Journal of Medical Diagnostic Methods
Open Access
ISSN: 2168-9784
ISSN: 2168-9784
Case Report - (2016) Volume 5, Issue 3
Avascular necrosis of femur as the name implies is directly related to the compromising state of the blood supply and their further pathological changes at that site. This results in major musculoskeletal disability. This may be traumatic or non-traumatic as the crux of the underlying problem is ischemia because of disruption of the vascular nourishment. This eventually leads to the death of marrow and osteocytes which leads to osteonecrosis. This shows in imaging in the form of ischemia or bone collapse and the diagnosis is made with the help of imaging armamentarium. The age of presentation and the history are very important to know before the diagnosis is made. Plain radiography, Computerized Tomography (CT) and Magnetic Resonance Imaging (MRI) play a pivot role in clinching the diagnosis. We present 28-years old male who reported with pain in both hip joints with painful and restricted movements. He was diagnosed as bilateral avascular necrosis of hips on the basis of the radiological findings.
Keywords: Avascular necrosis; Computed tomography; Magnetic resonance imaging; Osteonecrosis
Munro described this entity first time in 1738 and then Curveilhier further elaborated in 1835 with background of various pathological changes in bones. Markin in 1962 described about 27 cases going through the length and breadth of all the changes because of AVN and their impact on the bone in question. If the bone is participating in joint formation than the cartilage is also affected and can lead to osteochondritis dissecans.
28-years old male reported with the complaints of pain in both the hips of approximate two years duration. The symptoms were mild to begin with but have shown progression in two years. There was no relief with the symptomatic treatment in the local dispensary. He reported to the orthopedic department now with pain and difficulty in walking. On examination he was well built with normal physique without any visible disability. There was no history of trauma or any systemic disease like diabetes, hypertension, renal disease or thyroid problem. He was not on any long term medication for any systemic disease. He was not able to put weight on his hip joints and was able to walk with the stick. The movements were slightly painful and restricted. Systemic examination was unremarkable. All the biochemical parameters were within normal limits. Patient was subjected to plain bilateral hip joints anteroposterior and frog leg oblique views X-ray examination. Plain skiagram revealed the radiolucencies in both the femoral heads with more on left side. There was also mild subchondral sclerosis observed (Figures 1 and 2).
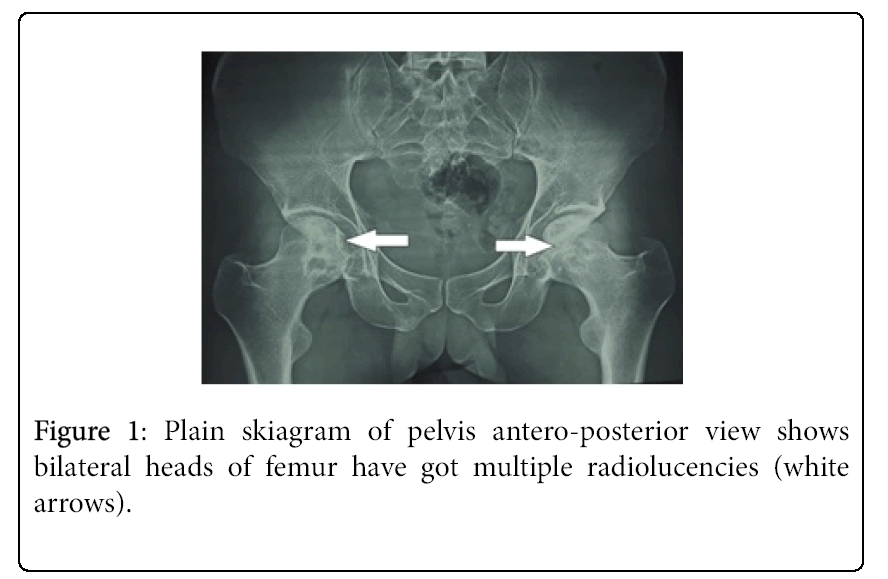
Figure 1: Plain skiagram of pelvis antero-posterior view shows bilateral heads of femur have got multiple radiolucencies (white arrows).
