Orthopedic & Muscular System: Current Research
Open Access
ISSN: 2161-0533
ISSN: 2161-0533
Research Article - (2014) Volume 0, Issue 0
Objective: To provide descriptive information on the risk of osteonecrosis (ON) in persons with osteoarthritis (OA) of the knee by age and gender.
Methods: The General Practice Research Database was used to construct a retrospective cohort of persons aged 18 to 89 years with OA of the knee between 1/1/2007 and 12/31/2009. Eligibility criteria included six months of medical history prior to the index date of knee OA and at least one activity record afterwards. Persons with a bilateral knee replacement prior to or on the index date were excluded. From this study sample we identified all firsttime diagnosed cases of ON in the study period and estimated rates.
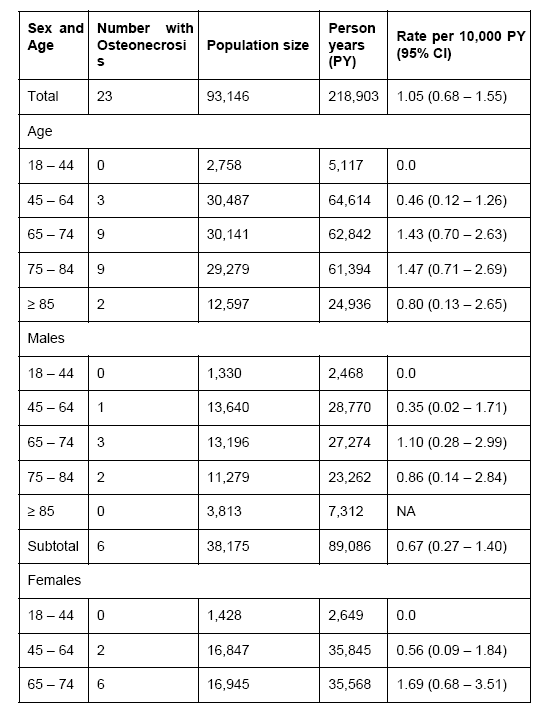
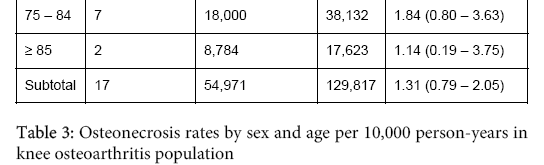
Results: We identified 93,146 individuals representing 218,903 person-years (PY) who had a diagnosis of knee OA and who met all study criteria. The median time to onset of ON from the index diagnosis of knee OA was 17.4 months. The three-year cumulative incidence rate of ON in this knee OA population was 1.05 (95% CI: 0.68-1.55) per 10,000 PY. The risk of ON increased until age 85 years. The risk of ON was higher among females than males (females=1.31, 95% CI: 0.79-2.05 per 10,000 PY; males=0.67, 95% CI: 0.27-1.40 per 10,000 PY).
Conclusion: Rates of ON are higher in women and older people in the knee OA population which is predominantly elderly and female. With the growing population of elderly, especially females, the number of cases of ON is likely to increase among individuals with knee OA over time.
Keywords: Osteonecrosis; Osteoarthritis; Knee osteoarthritis; Epidemiology; Cohort; Incidence rate; General Practice Research Database
Little is known about the epidemiology of osteonecrosis (ON) because of its rarity in the general population. ON is associated with traumatic (e.g., vascular trauma, dislocations, etc.), non-traumatic (e.g., infections, systemic lupus erythematosus, etc.) and iatrogenic conditions (e.g., corticosteroids, radiation exposure, etc.) [1,2]. Most of the literature examining the risk of ON focuses on either the hip in adults, the jaw in association with bisphosphonates, ON related to childhood onset conditions such as sickle cell anemia, or ON related to corticosteroid use for the treatment of conditions such as acute lymphoblastic leukemia [2-7]. In general, these studies are based on data from specialty centers treating these conditions and true measures of risk of ON for persons with knee osteoarthritis (OA) cannot be calculated from them.
Persons with knee OA are potentially at high risk for ON because of the underlying disease pathology and/or the widespread use of corticosteroids to manage pain and physical disability. It is estimated that around 37% of adults aged 60+ years have radiographic knee OA and the estimated lifetime risk of symptomatic OA in at least one knee is around 45%, with the risk further increasing among those with a history of knee injury or high body mass index (BMI) [8,9]. Given the high prevalence of knee OA, it is important to examine the risk of ON in this population. Thus, we conducted a retrospective cohort study to characterize the risk of ON among individuals with knee OA.
