Gynecology & Obstetrics
Open Access
ISSN: 2161-0932
ISSN: 2161-0932
Research Article - (2017) Volume 7, Issue 7
Aim: Ovarian cancer (OC) occurs due to genetic alterations and mutations in BRCA gene. The aim of the study is to assess the frequency of genetic alterations that persist in Ashkenazi founder mutation BRCA1, 185delAG in patients with ovarian cancer from South Indian origin.
Materials and Methods: A total of 100 ovarian cancer patients and an equal number of control subjects were included in the present study. Screening of 185delAG mutation BRCA1 gene was carried out by ARMS PCR followed by agarose gel electrophoresis. Statistical analysis was applied to test for the significance of the results obtained.
Results: The genotype distribution of WW, WM, MM showed a significant difference between the two subjects, 95%, 4% and 1% in controls and 52%, 36% and 12% in cases respectively. An increased frequency of homozygotic mutant genotypes (MM) were found in patients compared to controls. Similarly, a significant difference in the distribution of M allele in cases and control subjects (W v/s M: χ2 P<0.0001, OR 18.06, 95% CI 6.31-51.65) was observed.
Conclusion: The demographic details of the patients and controls revealed that females of age greater than 40 years are associated with high risk of ovarian cancer. The postmenopausal women have a very high susceptibility to OC (6.5 times riskier). Therefore, 185delAG mutation BRCA1 has a possible association in the etiology of ovarian cancer.
Keywords: BRCA1; 185delAG mutation; Ovarian Cancer
Ovarian cancer (OC) is the most common forms of hereditary cancer in women and is the leading cause of death by gynecological malignancy. It has a hostile phenotype and a relatively poor prognosis. More than two thirds of patients were showing late stage disease [1,2]. It is predominantly a disease of postmenopausal women and has an overall 5-year survival of less than 30% [3]. Earlier studies indicate that hereditary cancers constitute 5%-10% and may be up to 14% [4,5] epidemiologic and molecular genetics analyses indicate that about 10% of all epithelial ovarian carcinomas are associated with autosomal dominant genetic predisposition, conferred primarily by inherited mutations in BRCA1 or BRCA2, they account for >90% of hereditary cancers. In general population the frequency ranges between 2-12% and 2-6% respectively [6]. The cumulative life time risk of developing epithelial ovarian carcinoma ranges from 20%-30% [7]. BRCA1 cloned in 1994 and 2 in 1995 both are very large genes most known mutations lead to premature termination of protein, leading to loss of tumor suppression [8]. Mutations in BRCA1 are present in approximately onehalf of the early-onset breast cancer families and 80% of the early-onset breast and ovarian cancer families [9] whereas BRCA2 mutations are believed to account for a comparable percentage of inherited breast cancer cases [10]. Both the genes are detrimental and acts as a sensor for DNA damage [11,12] hence resulting in defects in DNA repair, transcription, abnormal centrosome regulation, impaired spindle check point and chromosome damage. In view of the above the present study is aimed to evaluate the role of the founder mutation in the etiology of ovarian cancer.
Study population
A total of 200 individuals were included in the present study. 100 clinically and histopathologically confirmed ovarian cancer patients from Yashoda Hospital, Secunderabad during the years 2012-14 and an equal number of age matched healthy control subjects were also incorporated for comparative studies. A structured proforma was used to seek information on dietary habits, smoking, alcohol consumption, family history etc. Written informed consent was obtained from all the subjects. The study was also approved by our Institutional Ethical committee.
DNA isolation
Five ml of venous blood was drawn from each individual in EDTA vacutainers. Genomic DNA was isolated from whole blood using the salting out method [13].
