Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Review Article - (2015) Volume 3, Issue 5
The development of venous thromboembolism is one of the major causes of morbidity and mortality in patients with cancer. The standard treatment of deep venous thrombosis or pulmonary embolism occurring in patients with active malignancy remains the use of low molecular weight heparins. However, in clinical practice, practitioners are frequently asked about the efficacy and safety of various new oral anticoagulants in cancer patients. In the United States, there are currently 4 different novel oral anticoagulants commercially available with the indication of the treatment of acute venous thromboembolism. These include dabigatran (Pradaxa), rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa). Use of these new medications is appealing due to the ease of administration, avoidance of injections, ability to use in patients with decreased renal or liver function, and consistent efficacy without fooddrug interactions. Currently, the only available data for the use of these new oral anticoagulants in cancer patients is from subgroup analysis of larger studies with no statistical significance. However, this preliminary data is encouraging that the novel oral anticoagulants may be effective and safe for primary and secondary prevention of venous thromboembolism in cancer patients. Further clinical trials are greatly needed for the head-tohead comparison of these novel oral anticoagulants versus low molecular weight heparins. Although the routine use of novel oral anticoagulants for the prevention or treatment of venous thromboembolism in cancer patients cannot be recommended at this time, we strongly support the development of Phase III trials assessing their efficacy and safety in patients with active malignancies compared to the current standard of care treatment with low molecular weight heparin.
Keywords: Anticoagulant; Cancer; Malignancy; Venous thromboembolism
ASCO: American Society of Clinical Oncology; DVT: Deep Venous Thrombosis; ESMO: European Society for Medical Oncology; FDA: Food and Drug Administration; LMWH: Low Molecular Weight Heparin; NCCN: National Comprehensive Cancer Network; NOAC: Novel Oral Anticoagulants; PE: Pulmonary Embolism; RCT: Randomized Controlled Trial; VKA: Vitamin K Antagonists; VTE: Venous Thromboembolism
Active malignancy is a significant risk factor for the development of venous thromboembolism (VTE). Of note, the association between cancer and VTE was first reported in 1823 by Jean-Baptiste Bouillaud [1] followed by Armand Trousseau in 1865 [2]. VTE is one of the major causes of death in patients with cancer and the increased risk of VTE in cancer patients undergoing cytotoxic chemotherapy is estimated to be six fold higher when compared to the general population [3,4]. To this end, extensive research has been performed to examine the methods to decrease the incidence of VTE in cancer patients as well as the morbidity/mortality associated with VTE once it occurs. The American Society of Clinical Oncology (ASCO) 2014 clinical practice guidelines on VTE prophylaxis and treatment in patients with cancer recommends against the routine use of thromboprophylaxis for ambulatory patients with cancer, but allows consideration of prophylaxis for high-risk patients. Currently, low molecular weight heparin (LMWH) remains the agent of choice for the initial 5 to 10 days of treatment for newly diagnosed VTE as well as for the long-term secondary prophylaxis for at least 6 months in patients with cancer. The use of the novel oral anticoagulants (NOACs) is not recommended for patients with active cancer because of limited data comparing NOACs to standard treatment with LMWH [5]. However, the use of NOACs in cancer patients receiving active treatment for their malignancy is appealing due to the ease of administration, avoidance of injections, ability to use in patients with decreased renal or liver function, and consistent efficacy without food-drug interactions. Here we perform a review of the literature to examine the evidence supporting primary and secondary prevention of VTE in patients with active malignancy, with a specific focus on the clinical trial evidence for the use of NOACs in this setting.
