Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2014) Volume 2, Issue 5
Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition of accelerated platelet consumption caused by antiplatelet autoantibodies, and glycoprotein (GP)IIb/IIIa is one of the major target antigens recognized by platelet-reactive CD4+ T cells. Patients with ITP often have few bleeding symptoms despite very low platelet counts, suggesting that ITP platelets are highly functional. Several factors may contribute to the prothrombotic state in ITP. We investigated the effect of thrombopoietin (TPO)-receptor agonist (RA) on the procoagulant state in ITP with or without anti-GPIIb/IIIa antibody. Long-term administration of eltrombopag resulted in stabilization of platelet numbers in many patients. On the other hand, when the analysis was carried out according to the presence of GPIIb/IIIa autoantibodies, the increase in platelet counts in ITP patients was more significant with than without anti-GPIIb/IIIa autoantibodies. In addition, there were significant differences in PDMP between cases in which platelet count was above or below 100x109/l. Our observation is possible to reflect the role of the anti-GPIIb/IIIa antibody in ITP patients who received TPO-RA.
Keywords: Itp; Anti-GpIIb/IIIa Antibody; Eltrombopag; Procoagulant State; PDMP
Immune thrombocytopenia (ITP) is an acquired hemorrhagic condition of accelerated platelet consumption caused by antiplatelet autoantibodies [1,2]. Autoreactive B- and T-cells play an important role in antibody generation in patients with ITP [3], and glycoprotein (GP)IIb/IIIa is one of the major target antigens recognized by platelet-reactive CD4+ T cells [4-6]. Bleeding risk in patients with ITP is increased, with platelet counts less than 20 or 30×109/l being a trigger for treatment [7]. However, patients with ITP often have few bleeding symptoms despite very low platelet counts, suggesting that ITP platelets are highly functional [8]. Several factors may contribute to the prothrombotic state in ITP [9]. The production of cell-derived MP and increased levels of some coagulation factors have recently been reported as possible causes of increased thrombotic risk in ITP patients [10]. Recently, Román et al [11] reported that thrombopoietin (TPO)-receptor agonist (RA) treatment increased platelet count but did not ameliorate their function and did not change the plasma- and microparticle (MP)-associated procoagulant state of ITP patient responders to this therapy. However, effect of TPO-RA on the procoagulant state in ITP with or without anti-GPIIb/IIIa antibody has remained poorly understood. In the present study, we have investigated this issue.
Patients
The study group included 42 patients with adult and chronic ITP who had already received steroids or other therapies (Table 1). Between September 2010 and April 2012, patients were selected from among those admitted to our hospital for the treatment of ITP. The study protocol was approved by the Institutional Review Board of our institution and written informed consent was obtained from each patient prior to the start of the trial. Participants were at least 18 years of age, had at least a 6 month history of ITP, had received at least one previous treatment for ITP. Patients receiving maintenance immunosuppressive regimens, primarily glucocorticoids, were eligible if the dose had been stable for at least 1 month. Patients with the following conditions were excluded: secondary immune thrombocytopenia (e.g. virus associated, antinuclear antibody positive, systemic lupus erythematosus and antiphospholipid antibody syndrome), congestive heart failure, arrhythmia, or myocardial infarction within 3 months before enrollment; women who were nursing or pregnant were also excluded. ITP patients were divided into 2 groups (TPO-RA-exposed: 18 patients; unexposed: 24 patients). TPO-RA-exposed patients were chosen by wrong reactivity for steroids or other therapies, or strong bleeding symptoms, since TPO-RA is not permitted to be used as a first line drug in Japan. Therefore, TPO-RA-exposed patients were chosen according to low platelet counts (<30×109/l) two times during steroid therapy. TPO-RA-unexposed patients were chosen by stable platelet counts (>30×109/l) during steroid therapy or nontherapy.