Mutation analysis of 185delAG
The mutation of 185delAG was analyzed based on Amplification Refractory Mutation System-Polymerase Chain Reaction (ARMSPCR). The BRCA1 185delAG exon 2 primers are as follows: forward primer, 5’- GGTTGGCAGCAATATGTGAA-3’ (P1), Wild-type reverse 5’-GCTGACTTACCAGATGGGACTCTC-3’ (P2) and Mutant reverse5’-CCCAAATTAATACACTCTTGTCGTGACTTACCAGAT GGGACAGTA-3’ (P3). A 335 base pair region for wild type and 354 base pair region for mutant type was targeted for amplification. The optimized reaction conditions consisted of 25 mg of genomic DNA in a reaction volume of 20 μl of reaction mixture consisting of 10 × PCR reaction buffer (10 mM Tris-HCl, pH 8.3, 50 mM KCl, 10 μg/ml gelatin), 3.25 mM MgCl2, 0.2 mM dNTPs, and 3 U Taq DNA polymerase (Roche, Penzberg, Germany), 2.0 μM for P1 and P3, 0.4 μM for P2. The cycling conditions were as follows: an initial denaturation at 94°C for 4 minutes, followed by 35 cycles at 94ºC for 30 s, 57.3° C for 30s and 72°C for 45s. The final extension step was at 72°C for 10 min.
The amplified products were electrophoresed on an agarose gel (2.0%) stained with ethidium bromide. The presence of 335 bp band indicates wild type and 354 bp band indicates mutant type based on 100–base pair ladder.
Statistical analysis
The distribution of BRCA1 185delAG mutation and allele frequencies in healthy and ovarian cancer group were analyzed by Chi-square. Odds ratio (OR) and 95% confidence intervals (95% CI) were also assessed. Differences among subject groups in clinical characteristics were analyzed with Fisher’s two-tailed exact tests. Mutation frequencies were tabulated by direct counting and allele frequencies estimated from the observed number of mutations.
The study population consist of 100 Ovarian cancer patients, comprising 32 familial and 68 sporadic cases including 100 agematched controls were screened for the presence of 185delAG of BRCA1 mutation. Data related to age, marital status, consanguinity, menopause status, familial history, taken into consideration and (Table 1) derived from the same geographic location and are representative of South Indian population from Telangana. There was a significant difference in allele distribution between patients and control subjects (W v/s M: χ2 P<0.0001, OR 18.06, 95% CI 6.31-51.65).
| Variables | Controls/Patients | Odd’s ratio | 95% CI | p-value |
|---|---|---|---|---|
| Age | ||||
| ≤40 | 44/18 | 6.833 | 3.413-13.813 | 0.000** |
| >40 | 56/82 | |||
| Menopause status | ||||
| Pre | 74/29 | 6.968 | 3.582-13.660 | 0.000** |
| Post | 26/71 | |||
| Consanguinity | ||||
| Yes | 8/26 | 0.247 | 0.097-0.616 | 0.001* |
| No | 92/74 | |||
| Diet Intake | ||||
| Veg | 10/18 | 0.506 | 0.204-1.240 | 0.153 |
| Non-Veg | 90/82 | |||
| Marital status | ||||
| Married | 86/75 | 0.246 | 0.054-0.963 | 0.037* |
| Unmarried | 14/03 | |||
Table 1: Demographic details of ovarian cancer patients and control subjects.
The demographic features of ovarian cancer patients and controls subjects have been represented on various variables like Age, Menopause Status, Consanguinity, Diet Intake and Marital Status.
The age of incidence of ovarian cancer seems to be population specific. Our ethnic group includes 100 OC patients of which 18% (≤ 40 years of age) and 82% (>40 years of age). Patients and control subjects were derived from the same ethnic group. A significant association of ovarian cancer patients with age (p<0.000), menopausal status (p<0.000), consanguinity (0.043) and marital status (p=0.022). On the other hand, there was no significant association with diet intake. Histopathologically, staging plays a major role, the ovarian tumors falls under major categories (Scully, 1987; Serov, 1973); epithelial, germ cell and sex cord-stromal cell tumors. According to our study, Epithelial (85%); Germ cell (04%); Sex cord-stromal (03%) and Unknown/ unclassified (08%). When taking family history into consideration, the study reflected over 32% are of familial cases and 68% are sporadic cases.