The average annual incidence of VTE is more than 1 in 1000 [6]. The most common causes of VTE in order of rate of occurrence are institutionalization (current/recent hospitalization or nursing home), idiopathic, malignancy, trauma, congestive heart failure, central venous catheter or pacemaker placement, neurological disease with extremity paresis, and superficial vein thrombosis. Patients with VTE attributable to malignancy represent approximately 20% of all VTE cases and 25% of cases are idiopathic. Importantly, as high as 25% of all cases of pulmonary embolism can present as sudden death with a poor 1-week survival rate of 71% [7]. A recent study published in March 2015 by Petterson et al., examined the risk of VTE based on the specific site of cancer and revealed that cancer of the pancreas, brain, gastrointestinal (esophagus, small intestine, gallbladder, other biliary), liver, and lymphoma have the highest risk of VTE. Patients with leukemia, liver cancer and stomach cancer were noted to be at intermediate risk [8]. It is also known that specific cancer treatment regimens can influence the propensities of VTE in patients. As such, cancer patients receiving cisplatin-containing regimens have 18% incidence of VTE compared with 34% in patients receiving a combination of lenalidomide and high dose corticosteroids for multiple myeloma [3]. Other cancer treatments such as hormonal therapy, angiogenesis inhibitors, or some kinase inhibitors are also known to increase the risk of thrombosis. However, in everyday clinical practice, it can be difficult to determine the individualized risk of VTE for a patient. In this context, the 2013 ASCO clinical practice guidelines recommended calculation of the Khorana score to estimate the risk of thrombosis for patients with cancer in the outpatient setting [9]. To determine the risk, this scoring system assimilates the following patient characteristics: site of cancer, pre-chemotherapy platelet count, pre-chemotherapy hemoglobin levels or use of red blood cell growth factors, pre-chemotherapy leukocyte count, and body mass index. Each patient characteristic is assigned a score and the possible outcomes are as follows: a) high risk score >3; b) intermediate risk score 1-2; c) low risk score 0 (Table 1).
| Patient Characteristics | Risk Score |
| Site of Cancer: | |
| Very high risk site (stomach and pancreas) | 2 |
| High risk site (lung, lymphoma, gynecologic, bladder, testicular) | 1 |
| Standard risk site (any other site) | 0 |
| Platelet count >350,000/mm3 | 1 |
| Hemoglobin level <10g/dl or use of red cell growth factors | 1 |
| Leukocyte count >11,000/mm3 | 1 |
| Body mass index >35 kg/m2 | 1 |
Table 1: Khorana risk score – predictive model for VTE in ambulatory cancer patients.
The Khorana score has been validated prospectively and will estimate a patient’s 6 month probability of developing VTE. In one large cohort study, the 6 month probability of developing a VTE was 1.5% with score 0, 3.8% with score 1, 9.4% with score 2, and 17.7% with score 3 [10]. Currently, additional ongoing randomized trials are evaluating whether primary VTE prophylaxis in patients with high Khorana scores translates into decreased incidence of VTE. Notably, all three guideline panels from American Society of Clinical Oncology (ASCO), National Comprehensive Cancer Network (NCCN), and European Society for Medical Oncology (ESMO) have uniformly recommended that venous thromboembolism prophylaxis should be considered for patients with a high risk Khorana score [9,11,12]. The subsequent pivotal step following the assessment of a patient determined to be high risk for VTE is the selection of the appropriate anticoagulation agent used for chemoprophylaxis. Current outpatient options include low molecular weight heparin products (LMWH), vitamin K antagonists (VKA), and the new oral anticoagulants (NOACs). The following section will comprise of the clinical trial data for the primary and secondary prevention of VTE in cancer patients for each of these agents.
Low molecular weight heparin
The current standard of care for both primary and secondary VTE prophylaxis in patients with active malignancy is the use of LMWH. The Cochrane Collaboration published a comprehensive review of 21 randomized controlled trials (RCTs) with a total of 9861 patients, all evaluating pharmacological interventions to prevent VTE in patients with cancer [13]. A subset of this analysis included 13 studies that compared LMWH (Dalteparin, Enoxaparin, Certoparin, or Nadroparin) with placebo. The use of LMWH decreased the risk of VTE by 36% (RR 0.64, 95% CI 0.45-0.91) without statistically significant increased incidence of major bleeding [13]. In 2014, an additional Cochrane Collaboration review was published that included 15 RCTs with a total of 7622 patients comparing anticoagulation with heparin or LWMH vs. no anticoagulation in ambulatory patients with active malignancy. The results were similar to the first, with prophylactic use of LMWH decreasing the risk of developing VTE by 46% (RR 0.56; 95% CI 0.42-0.74) compared with no anticoagulation. However, there was an increased risk of minor bleeding with anticoagulation; but no increased risk of major bleeding events. They found a 3% decrease in mortality at 12 months and 5% decrease in mortality at 24 months for patients treated with LMWH, but this was not statistically significant [14]. In 2003, the CLOT Trial established LMWH as the standard of care over VKA as secondary prophylaxis of acute VTE in patients with cancer. This trial compared dalteparin for 5 to 7 days followed by 6 months of treatment with a VKA to 6 months of treatment with dalteparin. The results of the CLOT trial reported a statistically significant decrease in recurrent VTE with use of dalteparin compared to VKA in patients with cancer. During the 6 month follow-up period, 27 of 336 patients (9%) in the dalteparin group had recurrent VTE compared with 53 of 336 patients (17%) in the VKA group (HR 0.48, 95% CI 0.3-0.77, P=0.002). There were no statistically significant differences in rates of bleeding events between the 2 groups. The 6 month mortality rate was higher in the VKA group at 41% compared with 39% in the dalteparin group, P=0.53 [15].
