Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Case Report - (2014) Volume 3, Issue 4
A 14-year old girl with Rett syndrome was studied. The patient had roncopathy, sleepiness, decreased activity and performance, corrected kyphoscoliosis, obesity, retrognathia, ojival palate and dental malocclusion. Nocturnal polysomnography (PSG) showed a moderate obstructive and apparently central sleep apnea-hypopnea syndrome (SAHS) with associated hypoventilation, corrected by continuous positive airway pressure of 11 cm H2O. Respiratory monitoring in the awake state showed a characteristic pattern of episodes of hyperventilation with hypocapnia followed by central apnea and accompanying desaturations. We conclude that patients with Rett syndrome should be studied using PSG in order to rule out SAHS since multiple predisposing factors are often also present.
Keywords: Rett syndrome; Nocturnal respiratory pattern; Awakening respiratory pattern; Sleep apnea-hypopnea syndrome; Cardiorespiratory function; CPAP; Treatment
Rett syndrome (RTT) is a severe, progressive neurodevelopmental disorder that appears in early childhood and affects females almost exclusively. It is characterized by progressive cerebral atrophy, autism, manual stereotypes, dementia, acquired microcephaly, apraxia of gait and a tendency to suffer epileptic crises [1]. It has occasionally been described in association with sleep apnoea-hypopnoea syndrome (SAHS). We report the case of a 14-year old patient with RTT, studied from the respiratory point of view in the awake state and when sleeping using polysomnography (PSG), who was treated with continuous positive airway pressure (CPAP).
A 14-year old girl diagnosed at the age of 33 months as having RTT was seen in the Pneumology Outpatients’ Clinic due to suspicion of SAHS. Her parents reported snoring with pauses of apnoea during the night for several years which had become worse in the last 1-2 years.
At the same time the patient exhibited excessive sleepiness during the day, a decrease in her normal activity and attention at school together with an increase in weight. On physical examination, dental malocclusion and malposition, Mallampati IV, retrognathia and ojival palate were found.
Conventional diagnostic PSG was done during the first night followed by monitoring when the patient was awake the following morning. During sleep, there was an efficiency of 71.4%, 13.2 arousals/hour and destructuration of the sleep architecture, with a decrease in the percentage of deep sleep and REM stage (REM: 6%, stage 1: 17%, stage 2: 32%, stage 3-4: 45%), together with multiple central and obstructive respiratory events (predominantly hypopnoeas) which determined an apnoea-hypopnoea index (AHI) of 18.6 events/hour together with an oxyhemoglobin (SpO2) desaturation index of 26/hour,
minimum SaO2 of 82% and T90 (percentage of sleep time with oxygen saturation below 90% (T90) defined as the ratio between time in minutes with saturation values under 90% divided by the total sleep time of 100 minutes) of 22% associated to hypoventilation component. When the patient was awake, the ventilatory pattern was monitored for one hour, together with the analysis of end tidal expired CO2 (EtCO2, Nellcor™ N-85 Portable Pulse Oximetry Monitor with Microstream®). An irregular ventilatory pattern was seen with sudden changes in tidal volume and episodes of hyperventilation with hypocapnia reaching a mean EtCO2 of 20, followed by central apnoeas and SaO2 desaturations (Figure 1).
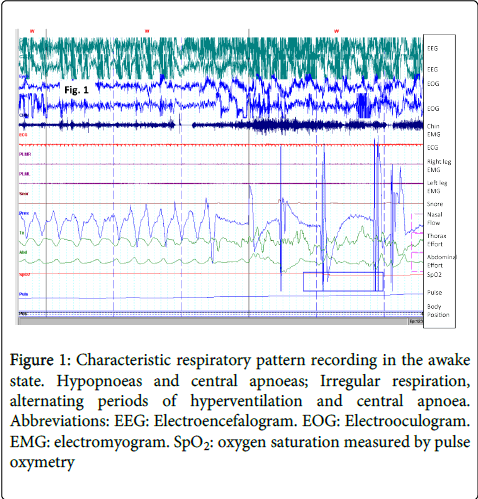
Figure 1: Characteristic respiratory pattern recording in the awake state. Hypopnoeas and central apnoeas; Irregular respiration, alternating periods of hyperventilation and central apnoea. Abbreviations: EEG: Electroencefalogram. EOG: Electrooculogram. EMG: electromyogram. SpO2: oxygen saturation measured by pulse oxymetry
During the first half of the second night, adjustment was made with non-invasive ventilation using BIPAP® with values of IPAP of 12 cm H2O and EPAP of 3 cm H2O. Both central and obstructive respiratory events were seen to persist as well as pathological desaturations (Figure 2A). During the second half of the night, a recording was made of the CPAP levels which eventually reached 11 cm H2O and the respiratory events practically ceased, with the sleep pattern returning to normal together with the number of arousals and the SaO2 levels remained above 90% (Figure 2A and B). Nocturnal CPAP was maintained at 11 cm H2O using a nasal mask. At subsequent check-ups, good tolerance and adaptation were found, together with an improvement in the patient’s sleepiness during the day, degree of physical activity and performance at school.