Mutation frequency (185delag) based on family history
Figure 1 shows the mutation-detection rate was dependent on different Cancer Case History that shows: Breast & Ovarian Cancer 7/9 (77.7%); Only Ovarian Cancer 3/4 (75%); History of Other Cancer 10/19 (52.6%); Sporadic Cases 31/68 (45.50%).
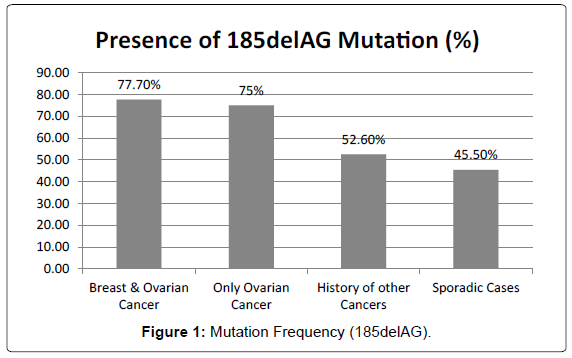
Figure 1: HPLC chromatogram of the nine reference compounds in 50% aqueous methanol, measured at 370nm. Retention times for rutin, sutherlandin A, sutherlandin B, kaempferol-3-O-rutinoside, sutherlandin C, sutherlandin D, quercitrin, quercetin and kaempferol were 11.9, 12.7, 13.8, 15.3, 16.2, 17.0, 18.0, 26.2 and 28.1 minutes, respectively.
Frequency of mutations in cases by age
Age has been considered as one of the potential factors for ovarian cancer as the risk increases with the advancement of age and the survival rate decreases accordingly. The average age at diagnosis of ovarian cancer was 52.5 years and the average age of menarche is 12.2 years, respectively. This graph is obtained in accordance with the age specific incidence of Ovarian cancer in south-Indian population. The age of the patients have been categorized into 4 groups ≤ 30 yrs (4); 31-40 yrs (14), 41-50 yrs (29) and ≥ 50 age group (53). However, the overall incidences in different groups were inconsistent and showed peak in ≥ 50 age group (Figure 2). Table 2 shows the distribution of 185delAG mutation of BRCA1 gene in control subjects and patients with ovarian cancer. WW 95%, WM 4% and MM 1% in controls and 52%, WM 36% and MM 12% in cases. An increased frequency of homozygotic mutant genotypes (MM) were found in patients compared to controls. There was a statistically significant difference in the distribution of allele frequencies in cases and controls (W v/s M: χ2 P<0.0001, OR 18.06, 95% CI 6.31-51.65).
| Genotype | Controls N=100% |
Patients N=100% |
Odds ratio | 95% CI | P value |
|---|---|---|---|---|---|
| WW | 95 (95) | 52 (52) | |||
| WM | 04 (4) | 36 (36) | 16.4 | 5.54-48.7 | <0.000** |
| MM | 01 (1) | 12 (12) | 21.9 | 2.77-173.3 | <0.0001** |
| Allelic Frequency | |||||
| W | 114 0.730 | 196 0.98 | |||
| M | 42 0.269 | 04 0.02 | 18.05 | 6.31-51.65 | <0.0001** |
Table 2: Distribution of 185delAG mutation and its allelic frequencies in patients and control subjects.
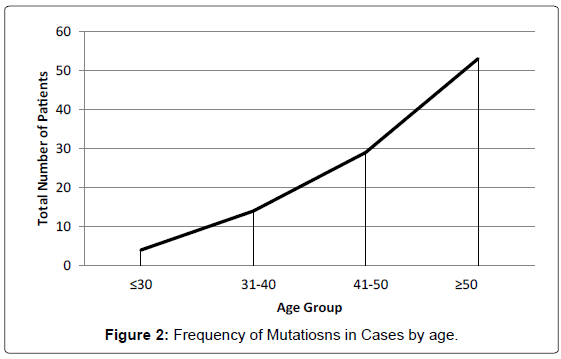
Figure 2: HPLC chromatogram of the nine reference compounds in 50% aqueous methanol, measured at 370nm. Retention times for rutin, sutherlandin A, sutherlandin B, kaempferol-3-O-rutinoside, sutherlandin C, sutherlandin D, quercitrin, quercetin and kaempferol were 11.9, 12.7, 13.8, 15.3, 16.2, 17.0, 18.0, 26.2 and 28.1 minutes, respectively.
