Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2015) Volume 3, Issue 3
Study background: To describe a novel technique, using the Universal Clamp (Zimmer Spine, Bordeaux France), for short-segment fixation in patients with severe osteoporosis and vertebral body fracture.
Methods: Consecutive patients with one-level osteoporotic vertebral fracture (OVF) that underwent short-segment (one-level above and one-level below) fusion surgery were retrospectively reviewed. Both radiographic and clinical evaluations were analyzed, and compared pre- and post-operation. Step-wise surgical techniques are described in detail.
Results: Five patients, including one male and four females, who had one level of OVF in the thoraco-lumbar spine were enrolled. The mean age was 67.6 ± 4.1 years, and the average preoperative T-score was -2.2 ± 1.5. The average follow-up was 10.6 months. Post-operatively, all patients had significant clinical improvement after the operation. Also, the mean Cobb’s angle (6.2 ± 4.3 degrees) was significantly improved compared to pre-operation (13.6 ± 8.1, p= 0.039). Furthermore, there were no complications, implant failures (i.e. screw loosening, pullout, breakage, or dislodgement), or loss of deformity correction.
Conclusion: Using the Universal Clamp to reinforce the short-segment pedicle screw fixation is a viable alternative for patients with osteoporosis and vertebral fracture. Successful restoration of spinal alignment and symptoms relief can be achieved. However, more long-term evaluations and a larger number of patients are required to corroborate this option.
<Keywords: Universal clamp; Short-segment fixation; Osteoporotic vertebral fracture
Posterior instrumentation with pedicle screw-based constructs have been commonly used in the surgical management of thoracolumbar spinal deformity [1]. There are reports of screw loosening or pull out, causing kyphotic deformity or fracture of vertebral bodies, even in patients with normal bone quality [2,3]. In patients with osteoporosis, achievement and maintenance of deformity correction are even more challenging [4]. Therefore, various strategies were developed to increase the purchase of pedicle screws, including placement of longer screws with a larger diameter, bicortical bone purchase, alteration of the shape of the screw, [5] and augmentation with poly-methyl-methacrylate (PMMA) or calcium phosphate cements [4,6,7]. For the osteoporotic vertebral fracture (OVF), some surgeons have advocated placement of pedicle screws in at least two segments above and below the fractured level [4,8].
In recent years, there have been reports about using Universal Clamps (Zimmer Spine, Bordeaux France) for deformity correction [9- 13]. The Universal Clamp connects the lamina to the rod, like a sub laminar wiring, and thus reinforces the screw-rod construct. The device was initially designed to substitute pedicle screws by using the polyester band and the metal clamp, tightened with an intended pressure, thus “holding” the pedicle screw-rod construct in place. In combination with regular pedicle screws, successful correction of adult and adolescent deformity has been reported a few times [9-13]. However, it has never been reported in the treatment of osteoporotic spine.
The aim of this study was to describe a novel technique for a less invasive surgery of OVF. Using the Universal Clamps to reinforce the short-segment instrumentation, placement of pedicle screws one level above and below, successfully restored stability in patients of OVF. To date, no other reports have demonstrated the viability of Universal Clamps in the management of osteoporosis.
The study enrolled 5 consecutive osteoporotic patients who had one vertebral body fracture, either compression fracture or burst fracture, with spinal canal compromise and symptoms/signs of compression in the thoracolumbar spine. They underwent laminectomy for decompression and posterior instrumentation with short-segment (i.e. one level above and one level below the fractured segment) fixation with pedicle screws. For each pedicle screw, a Universal Clamp was applied to connect the corresponding lamina to the screw-rod construct in the fashion of sublaminar wiring by artificial ligament. Patients with multiple segments of OVF, severe deformity requiring long-segment fixation, or pathological fractures due to metastatic tumors were excluded from this series.
Implant description
The Universal Clamp consists of three parts: one clamp, one locking screw, and one woven polyester band which contains a malleable lead at one end and preassembled to a pair of buckles at the other (Figure 1A). Before use, the Clamp is assembled by passing the malleable end through the slot of the Clamp, and the band is pulled until the Clamp reaches the buckle-end of the band.