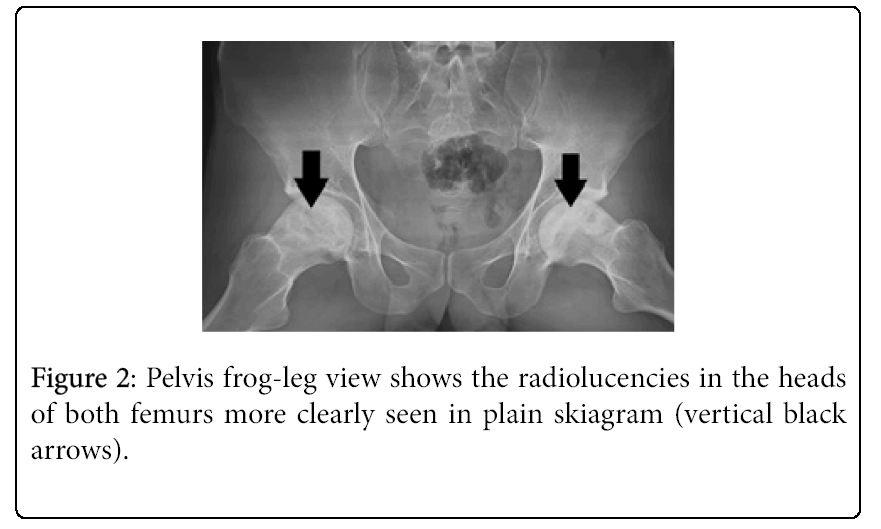
Figure 2: Pelvis frog-leg view shows the radiolucencies in the heads of both femurs more clearly seen in plain skiagram (vertical black arrows).
Plain CT examination confirmed the findings and underlying detailed anatomy of the joints in axial sections (Figures 3a and 3b) and 3D reformatted reconstruction (Figures 4a and 4b).
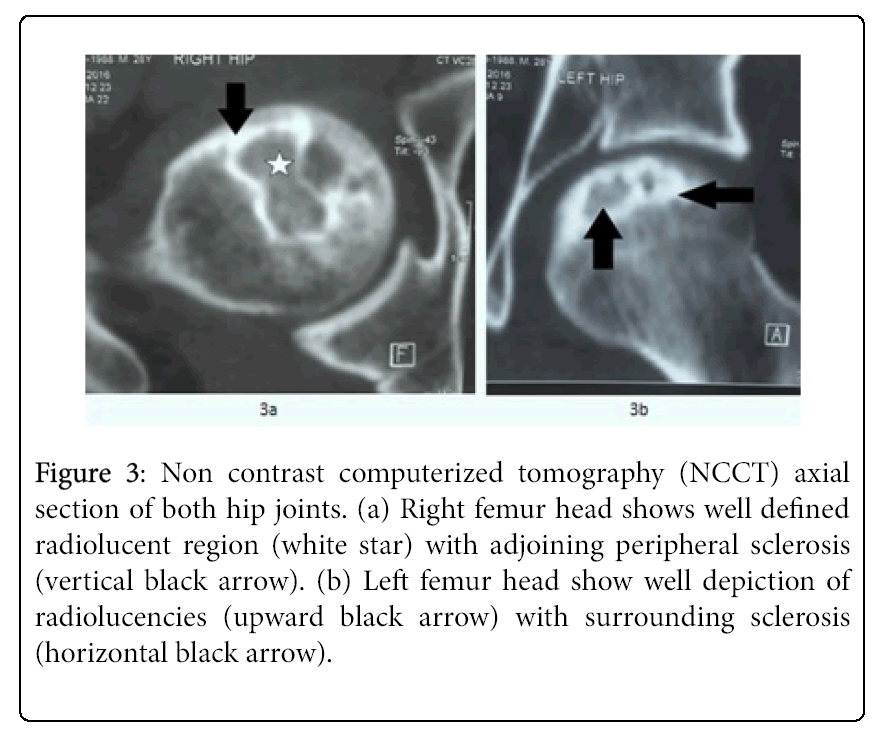
Figure 3: Non contrast computerized tomography (NCCT) axial section of both hip joints. (a) Right femur head shows well defined radiolucent region (white star) with adjoining peripheral sclerosis (vertical black arrow). (b) Left femur head show well depiction of radiolucencies (upward black arrow) with surrounding sclerosis (horizontal black arrow).
