Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2015) Volume 3, Issue 3
Background: Distal radius fractures are the most common fractures occurring in emergency. There’s no evidence for the superiority of one of the different treatment we can choose, particularly in old patients. The purpose of the present study was to determine if a surgical treatment for DRF in older than 85 is justified and to compare these results to a conservative treatment.
Methods: This is an observational retrospective study that included all patients older than 85 years diagnosed with distal radius fractures and hospitalized in our institution between January 1st, 2010 and June 30th 2013. Patients were divided in 2 groups. The main outcome was the functional result at the end of the patient’s follow up. It was measured objectively with wrist motility and subjectively with the common satisfaction of the patient and the surgeon. Secondary outcomes included hospitalization time, immobilization duration, rate and nature of complications, and the pain at the end of the follow up.
Results: 94 were included, 20 had a conservative treatment, 74 a surgical treatment. Groups were homogeneous at the admission. There were not statistically significant difference in the main outcome with the objective or the subjective evaluation (p=0.046; OR: 0.1729 CI-95% [0.0205; 1.2662]). Immobilization time was significantly longer in the surgical treatment group (42,4 vs. 35,7 days p: 0.045).
Conclusions: Conservative treatment is the best treatment for distal radius fractures in elderly.
Level of Evidence: Level III.
<Keywords: Wrist fracture; Elderly; Conservative treatment
Distal radius fractures (DRF) are the most common fractures occurring in emergency [1,2] (640000 cases per years in the USA) and the second fracture site in patients older than 65 years after proximal femur fractures. Ten percent (10%) of women older than 65 years will have a DRF[3]. Life expectancy is always growing [4]. A lot of treatment exists for these fractures but there are only few evidence of the superiority of one on them particularly in old patients[5].
The purpose of the present study was to determine if a surgical treatment for DRF in older than 85 years is justified and to compare these results to a conservative treatment.
This is an observational retrospective study that included all patients older than 85 diagnosed with DRF and hospitalized in our institution between January 1st, 2010 and June 30th, 2013. Patients were divided in 2 groups: surgical treatment and conservative treatment. A systematic review of the patients’ medical records was done. We collected information about patients demographics (age, sex, lifestyle, comorbidities), the existence of contraindication for anaesthesia, and we noted the nature of the trauma and if the fractures were intraarticular or not. The characteristics of the fractures were evaluated by re-examining the radiographs, and were categorized as displaced fractures, radio-carpal intra-articular and distal radio-ulnar intraarticular fractures. Fractures were classified using the Kapanji’s [6] wrist fractures classification. Characteristics of the treatment were analyzed (immobilization time, physiotherapy). At last, the follow up was analyses (time of the follow up, wrist function, recovery time, complications).
Patients were identified using the digital medical records of the hospital. We used the CIM-10 classification [7] codes: S52-5 and S52-6. Statistical analyses were conducted using the on-line software of the Jussieu Paris VI University: BiostaTGV [8]. Student’s t-test and Fisher’s exact F-test were used for that mean. The main outcome was the functional result at the end of the patient’s follow up. It was measured objectively with wrist motility and subjectively with the common satisfaction of the patient and the surgeon. Secondary outcomes included hospitalization time, immobilization duration, rate and nature of complications, and the pain at the end of the follow up.
There was no external funding source for this study.
Ninety-four patients were hospitalized in our institution between January 1st, 2010 and June 30th 2013. There were 74 surgical treatments and 20 conservatives’ treatments. The mean age was 88.7 (85-101). Groups were homogeneous at the admission (Table 1). The middle follow-up was 78.8 days.
| Surgery | Conservative treatment | p | ||
|---|---|---|---|---|
| Age | 88.5 | 89.4 | 0.30 | |
| Gender | Men | 2 | 1 | 0.52 |
| Women | 72 | 19 | ||
| Retierement home | 32.00% | 45.00% | 0.30 | |
| Anticoagulation | 56.00% | 45.00% | 0.45 | |
| Fall | 98.60% | 100.00% | 1.00 | |
| Time to consultation | 0.19 | 0.2 | 0.95 | |
| Associated trauma | 31.08% | 0.60% | 0.04 | |
| Side | Left | 42 | 12 | 1.00 |
| Right | 32 | 8 | 1.00 | |
| Fracture | Articular | 14.00% | 0.00% | 0.11 |
| Displacement | 97.30% | 80.00% | 0.02 | |
| Complication | 0 | 0 | 1.00 | |
| Kapanji's Classification | 0 | 1 | 5 | 0.00 |
| 1 | 61 | 13 | ||
| 2 | 6 | 1 | ||
| 3 | 0 | 0 | ||
| 4 | 7 | 0 |
Table 1: Patients baseline characterstics.