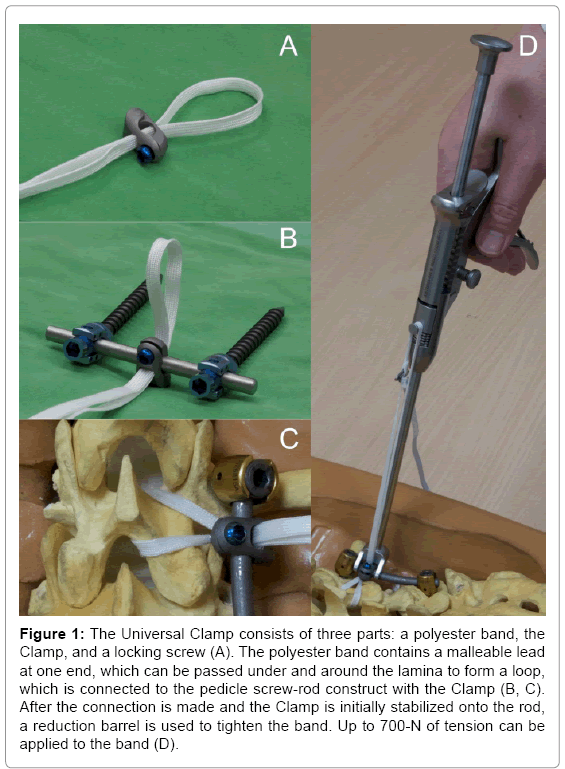
Figure 1: The Universal Clamp consists of three parts: a polyester band, the Clamp, and a locking screw (A). The polyester band contains a malleable lead at one end, which can be passed under and around the lamina to form a loop, which is connected to the pedicle screw-rod construct with the Clamp (B, C). After the connection is made and the Clamp is initially stabilized onto the rod, a reduction barrel is used to tighten the band. Up to 700-N of tension can be applied to the band (D).
Surgical technique
All operations were conducted with general anesthesia with patients placed in a neutral prone position with proper cushioning. Midline skin and fascial incisions were made with subsequent standard subperiosteal dissection for proper exposure. After confirming the indicated level, pedicle screws were placed one segment above and below the level of OVF with free-hand technique [14] (in thoracic segments) and under the assistance of fluoroscopy (in lumbar segments). Laminectomy was then carried out for the indexed level (i.e. the fractured vertebral body). Laminas reserved for application of the Universal Clamp were left intact while the surrounding soft tissue (e.g. ligamentum flava or epidural fat) was removed.
When the indicated lamina was ready, the malleable end of the polyester band was bent properly for the convenience of passage under the lamina. Care was taken when the band was passing below the lamina to avoid compression of the thecal sac or unintended durotomy. Once the band had been passed under the lamina and the desired length was reached, the malleable end was passed through the slot of the Clamp again, then both buckles, and with an opposite turn the malleable end was passed through one of the buckles for tightening. Thus an adjustable loop was made around and under the lamina (Figure 1B).
The rods were applied to connect each pedicle screw. The Clamp was then loaded onto the rod with the jaws open and medial orientation. Assemb ling the Clamp and rod was done by introducing the locking screw onto the Clamp for initial stabilization (Figure 1C). With a specific reduction tool, a 700-N of tension could be applied on the looping band (Figure 1D). After the intended tension was reached, the locking screw on the Clamp was tightened, and the excessive band outside of the Clamp-loop construct was removed (Figures 2,3).
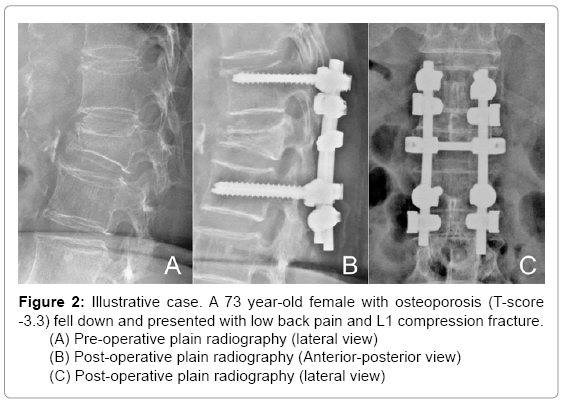
Figure 2: Illustrative case. A 73 year-old female with osteoporosis (T-score -3.3) fell down and presented with low back pain and L1 compression fracture.