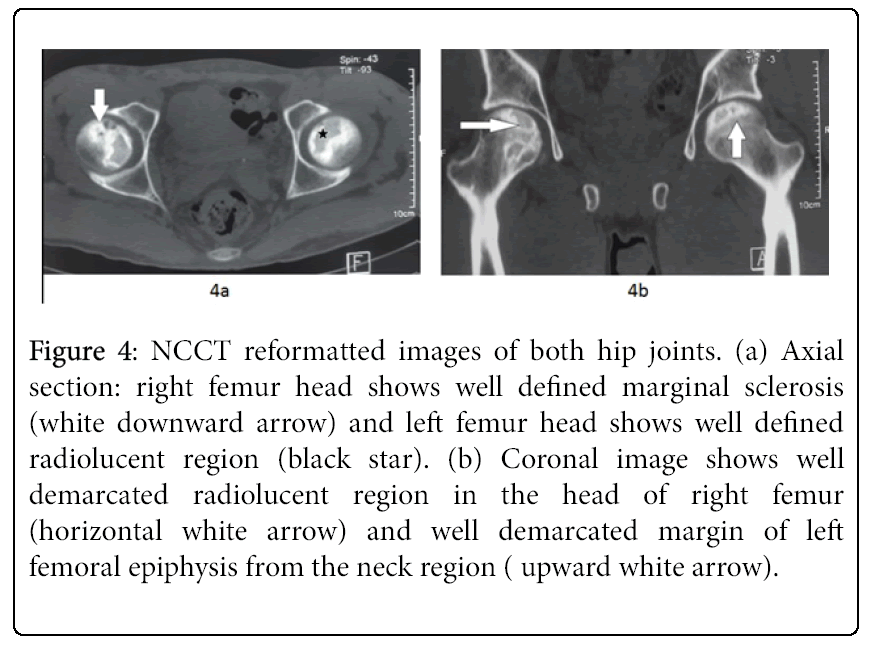
Figure 4: NCCT reformatted images of both hip joints. (a) Axial section: right femur head shows well defined marginal sclerosis (white downward arrow) and left femur head shows well defined radiolucent region (black star). (b) Coronal image shows well demarcated radiolucent region in the head of right femur (horizontal white arrow) and well demarcated margin of left femoral epiphysis from the neck region ( upward white arrow).
Plain as well as contrast enhanced MRI were carried out. MRI revealed the enhancement in both femoral heads with left side more affected (Figures 5a and 5b).
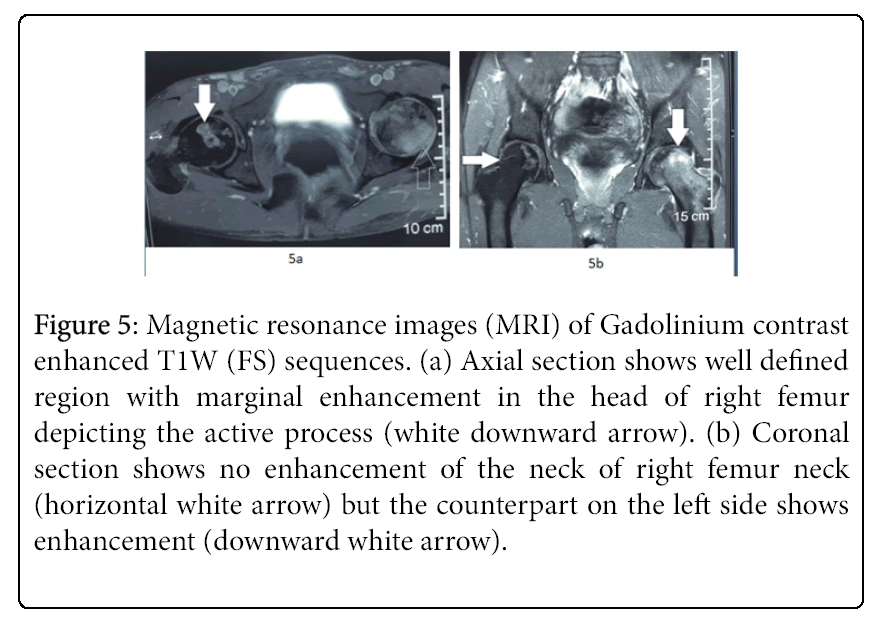
Figure 5: Magnetic resonance images (MRI) of Gadolinium contrast enhanced T1W (FS) sequences. (a) Axial section shows well defined region with marginal enhancement in the head of right femur depicting the active process (white downward arrow). (b) Coronal section shows no enhancement of the neck of right femur neck (horizontal white arrow) but the counterpart on the left side shows enhancement (downward white arrow).