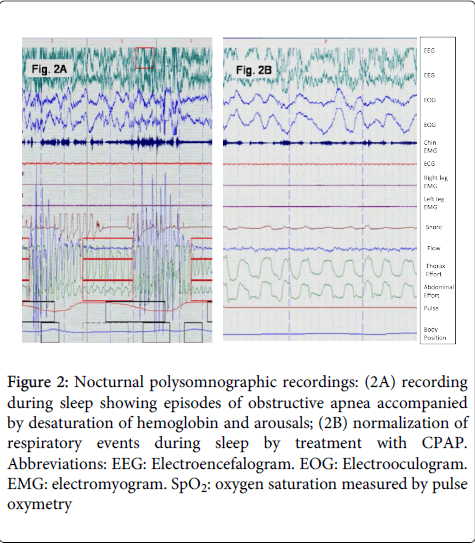
Figure 2: Nocturnal polysomnographic recordings: (2A) recording during sleep showing episodes of obstructive apnea accompanied by desaturation of hemoglobin and arousals; (2B) normalization of respiratory events during sleep by treatment with CPAP. Abbreviations: EEG: Electroencefalogram. EOG: Electrooculogram. EMG: electromyogram. SpO2: oxygen saturation measured by pulse oxymetry
The genetic basis of RTT consists of mutations or deletions of methyl-CpG-binding protein 2 (MeCP2) whose gene is located in the long arm of chromosome X (Xq28), which are described in 90% of the cases [1]. This protein acts in particular in the hypocampus, cortex and cerebelum, and plays an important part in modulating the activity of genes and neurons involved in social interactions. The phenotype spectrum of its mutation includes mental retardation, epilepsy, Angelman-like phenotype syndrome and autism.
RTT implies an alteration of the interactions between the autonomic, peripheral and central nervous systems, and hypofunction of neurotransmitters (glutamate, gamma-aminobutyric acid (GABA), serotonine or noradrenaline) has been postulated [2]. It has been suggested that altered expression of neuropeptide antagonists, such as substance P and methionine-encephalin, is the cause of the respiratory manifestations in this disease [2].
Patients show an immature sleep pattern with no reduction in the total sleep time and daytime sleep seen in normal children [3]. Periodic respiratory dysfunction, electroencephalographic (EEG) alterations, spasticity, eating disorders, retarded growth, cardiac disautonomy, constipation, dystonia and scoliosis are quite common. The degree of kyphoscoliosis tends to increase with growth, and at an age of around 16-20 years 43% of patients exhibit a severe degree or have already been operated on.
The respiratory pattern is characteristic, as it was in our patient. After a period of normal respiration with no hypoxemia, there is a period of hyperventilation with hypocapnia and prolonged periods of central apnea of up to 19 seconds accompanied by Valsalva manoeuvres and hypoxemia, with SaO2 desaturations of up to 50% [4]. Respiratory alkalosis and hypoxemia reported as a result of hypoventilation may contribute to brain damage [5]. Furthermore, hyperventilation is accompanied by an increase in blood pressure with an increase in vagal tone and decrease in heart rate. EEG shows theta 3-5Hz waves throughout the cerebral cortex [6]. Other respiratory patterns have also been described such as those of Biot or Cheyne-Stokes, being more severe the younger the child [7]. These events do not occur during sleep, when the respiration is regular during both NREM and REM sleep; the efficiency and architecture of sleep are maintained, with only lower values of SaO2 in the REM stage described, but these are within the normal range [8]. Therefore, patients with RTT do not have alterations in the system controlling ventilation and the alterations described when the patient is awake are due to an abnormality in the cortical influence of ventilation and alterations in the autonomic control of respiration. It has also been suggested that there is an autonomic alteration, due to longer QT intervals and a decrease in heart rate variability, with a greater incidence of sudden death [9].
Few studies have been done on respiratory disorders during sleep. Rohdin et al. [10] monitored 12 RTT girls in their home showing apnoea, hypoventilation or shallow breathing in wakefulness, but the authors did not specified the type of respiratory alteration during sleep. Weese-Mayer et al. [11] studied 47 girls with RTT and determined that, although the breathing and heart rate appeared more regular during the night, some irregularities could appear at home. Recently d’Orsy et al. [12] studied a 3-year-old girl showing central apnoeas not only during awake, but also during sleep. Some authors hypothesize that breathing dysregulation in RTT results from disturbances in mechanisms that modulate the respiratory rhythm, acting either alone or in combination with more subtle disturbances in rhythm and pattern generation [13].
Our patient could have had nocturnal hypoventilation due to her kyphoscoliosis despite the fact that it had been corrected, but what was most striking were the clinical symptoms suggesting SAHS and the predisposing factors. Normalization of the ventilatory pattern by means of CPAP and not BIPAP® supports the fact that the hypoventilation component was due to the severity of the obstruction of the upper airway, which was the main cause of SAHS and the apparently central apnoeas were obstructive in origin, normalizing the nocturnal respiratory pattern with CPAP. In these cases only the response to CPAP distinguishes the true central apneas from obstructive apneas. In our case, it is possible that the espiratory airway pressure (EPAP) applied during the titration was insufficient to overcome the obstructive apneas and had gotten a good response to the BIPAP increasing the EPAP. If respiratory events had persisted, switching to adaptive servo ventilation could be the best treatment option [14]. Given that SAHS in the child population may present neuropsychiatric alterations such as hyperactivity, attention deficit, etc., these may cause the neurological symptoms of the disease to worsen even more, as occurred in our patient.
We conclude that to perform a nocturnal polygraphic recording with monitorization of respiratory variables in patients with RTT may be essential for diagnosis and treatment of SAHS, which may be associated with RTT since there are many potential predisposing factors. Daytime monitorization of the ventilation pattern may reveal characteristic alterations that appear when the patient is awake.