| TPO-RA (+) | TPO-RA (-) | p value | |
| Variables | 18 | 24 | |
| Gender(male/female) | 6 /12 | 4 / 20 | |
| Age, y | 68 ± 7 | 52 ± 6 | <.01 |
| Platelet counts×109/l | 24 ± 12 | 70 ± 29 | <.001 |
| T-BIL, mg/dL | 0.9 ± 0.4 | 0.7 ± 0.3 | N.S. |
| LDH, U/l | 250 ± 38 | 194 ± 36 | <.05 |
| CRP, mg/ml | 0.12 ± 0.12 | 0.13 ± 0.21 | N.S. |
| Prior therapy | |||
| Immunosup. agent (%) | 4 / 18 (22.2) | 7 / 24 (29.2) | N.S. |
| IVIG (%) | 2 / 18 (11.1) | 3 / 24 (12.5) | N.S. |
| Splenectomy (%) | 2 / 18 (11.1) | 2 / 24 (8.3) | N.S. |
Table 1: Comparison of clinical and laboratory data for patients with ITP. Data are shown as mean ± SD. N.S: not significant, TPO-RA(+): eltrombopag-exposed group, TPO-RA(-): unexposed group, T-BIL: total bilirubin, LDH: lactate dehydrogenase, CRP: C-reactive protein Immunosup. agent: immunosuppressive agent IVIG: intravenous immunogloburin
Study design
Doses of eltrombopag ranging from 12.5 mg to 50 mg were administered daily. The drug dose was gradually multiplied when platelet counts responded to eltrombopag. We investigated the change of platelet counts and platelet-derived MP (PDMP) in patients with ITP who were administered eltrombopag over 50 weeks. Furthermore, patients were split into two groups retrospectively, either with anti-GPIIb/IIIa antibody or not.
Measurements of PDMP
Blood from 15 normal subjects was used as a control. Blood samples from patients and controls were collected into tubes with sodium citrate or tubes without anticoagulant. Blood samples were allowed to clot at room temperature for a minimum of 1 hour. Serum or citrated plasma was isolated by centrifugation for 20 minutes at 1,000 g (4ºC) and stored at -30ºC until analysis. PDMP were detected by ELISA in the plasma of ITP patients [12].
Measurement of antiplatelet antibodies
The specific antigen of the anti-GPIIb/IIIa antibody was examined using the PakAuto system (GTI Diagnistic, Inc., Waukesha , WI, USA) [13]. In brief, the patient’s serum was added to the microwell, which fixed three platelet-glycoprotein (GP) such as GPIIb/IIIa, GPIb/IX and GPIa/IIa. Next, uncombined antibodies were removed by washing. ALP-labeled antihuman globulin (IgG/A/M) reagent was added and left to incubate. This was then flushed with uncombined enzyme-labeling antihuman IgG/A/M antibody, and p-nitrophenyl phosphate substrate was added. After 30 min incubation, reaction was stopped by the addition of NaOH solution. The absorbency of the coloring material was measured using the absorbency total. The absorbency of the positive control was 100% that of the negative control 0%, and the patient’s samples were converted to a percentage with respect to the absorbency of the positive control. The non-specific reaction area was decided from the blank result, and the following criteria were set: 0-30%: (-); 31-60%: (+); 61-100%: (2+); and more than 101%: (3+).
Statistics
Data are expressed as the mean ± SD and were analyzed by two- factor ANOVA for repeated measures as appropriate. Between-group comparison of values was made with the Newman-Keuls test and Scheffe’s test. P-values less than 0.05 were considered statistically significant. Analysis was performed using the StatFlex program (ver. 6).
When baseline values before the treated period were compared between the TPO-RA-exposed and unexposed groups, there were significant differences in age (p<0.01), platelet counts (p<0.001) and lactate dehydrogenase (p<0.05) (Table 1). In addition, there were no significant differences in frequencies of prior therapy such as immunosuppreressive agent, IVIG or splenectomy(Table 1). The response rate of the TPO-RA was 77.8% (14/18). Long-term administration of eltrombopag resulted in stabilization of platelet numbers in many patients (Figure 1). On the other hand, when the analysis was carried out according to the presence of GPIIb/IIIa autoantibodies, the increase in platelet counts in ITP patients was more significant with than without anti-GPIIb/IIIa autoantibodies (Figure 2). In addition, there were significant differences in PDMP between cases in which platelet count was above or below 100×109/l (Figure 3).