Vitamin K antagonists
In clinical practice, limitations prevail in the use of vitamin K antagonists for chemoprophylaxis to prevent VTE in patients with active malignancy and these are considered less suitable for long-term management and secondary prevention once VTE has occurred [15,16]. The Cochrane Collaboration has looked at the effect of prophylactic oral anticoagulation on overall survival (OS), comparing warfarin vs. placebo/no treatment in patients with active malignancy and no other indication for anticoagulation. Data from 5 pooled RCTs showed no benefit in OS at 6 months, 1 year, 2 years, and 5 years. Warfarin increased the incidence of both major bleeding and minor bleeding [16]. All major consensus guidelines recommend a LMWH for initial and long-term treatment of cancer associated thrombosis; however the ASCO 2013 VTE Prevention and Treatment Guidelines recommends a VKA with INR of 2-3 if LMWH is unavailable or contraindicated [9].
In the United States, there are currently 4 different novel oral anticoagulants commercially available with the Food and Drug Administration (FDA) indication of the treatment of acute deep venous thrombosis (DVT) or pulmonary embolism (PE). These include dabigatran (Pradaxa), rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa) (Figure 1).
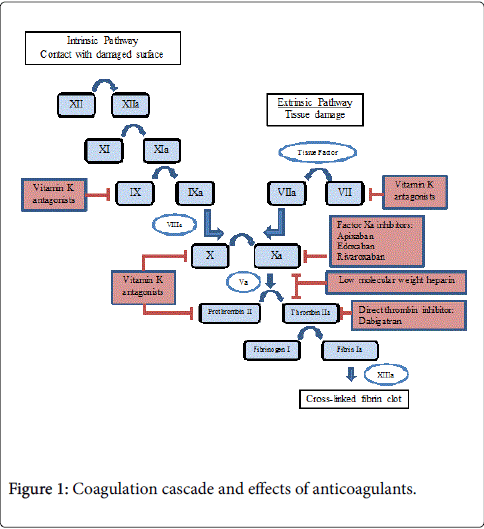
Figure 1: Coagulation cascade and effects of anticoagulants.
However, the only available data for the use of these NOACs in cancer patients is from subgroup analysis of larger studies. To date, there has only been one published prospective randomized controlled trial examining the efficacy and safety of NOACs specifically in patients with cancer [17]. The following is a summary of the currently available data using NOACs in patients with active malignancy, extracted from subset analysis of larger studies.
Oral thrombin inhibitors
Dabigatran: Dabigatran etexilate (pro-drug of dabigatran) is a reversible, competitive and direct thrombin inhibitor (Pradaxa, Boehringer Ingelheim Pharmaceuticals) which acts by inhibiting the serine protease thrombin and prevents the conversion of fibrinogen into fibrin, thus preventing thrombus formation. The anticoagulant properties of dabigatran have been published in 5 clinical trials: RE-LY, RE-COVER, RE-COVER II, RE-MEDY, and RE-SONATE. The RE-LY trial showed the superiority of dabigatran over warfarin for the prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation [18]. The RE-COVER and RE-COVER II trials are randomized trials examining the secondary prevention and safety of dabigatran vs. warfarin in patients with DVT or PE. Both trials showed that dabigatran had similar efficacy as warfarin for the prevention of recurrent VTE (2.4% vs. 2.2% respectively) as well as similar safety profile [19,20]. The RE-COVER trial included 5% of patients in the dabigatran group with active cancer compared with 4.5% of patients in the warfarin group. A subgroup analysis of 121 patients with active cancer showed a recurrence of VTE in 5.3% of cancer patients treated with dabigatran vs. 3.1% of patients treated with warfarin (p=0.49). However, this was not a pre-planned analysis and patients with a life-expectancy of less than 6 months were excluded [19]. After completion of at least 6 months of treatment on the RE-COVER study, patients were eligible for enrollment into the RE-MEDY or RE-SONATE studies. The RE-MEDY study examined the incidence of recurrent VTE in patients treated with a prolonged course of anticoagulation with either dabigatran vs. warfarin for 6 to 36 months and found similar rates of recurrent VTE (1.8% with dabigatran and 1.3% with warfarin). The dabigatran group had a significantly decreased incidence of bleeding compared to warfarin (0.9% vs. 1.8%, HR 0.54; 95% CI 0.41-0.71) but had an increased incidence of acute coronary syndrome (0.9% vs. 0.2%, p=0.02). Subset analysis of the RE-MEDY trial found that 119 patients had active cancer during study and 2 patients treated with dabigatran had recurrent VTE compared to 1 patient treated with warfarin. The RESONATE study examined the incidence of recurrent VTE in patients who had received 3 months of anticoagulation with dabigatran and compared continued treatment with dabigatran to placebo. Recurrent VTE occurred in 3 of 681 (0.4%) patients receiving prolonged anticoagulation with dabigatran compared with 37 of 662 (5.6%) patients treated with placebo. There was no subset analysis performed for patients with active cancer [21].