In our present study, an increased BRCA1 185delAG is the founder mutation in many ethnic groups. This study supports the concept that the 185delAG of BRCA1 germ line mutation, referred to as ‘Ashkenazi mutation’, which is not restricted to a particular ethnic sub-group [14]. Ashkenazi and a considerable fraction of non-Ashkenazi 185delAG mutation carriers support the concept of a common ancient founder for this particular mutation in Jewish people of different ethnic origin [15]. The study conducted by Saxena et al. [16] on 204 families which included only 34 families had a positive family history [16]. One of the main features of familial breast/ovarian cancer is its early onset; therefore families with an early onset will be considered for BRCA1 and BRCA2 mutation study. But in India, to include such families in the screening program may not be reasonable because it has been reported in population based registries that the average age of breast cancer patients to be 50-53 which in case of American women is 61 years. This is an important fact because 90% of the breast cancers are of sporadic origin. Therefore, if early onset families are included in mutation screening studies, it may lead to compromised estimation of the mutation frequency. As per this study, the frequency of these two gene mutations in familial breast cancer cases was found to be 24.6% and ovarian contributed to 3.28% respectively. In different population it is 21% and 9% in Britain, 24% and 18% in France, 40% and 16% in Canada, and 39% and 25% in the USA, respectively, and in either genes 35% represented in the families of Sweden and Hungary [17].
This mutation occurs in an area of multiple adenosines residues which is prone to DNA slippage, thus indicating that this mutation has sustained the natural selective evolutionary pressure against it, with the finding of an apparent independent focus of its occurrence [18]. As the mutation 185delAG was predominantly detected among Ashkenazi Jews, it has been termed as the “Ashkenazi Mutation” because this group attained 1% carrier frequency within the population since origin of the ancestral mutation [19]. Among the breast/ovarian cancer patients, absence of 185delAG mutation in BRCA1 may be due to mutations in other regions like in non-coding and other coding regions of the gene and in other genes like BRCA2, PTEN, p53 [20-22]. 185delAG mutation is one of the most common mutations, it is located at the 5’ end of the gene and predicted to cause truncation at the beginning of the zinc-binding region of the RING of the putative polypeptide. It was proposed that mutations within the BRCA1 RING domain predispose to cancer by inactivating BRCA1 ubiquitin protein ligase activity [23].
In our present study, an increased frequency of homozygotic mutant genotype (MM) was found and a statistical significant association was noticed in the distribution of 185delAG in patients compared to control subjects. Further studies are required based on mutational analysis for identification of related mutations and polymorphisms. The biological effects of the protein related to polymorphisms can be understood which will help in predicting the etiology of ovarian cancer in different geographical regions. Proper counselling of patients and presymptomatic mutation carriers will help them make better decisions about medical and surgical preventive options.
From this study, we found that the prevalence of 185delAG of BRCA1 gene have shown some similarities and difference when compared with other populations. This study also emphasizes the importance of demographic details which play major role in mutation screening. Patients who are at a high risk of early-onset disease, with appropriate awareness i.e. genetic counselling, counselling should include a discussion of the basic principles of hereditary cancer susceptibility as well as an evaluation of the woman’s own risk of cancer, and how testing would add to the characterization of those risks, and how medical management would be affected by a positive and a negative test result so that patients and carriers would be in safe zone.
The authors are thankful to Mr. P. Madhava Prasad and all the clinical staff of Yashoda Hospitals, Secunderabad.