The patient has been kept under observation and will be planned for prophylactic core decompression with bone graft of left side first and then to the right side.
AVN is also called as aseptic necrosis or osteonecrosis. All these changes take place following the ischemic state of the bone [1]. Whenever the head of femur vascular necrosis takes place there is always physical disability involved leading immediate attention for the management [2]. Non traumatic type of AVN is difficult to diagnose in the initial stages because of no special history [3]. This occurs in people between 30 to 50 years of age. This is called as Legg-Calve-Perthes syndrome. Males are affected four times more than females. 50% cases are bilateral and it is rare in the extreme of the age. There is pain in the groin radiating to thigh or buttocks and the gait is antalgic. AVN of femoral head has got great diagnostic as well therapeutic challenge because of its impact on the afterwards disability [4]. This requires total hip replacement within three years of the diagnosis as there is collapse of the particular joint within two years of the starting process. The patient may be having asymptomatic pain with gradual increase in its intensity. The diagnosis is delayed because of no positive signs of disease in plain radiography for the first three months as was in our present case. The patient starts limping in due course of time.
The pain may be relieved with rest in the beginning and aggravated by coughing or sneezing and at night time. Plain antero-posterior and frog leg views of the hip joint delineate the radiolucency in the femoral head with sub chondral sclerosis. This leads to the collapse in the form of crescent sign leading to degenerative changes and ultimately loss of joint space. Both the femoral heads must be assessed as the symptoms could be present in only affected side. Ficat and Arlet [5] proposed four stage system from Stage 1 – Stage IV with the advancement of the disease [5]. Steinberg [6] further proposed the staging to clarify the undergoing process into Stage I – Stage VI. First four stages were further divided on the basis of the involvement of the head of area into three categories as A (<15%), B (15-30%) and C (>30%) [6,7]. MRI is very sensitive in the diagnosis than even bone scan. This is the modality of choice where plain skiagram is normal. It has sensitivity of 97% and the specificity 98%. Bone marrow edema, acetabular collapse and comparing with other hip is of great importance in MRI. The findings can be picked up as early as five days after the vascular insult. T1W shows low signal with increased intensity in STIR images. Double line appearances in T2W images is the hallmark of the process as these depict demarcation between the ischemic and normal bone. This also helps in the follow up of post-operative cases. There is serpiginous line between 10 O’Clock and 2 O’Clock showing the necrotic and reparative zones. There is better outcome if the lesion is more on medial aspect and the size is less than one fourth of femoral head. Bone scan shows photopenic area of vascular insult and is better than plain radiographs. CT scan on the other hand assesses accurately the collapse of the head and amount of sclerosis with degenerative changes. Angiographic procedures are of only academic interest.
Management in these type of patient is very important as the disease will develop comorbidities. Physical therapy does not alleviate the underlying disease other than temporarily providing the relief. Other underlying causative factors like steroid use will require statin therapy for the management [8]. Alcoholic disorders have to be looked into and this require additional psychiatric counselling. Post traumatic AVN can also present in similar fashion. Surgical intervention is required for prophylactic and reconstructive purpose. Core decompressions with cancellous bone graft or vascular fibular graft are the procedures of the choice [9]. The reconstructive management depends upon the case to case basis as ultimately prosthesis is required either on one side or both the hips [10].
Idiopathic avascular necrosis of the femoral head involves a lot of morbidity with the passage of time and duration of underlying symptoms. The diagnosis should be picked up at the earliest possible time and both the femoral heads should be examined. The management has to be tailored as per the radiographic staging of the disease. The symptomatic treatment can make life comfortable but ultimately surgical management is the answer. Core decompression with bone grafting should be carried out with proper merits of the case. The delayed and chronic cases ultimately require prosthesis by hip replacement.