Oral factor Xa inhibitors
Rivaroxaban: Rivaroxaban (Xarelto, Janssen Pharmaceuticals) is a selective inhibitor of factor Xa and does not require a cofactor for activity. Rivaroxaban inhibits free factor Xa and prothrombinase activity. It does not have a direct effect on platelet aggregation, but indirectly inhibits platelet aggregation induced by thrombin. By inhibiting factor Xa, rivaroxaban decreases thrombin generation. The MAGELLAN study was performed in hospitalized patients >40 years of age with acute medical illnesses with decreased level of mobility and compared rivaroxaban for 35 days to enoxaparin for 10 days as thromboprophylaxis to prevent VTE. Rivaroxaban for 35 days was superior to enoxaparin for 10 days in preventing VTE. VTE occurred in 4.4% of patients receiving rivaroxaban and 5.7% receiving enoxaparin (RR 0.77; 95% CI 0.62-0.96)l P= 0.0211). However, both minor and major bleeding rates were higher in the rivaroxaban group. Patients with active cancer were included in this trial with subgroup analysis showing 7% of patients in both treatment arms had cancer. In the subset of patients with cancer, thromboprophylaxis with rivaroxaban for 35 days showed a non-significant trends towards inferiority compared with treatment with enoxaparin for 10 days (9.9% vs. 7.4%l RR 1.34; 95% CI 0.71-2.54) [22]. Rivaroxaban was evaluated for prevention of symptomatic recurrent VTE in patients with acute VTE in the EINSTEIN-DVT and EINSTEIN-PE studies and each study included a subset of patients with active cancer. The EINSTEINDVT study enrolled 3449 patients and compared rivaroxaban vs. enoxaparin/followed by VKA for 3, 6,or 12 months in patients with acute DVT [23]. The EINSTEIN-PE study enrolled 4832 patients who had acute symptomatic pulmonary embolism and compared rivaroxaban to enoxaparin followed by VKA for 3, 6 or 12 months [24]. Both studies concluded that rivaroxaban had non-inferior efficacy in preventing recurrent VTE and PE compared to standard therapy of enoxaparin bridge followed by warfarin. The EINSTEIN-DVT study included 207 (6%) patients with active cancer and the EINSTEIN-PE study included 223 (4.6%) patients with active cancer [23,24]. Pooled analysis of these studies showed that treatment with Rivaroxaban or LMWH followed by VKA had similar rates of recurrent VTE in patients with active cancer [25].
Apixaban: Apixaban (Eliquis, Bristol-Myers Squibb) is an oral, direct, and highly selective factor Xa inhibitor with high oral bioavailability. The AMPLIFY study showed non-inferiority of apixaban compared with traditional therapy of LMWH followed by VKA for 6 months as secondary prevention after VTE. Recurrent symptomatic VTE or VTE-related death occurred in 59 of 2609 patients (2.3%) treated with apixaban compared with 71 of 2635 (2.7%) of patients treated with LMWH/VKA (RR 0.84, 95% CI 0.60-1.18). Apixaban had lower bleeding rates compared to LMWH/VKA. There were 42 patients (1.7%) with active cancer enrolled in this study, but results of subgroup analysis has not been reported and the authors have concluded that additional information is needed to assess the safety and efficacy of apixaban for cancer associated VTE [26]. In the ADOPT study, apixaban was also studied as an agent for VTE prophylaxis in medically ill hospitalized patients and patients were randomized to receive either apixaban 2.5 mg po BID for 30 days or enoxaparin 40 mg subcutaneously daily for 7-14 days. The primary endpoint of major VTE or death by day 30 was similar in both treatment groups but with higher rates of bleeding in the apixaban group. The authors concluded that an extended course of anticoagulation with apixaban was not superior to shorter course of LMWH in prevention of VTE in hospitalized medically ill patients. 9.7% of patients enrolled in the ADOPT study had a history of cancer, but no subgroup analysis was performed [27]. In the phase II pilot study ADVOCATE, the efficacy of apixaban for primary VTE prevention in patients receiving chemotherapy was examined. This study enrolled patient with active malignancy and receiving first or second line chemotherapy for myeloma, lymphoma, advanced breast, pancreatic, gastrointestinal, lung, ovarian, or prostate cancer. Patients determined to have a high risk of bleeding were excluded. 125 patients were enrolled and randomized to receive apixaban or placebo for a total of 12 weeks. No patients in the apixaban group developed symptomatic VTE compared to 3 patients in the placebo group [17]. Interpretation of these results is difficult due to small sample size and no recommendations were made to routinely use apixaban as VTE primary prophylaxis in patients receiving chemotherapy, but further Phase III confirmatory studies could be performed in the future.