(A) Pre-operative plain radiography (lateral view)
(B) Post-operative plain radiography (Anterior-posterior view)
(C) Post-operative plain radiography (lateral view)
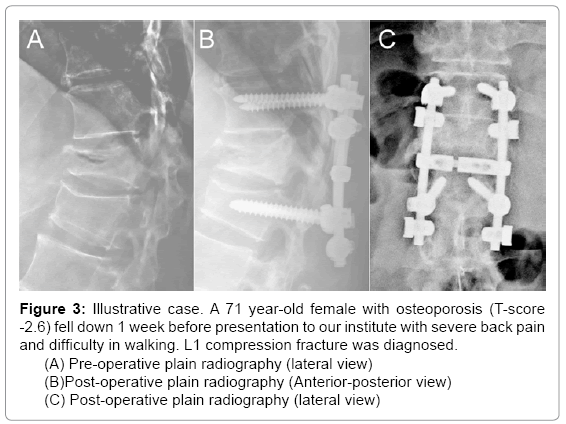
Figure 3: Illustrative case. A 71 year-old female with osteoporosis (T-score -2.6) fell down 1 week before presentation to our institute with severe back pain and difficulty in walking. L1 compression fracture was diagnosed.
(A) Pre-operative plain radiography (lateral view)
(B)Post-operative plain radiography (Anterior-posterior view)
(C) Post-operative plain radiography (lateral view)
Clinical and radiological evaluation
Clinical evaluation was carried out preoperatively and approximately 3, 12 and 24 months postoperatively as outpatients. Every patient received preoperative imaging, including plain radiography, CT scanning, MR imaging, and Dual-energy X-ray absorptiometry (DEXA) study. Follow-up imaging included standard plain radiography (anterio-posterior and flexion-extension views) at approximately 1, 3, 12 and 24 months after the surgery. The measurement was conducted with SmartIris analysis software (Taiwan Electronic Data Processing Co.)
Statistical analysis was performed with Excel software (Microsoft Inc.). A p value of 0.05 was considered statistically significant.
This study enrolled a total of five patients (Table 1) with a mean age of 67.6 ± 3.3 (64 - 73) years, and a mean preoperative T-score of -2.2. The average follow-up duration was 10.6 months with the longest follow-up to 17.3 months.
| No. | Age | Sex | Preop Cobb’s Angle |
Postop Cobb’s Angle |
Cobb’s Angle Correction |
|---|---|---|---|---|---|
| 1 | 73 | F | 16 | 6 | 10 |
| 2 | 71 | F | 15 | 3 | 12 |
| 3 | 64 | M | 22 | 13 | 9 |
| 4 | 65 | F | 15 | 7 | 8 |
| 5 | 65 | F | 0 | 2 | 2 |
| Mean± SD | 67.6± 4.1 | 13.6±8.1 | 6.2±4.3 | 7.4±5.5 p=0.039* |
F, female; M, male; Preop, preoperative; Postop, postoperative; SD, standard deviation
* Comparison between preoperative and postoperative Cobb’s angles.
Table 1: Demographic and clinical data.
All patients underwent surgical procedures as previously described and had uneventful recovery. Significant clinical improvement was observed in each patient. The average postoperative Cobb’s angle (6.2 ± 4.3 degrees) of the instrumented segments significantly improved compared to that of the preoperative one (13.6 ± 8.1 degrees, p= 0.039, paired-T test). The mean correction in Cobb’s angle was 7.4 ± 5.5 degrees (Table 1). There were no peri-operative complications or newly onset neurologic deficits postoperatively. No screw loosening or screw pullout was noticed during the period of follow-up.