Data for this study were derived from the U.K. General Practice Research Database (GPRD). The database is housed and organized for research purposes at the Boston Collaborative Drug Surveillance Program. The data resource has been previously described in detail and validation of its data elements is on-going [10-13]. The GPRD is a longitudinal database that continuously collects data from over 500 general practices in the UK. It is a unique computerized, medical data resource for epidemiological research for two main reasons: a) the primary health care system comprehensively covers the UK population and b) the information on all relevant medical care is located in the offices of the general practitioners, who function as “gatekeepers” for hospital and specialist referrals in the UK health system. The GPRD contains information on more than 5 million patients, of which over 3.5 million are currently active (approximately 5% of the UK population), with a cumulative follow-up time of more than 35 million person years. It has a representative age/sex distribution of the entire UK population. The information recorded includes patient demographics and characteristics (e.g. height, weight, smoking status), symptoms, clinical diagnoses, consultant referrals, hospitalizations, lab test results, and drug prescriptions.
Study sample
The sample comprised all people in the GPRD who had a qualifying Read code for knee OA (Table 1) at any time before January 1, 2010 and who were present in the database during the study period, January 1, 2007 to December 31, 2009, and who were aged 18 to 89 years at first diagnosis of knee OA. We also included people with a diagnosis of non-specific arthritis of the knee (“N06z611 – knee arthritis NOS”), in the absence of a history of rheumatoid arthritis, gout, pseudogout, systemic lupus erythematosus, or psoriatic arthritis any time before or within one year after the first knee arthritis diagnosis unless they had a diagnosis of OA any time in their medical history. The date of the first diagnosis of the knee OA in the study period was designated as the “index date”, unless the first knee OA was diagnosed prior to the study period (i.e. a prevalent case), in which case index date was January 1, 2007. If a patient had a knee replacement code recorded before the date of the index diagnosis, we considered the date of the first knee replacement as the first date of knee OA diagnosis. Additional eligibility criteria were: at least 6 months of recorded data in the database prior to the index diagnosis interval and at least one recorded entry after the index diagnosis. Each eligible subject was followed until they developed ON, transferred out of the general practice, died, or reached the end date of the study (December 31, 2009), whichever came first. If a patient had a history of bilateral knee replacement before or at the index date, or if a patient had a first knee OA diagnosis on December 31, 2009, he/she was excluded from this study. A total of 93,146 patients met the inclusion/exclusion criteria.
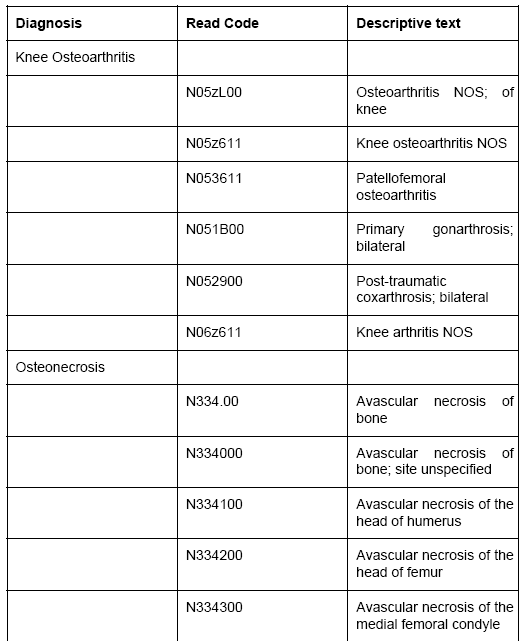
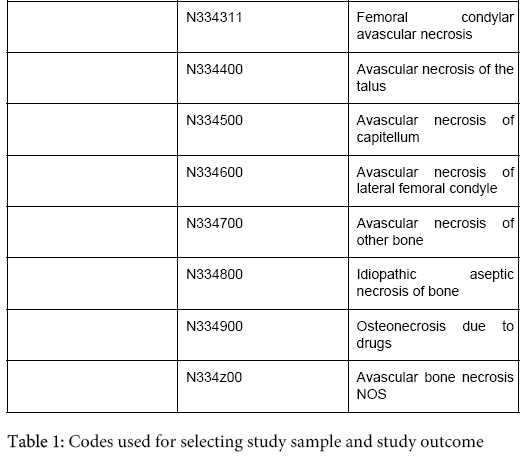
The Read codes used to identify cases of ON were selected in cooperation with both experienced physicians and epidemiologists to ensure that they accurately represented the diagnoses of interest. Codes are listed in Table 1.
