreatitis | 0-6 [5,6] | 69 [1] | 40-55 [3] | 75% with paternal inheritance |
| Tropical chronic pancreatitis | 4-6 [7,8]* | 5-100 [1,4]** | Unknown [4,7]*** | Data from India |
CP, chronic pancreatitis; PaC, pancreatic cancer; *Data was from 2 recent studies, which markedly declined from the 58-70% frequency in the past. The number is probably closed to zero in the Westerns; **5 folds for histology-proven PaC, 100 folds if including all suspicious PaC; ***Prevalence was 4% in a recent study of 1,086 patients from India
Table 1: Risks of PaC in CP according to the etiologies [1-8].
Which CP Patients Need Surveillance?
Since the incidence of PaC in CP is not that high, to survey all CP patients for PaC with any current modality will result in too many false positive and false negative beyond acceptable and may cause problem rather than benefit. Thus, the strategy to select only subgroups of CP with higher pre-test probability for PaC may be more appropriate. CP patients with higher likelihood for PaC who are probably candidates for PaC surveillance are summarized in Table 2.
| Specific types of CP |
|---|
| Hereditary pancreatitis |
| Tropical chronic pancreatitis |
| Clinical suspicions |
| Obstructive jaundice |
| Reappearance of pain after pain relief |
| Unexplained weight loss despite pancreatic enzyme therapy |
| Markedly elevated CA 19-9 |
| Imaging suspicions |
| Pancreatic mass |
Table 2: Possible CP candidates for PaC surveillance
Given the highest relative risks and lifetime risks for PaC (Table 1), hereditary pancreatitis (HP) and tropical chronic pancreatitis (TCP) may be the most appropriate candidates for PaC surveillance than other types of CP [9]. For the other types of CP, surveillance should be performed when there are some clinical suspicions of PaC (Table 2), i.e. the presence of obstructive jaundice, re-appearance of pain in patients who have already had pain relief or patients with painless late-onset idiopathic CP, unexplained weight loss despite adequate pancreatic enzyme replacement or markedly elevated CA 19-9. These clinical clues though make sense, have never been proven of their accuracy. Last, but very important, is the presence of pancreatic mass from cross-sectional imaging.
Surveillance tools for detecting PaC in CP are any method that can pick up PaC and differentiate it from the background of CP and, in particular, inflammatory mass or focal CP. Therefore, the candidate tools are usually derived from studies that focused on how to differentiate PaC from focal CP.Unfortunately; most studies compared focal CP to conventional PaC in patients without CP. Thus, ones had to keep in mind that the capabilities of the differential features derived by these studies were probably overrated and the accuracy will likely be lower when being used to detect PaC in the setting of underlying CP.
Serum CA 19-9
The role of CA 19-9 to differentiate PaC from CP has been prospectively studied in patients who had pancreatic mass from imaging studies [10]. CA 19-9, using cut-off >40 U/ml, had sensitivity, specificity, positive (PPV) and negative predictive value (NPV) 81%, 81%, 90% and 69%, respectively for PaC [10]. It seems to be suboptimal to the standard surveillance tool.
No study has tested the capability of CA 19-9 for the surveillance of PaC in patients with HP, TCP, or CP without pancreatic mass. However, it is likely that the utility would be low.
Cross-sectional imaging studies
Common findings from computed tomography (CT) or magnetic resonance imaging (MRI) that favor PaC than focal CP are the presence of heterogeneous hypodensity mass (or hypointensity by MRI) and pancreatic duct cut-off. The less common but more specific findings for PaC are invasion of vessels, hepatic metastasis and ascites [10]. On the other hands, features that favor CP are iso- or homogeneous mass, presence of calcifications or cysts [10]. Using these features, CT scan was shown to have sensitivity 94% and specificity 95% for the differentiation between PaC and focal CP [10].
Duct-penetrating sign is a feature, which has been proposed to indicate inflammatory mass. Study with MRCP showed the sensitivity 85% and specificity 96% of this sign for focal CP [11]. However, results were poorer with CT probably because it is more difficult to trace the pancreatic duct with CT. One study of only patients with focal CP demonstrated duct-penetrating sign in only 30% by CT (Figure 1) and 50% conversely had pancreatic duct cut-off resembling PaC [12].