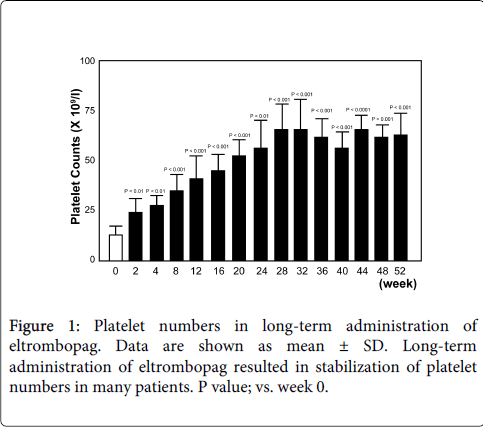
Figure 1: Platelet numbers in long-term administration of eltrombopag. Data are shown as mean ± SD. Long-term administration of eltrombopag resulted in stabilization of platelet numbers in many patients. P value; vs. week 0.
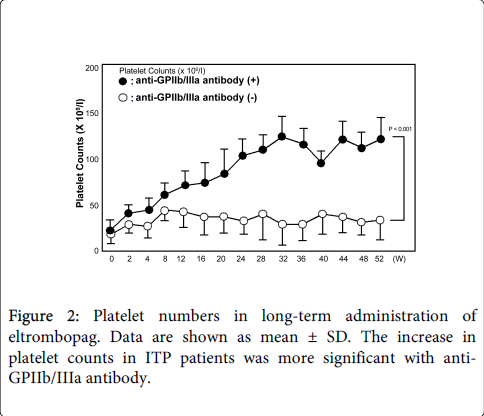
Figure 2: Platelet numbers in long-term administration of eltrombopag. Data are shown as mean ± SD. The increase in platelet counts in ITP patients was more significant with anti- GPIIb/IIIa antibody.
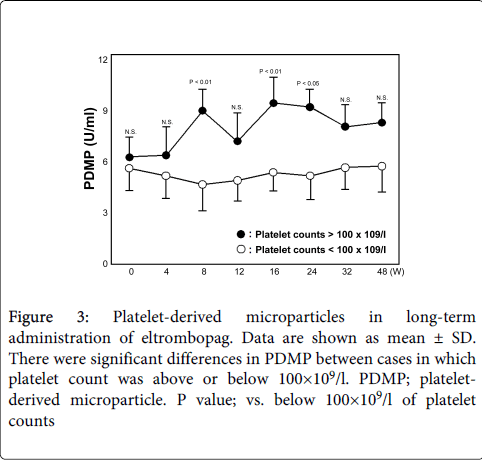
Figure 3: Platelet-derived microparticles in long-term administration of eltrombopag. Data are shown as mean ± SD. There were significant differences in PDMP between cases in which platelet count was above or below 100×109/l. PDMP; plateletderived microparticle. P value; vs. below 100×109/l of platelet counts
Several reports have shown that ITP patients have a higher risk of suffering venous thromboembolism [14,15]. In addition, based on data from TPO-RA clinical trials, an increase in thrombotic risk in patients treated with these therapies cannot be excluded [16]. Thus, it is very important to investigate the effect of TPO-RA on the procoagulant state in ITP patients who received long-term administration of TPO-RA. Furthermore, it is possible that TPO-RA contributes to the development of platelet activation and participates in thrombus formation, as TPO can cause platelet activation [17]. Román, et al. [11] suggested that MP in ITP patients were increased compared to healthy controls, but no change in MP existed before or after TPO treatment. Our results partially support the report by Román et al. [10]. Although our report is limited as we investigated only PDMP but not other types of MP such as tissue factor- or phosphatidylserine-exposing MP, we suggest that PDMPs may be increased after TPO-RA treatment by the the actions of anti-platelet antibodies or reactivity against TPO-RA. Román, et al. [10] also reported that the surface expression and activation of the fibrinogen receptor on platelets from ITP patients was reduced, and that a relationship existed between apoptosis and platelet activation ability. By contrast, we did not observe a change in the platelets of ITP patients. Our observation is possible to reflect the role of the anti-GPIIb/IIIa antibody in ITP patients who received TPO-RA. However, many unresolved problems remain in ITP patients treated with long-term TPO-RA. Therefore, further investigation is necessary to better elucidate the potential involvement of TPO-RA in thrombus formation.