Edoxaban: Edoxaban (Lixiana, Daiichi-Sankyo) is a novel oral direct factor Xa inhibitor. Edoxaban has been available in Japan since 2011 for the prevention of VTE in patients undergoing orthopedic surgery. In 2014, results of the HOKUSAI-VTE study were published comparing edoxaban to VKA in the secondary prevention of patients with acute VTE. 8240 patients were enrolled with 4118 patients randomized to receive edoxaban 60 mg po daily and 4122 patients received LMWH followed by VKA (INR 2.0-3.0 for 3-12 months). The primary endpoint of recurrent VTE occurred in 130 patients (3.2%) receiving edoxaban and 146 (3.5%) of patients receiving LMWH/VKA (HR 0.89, 95% CI 0.70-1.13). Edoxaban had less major and minor bleeding compared with VKA. A subset analysis of 208 (3.5%) patients with active cancer was performed with 3.7% of patients in the edoxaban group experiencing recurrent VTE compared to 7.1% of patients in the VKA group. It was concluded that edoxaban was noninferior to VKA in secondary prevention of VTE [28]. Based on these results, in January 2015, the FDA approved edoxaban in the US for prevention of stroke in non-valvular atrial fibrillation and for the treatment of acute VTE (Table 2).
| Generic Name | Dabigatran | Rivaroxaban | Apixaban | Edoxaban | Warfarin |
| Trade Name | Pradaxa | Xarelto | Eliquis | Savaysa | Coumadin |
| MOA | Direct thrombin inhibitor | Factor Xa inhibitor | Factor Xa inhibitor | Factor Xa inhibitor | Inhibits synthesis of vitamin K dependent clotting factors |
| FDA Indications | 1.Stroke prevention in non-valvularafib 2. Treatment of acute DVT/PE 3.Secondary prophylaxis |
1.Stroke prevention in non-valvularafib 2. Treatment of acute DVT/PE 3.Secondary prophylaxis 4.DVT prophylaxis after hip/knee replacement |
1.Stroke prevention in non-valvularafib 2. Treatment of acute DVT/PE 3.Secondary prophylaxis 4.DVT prophylaxis after hip/knee replacement |
1.Stroke prevention in non-valvularafib 2. Treatment of acute DVT/PE |
1.Stroke prevention in non-valvularor valvularafib 2. Treatment of acute DVT/PE 3.Primary or secondary VTE prophylaxis |
| Dosing | CrCl>30 – 150 mg po BID CrCl 15-30 –75 mg po BID HD – Not defined |
Afib: CrCl>50 – 20 mg poqd CrCl 15-50 –15 mg poqd VTE: 15 mg po BID x 21 days, then 20 mg qd DVT prophylaxis: 10 mg poqd *Take with food |
Afib: 5 mg po BID VTE: 10 mg po BID x 7 days, then 5 mg po BID Hip: 2.5 mg po BID x 35 days Knee: 2.5 mg po BID x 12 days *Dose reduce if Age >80 Weight <60kg creatinine>1.5 |
CrCl 50-95 – 60 mg poqd CrCl 15-50 – 30 mg poqd *Dose reduce if weight <60 kg |
Individualized dosing titrated to achieve desired INR goal |
| Contraindications | -Pregnancy C -mechanical heart valves -spinal anesthesia |
-Pregnancy C -mechanical heart valves -Child Pugh B/C -spinal anesthesia |
-Pregnancy C -mechanical heart valves -Child Pugh B/C -spinal anesthesia |
-Pregnancy C -mechanical heart valves -CrCl>95 -CrCl<15 -Child Pugh B/C -spinal anesthesia |
-Pregnancy X -Prior warfarin tissue necrosis |
| Reversal | Hemodialysis – 49% cleared from plasma in 4 hours | -Not dialyzable -PCC -aPCC (off label) -Activated FVII -Activated charcoal |
-Not dialyzable -PCC -aPCC (off label) -Activated FVII -Activated charcoal |
-Not dialyzable -PCC -aPCC (off label) -Activated FVII -Activated charcoal |
-Vitamin K -PCC -aPCC (off label) -Activated FVII -Activated charcoal |
| Trials | RE-LY RE-COVER RE-COVER II RE-MEDY RE-SONATE |
MAGELLAN EINSTEIN-DVT EINSTEIN-PE |
AMPLIFY ADOPT ADVOCATE |
HOKUSAI-VTE | Numerous trials |
Table 2: Characteristics of oral anticoagulants.