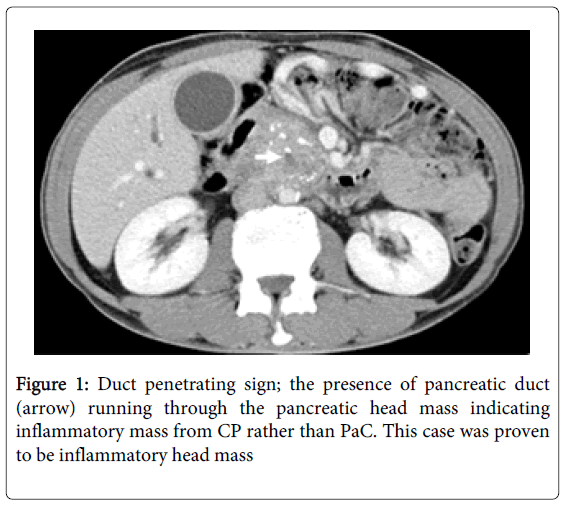
Figure 1: Duct penetrating sign; the presence of pancreatic duct (arrow) running through the pancreatic head mass indicating inflammatory mass from CP rather than PaC. This case was proven to be inflammatory head mass
Features that are frequently quoted to be useful and should warrant physician for the presence of PaC in CP are the displacement of pancreatic calcifications and duct-penetrating sign [11,13,14], though the accuracies are unknown.
No study has tested the accuracies of CT or MRI for the surveillance of PaC in patients with already known CP.
Positron emission tomography
Positron emission tomography (PET) scan has widely been studied in the differentiation between focal CP and PaC. Meta-analysis showed that the overall sensitivity was 90% and specificity was 84% for differentiating focal CP from PaC [15].
One study has used PET to detect PaC in the setting of CP and demonstrated a sensitivity of 83% and specificity of 87% for PaC [16].
Endoscopic ultrasonography with or without fine needle aspiration
Endoscopic ultrasonography (EUS) and fine needle aspiration (FNA) has been accepted as the most sensitive tool to detect small pancreatic lesions. It has become the investigation of choice for the detection of small pancreatic tumor, e.g. insulinoma and for surveillance of population at highest risk for PaC i.e. familial pancreatic cancer and some specific inherited syndromes [17]. However, the ability of EUS to detect PaC in the setting of CP is generally worse due to the background of lobulation, which can be falsely interpreted as masses (Figure 2) and calcifications, which can create acoustic shadows and mask the view of US [18]. EUS findings that should warrant physician for PaC in the setting of CP include focal distinctive hypoechoic area, absence of hyperechoic foci, displacement of calcifications and periductalhypoechoic sign around dilated pancreatic duct [19]. One study showed that EUS alone had sensitivity 64% and specificity 76% for PaC detection in the setting of CP, of which were significantly much improved when adding FNA (73% and 100%) [20].
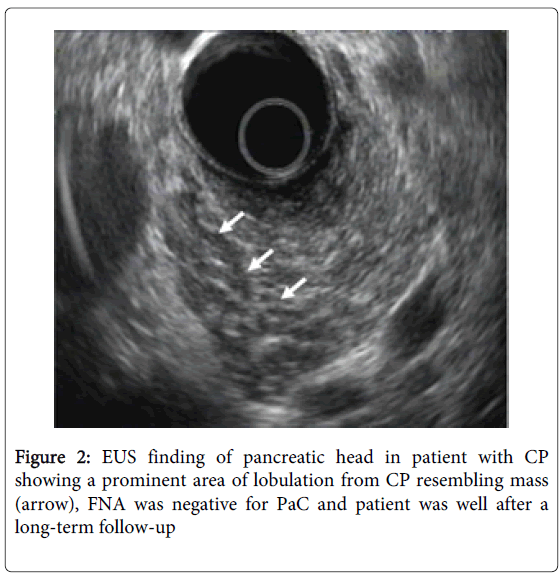
Figure 2: EUS finding of pancreatic head in patient with CP showing a prominent area of lobulation from CP resembling mass (arrow), FNA was negative for PaC and patient was well after a long-term follow-up
FNA significantly increases the diagnostic yield of EUS for solid pancreatic lesions. Meta-analysis reported pool sensitivity 85% and specificity 98% of EUS-FNA for solid pancreatic mass [21]. As predicted, the sensitivity of EUS-FNA for PaC in the setting of CP is significantly lower (54-74%) compared to those without CP (89-91%) [22,23], mostly due to incorrect targeting and inadequate sampling [18]. Proposed techniques to increase the yield of EUS-FNA in the setting of CP include on-site cytopathologist [21, 24], more FNA passes (at least 7 passes) [25], using suction, 19G needle or trucut [18] and finally, using new technologies, i.e. contrast-enhanced EUS or elastography (see next topics).
EUS with novel techniques
EUS-elastography: EUS-elastography has been used with the rational that PaC is usually stiffer (shown as higher qualitative score and strain ratio) than focal CP mass (Figure 3). Many studies have used EUS-elastography to differentiate PaC from focal CP and meta-analysis showed a sensitivity of 95% and specificity of 94% [26]. However, no study has used EUS-elastography for the surveillance of PaC in patients with underlying CP.