The main outcome results were not statistically significant with the objective nor the subjective evaluation (p=0.046; OR: 0.1729 CI-95% [0.0205; 1.2662]) (Table 2).
| Motilities | Surgery | Conservative Treatment | p | |
|---|---|---|---|---|
| Objective Main Outcome(Degrees) | Flexion | 52.14 | 38.33 | 0.26 |
| Extension | 32.86 | 38.33 | 0.86 | |
| Abduction | 14.17 | 11.67 | 0.67 | |
| Adduction | 28.33 | 28.33 | 1.00 | |
| Suppination | 63.33 | 53.33 | 0.66 | |
| Pronation | 73.33 | 33.33 | 0.29 |
Table 2: Main outcome results.
Hospitalization time was significantly longer in the conservative treatment group (10.8 vs. 5.1 days p: 0,039). Immobilization time was significantly longer in the surgical treatment group (42,4 vs. 35,7 days p: 0.045).
In the group « surgical treatment » 67 reduction (ORIF) with metal pins and 7 plates were realized (Table 3).
| Surgery | Conservative Treatment | p | |
|---|---|---|---|
| Disunion | 13.24% | 25.00% | 0.17 |
| Malunion | 42.38% | 35.73% | 0.04 |
| Hospitalisation time (days) | 5.14 | 10.8 | 0.04 |
| Complications | 25.67% | 40.00% | 0.26 |
| Pain | 26.92% | 57.14% | 0.19 |
Table 3: Secondaries outcomes results.
73% had physiotherapy in the two groups (p=1). 60 % of patients were followed by physical therapist after immobilization (64% of patients in the surgery group and 53% of patients in the conservative treatment group p>0.05). Other patients had self-physical therapy 0.28% of patients had complications (Figure 1). There were only 2 cases of arthritis following surgical treatment; other complications were expected in this type of fractures. There was no tendon complication found that was related to surgery.
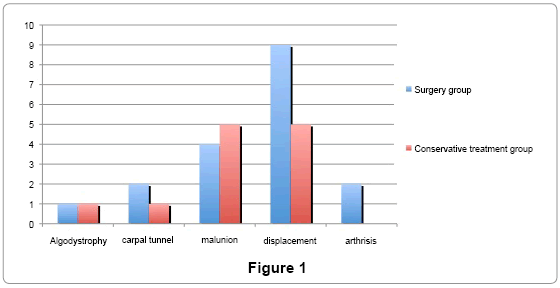
Figure 1
Our study did not show any significant difference between our 2 groups. This might be due to the small patients sample in the conservative treatment group. Most patients with conservative treatment are managed in the emergency room and thus are not easily identified found in our electronic medical record. Only a prospective study could reduce this bias of recruitment. We can estimate that less of 1 patient on 2 is usually hospitalized for a conservative treatment [9]. In their study, Camelot et al [10] followed consecutively 280 patients with a DRF treated conservatively. Their complication rate and nature of these complications were comparable to ours. This element consolidates the quality of our study, despite the bias of recruitment.
To classify fractures, we used Kapanji’s classification [11]. Although there’s no perfect classification for DRF [12], this one seems to be clear and reproducible particularly for the stability and the comminution. Moreover, it’s a very popular and used classification by orthopedic surgeons.
Our mean follow-up time was relatively short: 78.8 days. This is another limit of the study. In fact it has clearly been shown that a 12 month follow-up [13] is necessary for definitive results evaluation. However, the most frequently seen complications appears very early in the follow up.
Although most of the studies focus on patient over 65 [14]. We decided to study patients older than 85. So we can evaluate the benefit of a surgical treatment versus a conservative treatment in an older population. Taking in consideration, that, this group of patients will have a reduction of their normal daily activity and different requirements in functional outcomes compared to a younger population.
Conservative treatment of DRF has always been a dilemma to surgeons. Indeed, quality of the anatomic reduction assessed on radiographs is often recognized as a predictive factor for a good functional result [15,16]. The main criterion is the respect of the radiocarpal articulation [17], which could be achieved using volar-locking plates [18]. However, several studies proved that this dogma was disputable: despites wrist arthritis, which is significantly more frequent in the case of radiographic displacement, functional result is not different [19,20]. In our study, the length of stay was longer in patients receiving a conservative treatment and this could be contributed to their extensive comorbidities.
In 2011, Diaz-Garcia et al. published a metanalysis comparing conservative and surgical treatment in DRF in patients older than 60 years [21]. Functional, radiologic results and complications were compared. Twenty-one studies and 1027 patients were analyzed. There were 220 (21%) conservative treatments. There was no significant difference found on the functional result despite a worst radiographic result in the conservative treatment group. However, there was significantly more complication in the surgical treatment group. A systematic review of the literature comparing conservative treatment and external fixation in DRF [21] found similar results. As well as the prospective Arora et al [22] study in 2012 which found no differences after a 12 month follow up in instable DRF between anterior locking plates and a conservative treatment.
No significant differences were found between surgical and conservative treatment for DRF in patients older than 85 year. This result is in agreement with what has been published on DRF conservative treatment. We can conclude that conservative management is the best treatment needed for DRF. These results need to be re-inforced by a prospective study with an extended follow-up period.
The authors declare no conflict of interest.