The results of three recent systematic reviews and meta-analyses of pooled Phase III trial data provides some evidence for the seemingly similar efficacy and safety between the four available novel oral anticoagulants and conventional treatment for secondary prevention of VTE in patients with cancer [29-31]. Each of these three meta-analyses performed subgroup analysis of phase III trials investigating NOACs for the treatment of VTE in cancer patients with the endpoints of efficacy outcome of recurrent VTE and the safety outcome of bleeding rates. Van der Hulle et al. 2014 analyzed five studies (RE-COVER I, RE-COVER II, EINSTEIN-DVT, EINSTEIN-PE, HOKUSAI-VTE) including 973 patients with active cancer. The pooled incidence rate of recurrent VTE was 4.1% in patients treated with NOACs and 6.1% in patients treated with VKAs (RR 0.66, 95% CI 0.38-1.2). The pooled incidence rate of major or clinically relevant bleeding was 15% in cancer patients treated with NOACs and 16% in patients treated with VKAs (RR 0.94, 95% CI 0.70-1.3) [29]. Sadar et al. 2014 analyzed six studies (RE-COVER I, RE-MEDY, EINSTEIN-DVT, EINSTEIN-PE, MAGELLAN, ADVOCATE) including 1,197 patients with active cancer. The pooled incidence rate of recurrent VTE/VTE-related death was 4.6% in patients treated with NOACs and 5.5% in patients treated with LMWH/VKA/placebo (OR 0.80, 95% CI 0.39-1.65). The pooled incidence rate of major or clinically relevant bleeding was 8.6% in cancer patients treated with NOACs and 5.8% in patients treated with LMWH/VKA/placebo (OR 1.49, 95% CI 0.82-2.71) [30]. Lastly, Vedovati et al. 2015 analyzed six studies (RE-COVER I, RE-COVER II, EINSTEIN-DVT, EINSTEIN-PE, HOKUSAI-VTE, AMPLIFY) including 1,132 patients with active cancer. VTE recurrence occurred in 3.9% of patients treated with NOACs and in 6.0% treated with VKAs (OR 0.63, 95% CI 0.37-1.10). Clinically relevant bleeding occurred in 14.5% of patients treated with NOACs and in 16.5% of patients treated with VKA (OR 0.85, 95% CI 0.62-1.18) [31]. Each of these three meta-analyses of phase III trial data had similar results showing that the use of NOACs in patients with active cancer was associated with a non-statistically significant reduction in VTE recurrence compared to comparator arms with similar rates of clinically relevant bleeding. However, it is important to note that in these studies the vast majority of patients with active cancer treated with NOACs were compared to patients treated with heparin followed by VKA and not the current standard of care with LMWH.
The prevention and treatment of venous thromboembolism in patients with active malignancy can be challenging and in clinical practice oncologists are frequently asked about the role of the novel oral anticoagulant agents for the prevention or treatment of VTE in this population. The only available data for the use of NOACs in cancer patients is from subgroup analysis of larger studies with no statistical significance. However, this preliminary data is encouraging that NOACs may be effective and safe for primary and secondary prevention of VTE in cancer patients. Further clinical trials are greatly needed for the head-to-head comparison of NOACs versus LMWHs. Although the routine use of NOACs for the prevention or treatment of VTE in cancer patients cannot be recommended at this time, we strongly support the development of Phase III trials assessing their efficacy and safety in patients with active malignancies compared to the current standard of care treatment with LMWHs.