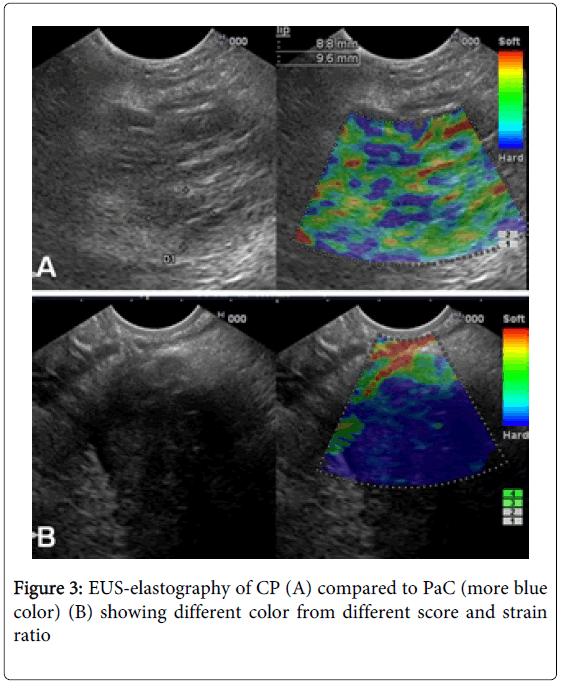
Figure 3: EUS-elastography of CP (A) compared to PaC (more blue color) (B) showing different color from different score and strain ratio
Contrast-enhanced EUS: With this technique, after contrast injection, the PaC is typically hypoenhanced and in contrast to the iso- or hyperenhancement of focal CP. Many studies have tested the accuracy of contrast-enhanced EUS for the differentiation between PaC and focal CP and the meta-analysis revealed a sensitivity of 94% and specificity of 89% [27]. Again, no study has used contrast-enhanced EUS to surveillance PaC in patients with CP.
Pancreatic juice study
K-ras mutation is the most common and earliest genetic derangement during the development of PaC. Thus, many studies tried to determine whether detection of K-ras mutation in pancreatic juice collected during pancreatic function test or endoscopic retrograde cholangiopancreatography of CP patients could predict the development of PaC [28-31]. Overall, K-ras mutation was found in 9-52% (average 27%) of patients with CP, of which 0-20% (average 9%) truly developed PaCduring long-term follow-up [28-31]. Thus, analysis of K-ras mutations in pancreatic juice of CP patients could not be acceptable as surveillance tool since its false positive rate is too high.
Table 3 summarizes the sensitivity and specificity of any given candidate for the differentiation between PaC and focal CP and, more desirable; to detect PaC in the setting of CP. PET scan and EUS-FNA are possible candidates. However, with cost and availability, EUS-FNA may be preferred over PET. PET may be preferred only in patients with dense calcifications or stones which significantly obscure the views of EUS. EUS-elastography and contrast-enhanced EUS need some more studies on the use for surveillance in CP but likely to become complementary tests to EUS-FNA in the future.
| Surveillance tools | To differentiate PaC from focal CP | To detect PaC in CP | ||
|---|---|---|---|---|
| Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | |
| CA 19-9 [10] | 81 | 81 | - | - |
| CT/MRI [10] | 94 | 95 | - | - |
| PET [15,16] | 90 | 84 | 83 | 87 |
| EUS alone [20] | - | - | 64 | 76 |
| EUS-FNA [20,22,23] | 89-91 | 94-100 | 54-74 | 100 |
| EUS elastography [26] | 95 | 94 | - | - |
| Contrast-enhanced EUS [27] | 94 | 89 | - | - |
| Pancreatic juice study [28-31] | - | - | 100 | 75 |
CP, chronic pancreatitis; CT, computed tomography; EUS, endoscopic ultrasonography; FNA, fine needle aspiration; MRI, magnetic resonance imaging; PaC, pancreatic cancer; PET, positron emission tomography
Table 3: Sensitivity and specificity of various modalities to differentiate PaC from focal CP
So what is the recommendation in the real clinical practice? The authors’ opinions are as follows
1. In CP patients with clinical suspicions: Perform CT/MRI first. If there is a mass, evaluate with EUS-FNA. Contrast-enhanced EUS or elastography may be used in selected cases. If there is no mass detected by CT/MRI, a further evaluation with EUS is recommended. If there is no focal lesion by EUS, patient may be followed-up clinically and EUS may be repeated if it remains suspicious, for example, within 3-6 months, though the best interval remains unknown. PET may be performed if the EUS-image quality is significantly obscured by calcifications or stones (Table 2).
2. In HP or TCP without clinical suspicions or mass: Currently, there is no surveillance tool that is good enough. Existing guideline of HP did not support surveillance but stated that surveillance could be offered in HP with age >40 years [9]. Nevertheless, in case ones need to do so, if the pancreas does not have much calcifications or stones, yearly EUS might be appropriate. Contrast-enhancement can be added in some cases. If mass is found, perform EUS-FNA. In a case with too many calcifications or stones that obscure many EUS views, no investigation can currently solve this problem. PET scan may be an option but needs more studies because all of the previous PET studies included only patients with pancreatic mass already identified by other imaging. Most importantly, long-term safety and cost of PET must be considered seriously.