This is the first report describing the application of Universal Clamps to prevent the pedicle screws from pulling out in severe osteoporotic patients. This study therefore demonstrates the application of the Universal Clamp in the treatment of OVF, with the longest follow-up of 17.3 months.
The surgical decision was made based on the necessity of surgical decompression and biomechanical design of the instrumentation. The short-segment screw-rod construct was reinforced by sublaminar wiring with polyester artificial ligaments. The short construct was thus securely tightened to the corresponding lamina at each of the four pedicle screws. These Universal Clamps connected lamina to the rod, thus making the entire screw-rod construct integrated into the bony structures for stabilization. This maneuver, like the locking plate system, tremendously increased the strength of fixation. With these characteristics, the intention of the surgery was to avoid longterm complications (e.g. screw pull-out, junctional kyphosis, and adjacent compression fracture). Significant clinical improvement was observed in every patient. Furthermore, there were no surgical complications, no implant failure (i.e. screw loosening, pullout, breakage, or dislodgement), or loss of deformity correction. Even though percutaneous vertebroplasty may have been a less invasive approach to treat compression fracture, it provides less advantage in decompression and restoration of the vertebral heights in comparison to posterior instrumentation, and the differences between these 2 surgical methodologies had been demonstrated in several studies [15- 18].
Posterior instrumentation of pedicle screw-based implants had been frequently used in the treatment of vertebral fractures with deformity: however, the optimal fusion length is still in discussion [15,19-22]. Short-segment fixation (one level above and below the injured vertebrae) offers advantages of lesser exposure, shorter operation time, less blood loss, and less compromise of spinal motion, etc. However, reports have been made on implant failure and even re-kyphosis at the incidence of 9-54% [6,19,23,26]. To avoid such complications and achieve proper correction of deformity in osteoporotic spines is even more challenging. Several adjunct surgical strategies have been proposed, such as bicortical purchase of the pedicle screws, alteration of the shape or diameter of the screws, transpedicular augmentation of vertebral body with PMMA or calcium phosphate cements [4,6,7,24]. Besides these methods, other authors have advocated increasing the fusion length to at least an additional level (two levels above and below the fractured segment) to enhance stability and efficacy of reduction of deformity [24,27-30].
During the past decade, the use of Universal Clamps for correction of thoraco-lumbar deformity has been increasingly reported [9-13]. With the aforementioned surgical technique, the Universal Clamp acted as a polyester band passing under the lamina, and was connected to the rod by a clamp. With the low-profile nature of the band and greater contact surface with the lamina compared with wiring, the Universal Clamp could distribute the stress over a larger base and provide better stability [4,10].
Several studies have demonstrated the safety and efficacy of such a device [4,9,11,12]. In 2009 a biomechanical study conducted by Hongo et al. [4] suggested that the Universal Clamp may have provided more predictable fixation in osteoporotic spine and was less likely to cause neural damage than the sublaminar wiring technique. Jouve et al. [10] demonstrated the efficacy of progressive reduction of deformity with this device and reduced risk of laminar fracture and neurologic complications. The ability to correct deformity with the Universal Clamp in conjunction with pedicle screw-based systems was demonstrated in a study by Mazda et al.[12] The result suggested the Universal Clamp technique was safe, with reduced operation time, blood loss and radiation exposure, while providing superior sagittal correction and equivalent coronal/axial correction compared to the best reported results on all-screw or other hybrid constructs. In 2012 the same study group conducted another series in which they used this device to prevent screw pullouts in the treatment of thoraco-lumbar fractures in skeletally immature patients with short-segment posterior fixation and anterior strut grafting [32].
The limitation of the current series would be the small case numbers due to the novel development of such application and late introduction to our institute. More long-term evaluations and more patient numbers are necessary for corroboration of this technique.
Short-segment fixation with reinforcement by Universal Clamp is a viable strategy in the management for deformity caused by vertebral fractures in patients with severe osteoporosis. Improvement of symptoms and reduction of deformity could be safely achieved without long constructs. However, these findings need to be corroborated by larger-scale clinical investigations and longer follow-up.