Analysis
Incidence rates and 95% confidence intervals (CIs) were calculated and reported as the number of events per 10,000 person-years (PY) at risk. Incidence rates were calculated for the entire study period (cumulative risk). Incidence rates were also calculated, stratified by gender and age group (18-34, 35-44, 45-54, 55-64, 65-79, and 80+) and age/gender group. All analyses were conducted using SAS version 9.2 (SAS Institute, Cary, NC).
The median time from the index diagnosis to the first ON diagnosis in the observation period was 17.4 months (interquartile range: 5.2-21.9). The three-year cumulative incidence rate of ON in this knee OA population was 1.05 (95% CI: 0.68-1.55) per 10,000 PY. The incidence rate of ON increased until aged 85+ years after which it declined. Osteonecrosis was not observed among those less than age 45. There were marked differences in the incidence rates between the genders, with the rate of ON being nearly double among females relative to males. For each age group, females had a higher incidence of ON than males (Table 3).
To the authors’ knowledge, this is the first report to characterize the risk of ON specifically in persons with knee OA in a European population. Because of the infrequent occurrence of ON, a large sample such as this one was required to provide meaningful risk estimates for the full study sample as well as for study subgroups. Our results, which showed higher risks of ON in women and with increasing age up to age 85, are at variance with those of Cooper, et al. where the risk of ON was higher among men (study period 1999 through 2003) [14]. One explanation for the differences is that Cooper et al. utilized the general population from which to base their rates while the computation of risk of ON in our study was determined from a population of those with knee OA. A review of the literature reported that ON occurs predominantly in males [1], however there is more knee OA in females, thus the population of this study contained a larger proportion of females than the Cooper study. The data reported herein show that the highest rates of ON were between ages 65 and 84 which is also at variance with the dated literature, which suggests peak rates occur between 30 and 60 years of age [1]. Again, the reported results are based on a different population than these results.
The natural history of ON is not well understood, in part owing to its uncommon occurrence. Our study provides some insight into the natural history of ON in the knee OA population by describing the risk of its occurrence among age and sex groups. Despite this, there are several limitations of this study. One is that we cannot characterize the risk of ON by the severity of knee OA due to lack of radiographic features of the knee at index diagnosis. Another limitation is that we may have missed some ON cases. However, given the serious nature of ON, it is expected that the vast majority of these events would be captured in the GPRD. Finally, selection bias may have occurred due to our sample inclusion criteria.
Rates of ON are higher in women and older people in the knee OA population which is predominantly elderly and female. With the introduction of new treatments for knee OA, data such as these provide important information on the risk of ON among persons with knee OA and give us context in which to interpret certain safety concerns.
Abbott Laboratories provided funding to the Drug Research Group, Inc. d.b.a. Boston Collaborative Drug Surveillance Program for conducting the study. The authors declare that they have no conflict of interest.
The authors thank Denise Oleske, Steve Niemcryk, Ming Ji and Jerry Hall of Abbott Laboratories for their valuable input into the study design and Nataliya Kuptsova-Clarkson of Abbott Laboratories M.D., Ph.D., for assistance in reviewing the diagnoses codes used in this report.
This study was funded by Abbott Laboratories.
Drs. Jick and Li received funding from Abbott Laboratories for the conduct of this project.
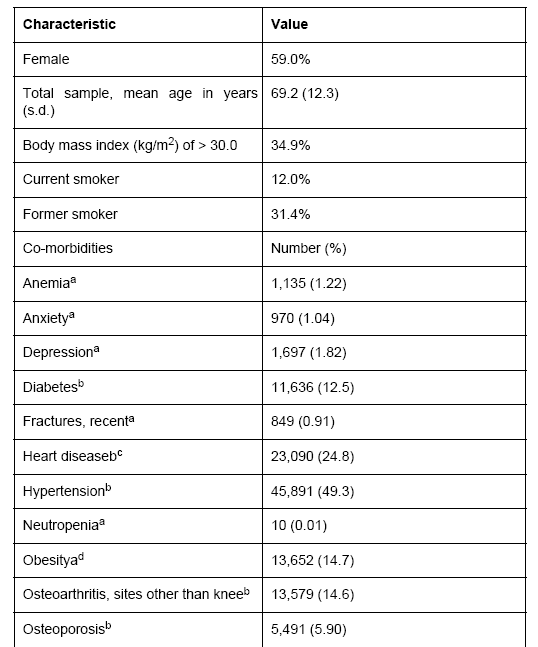
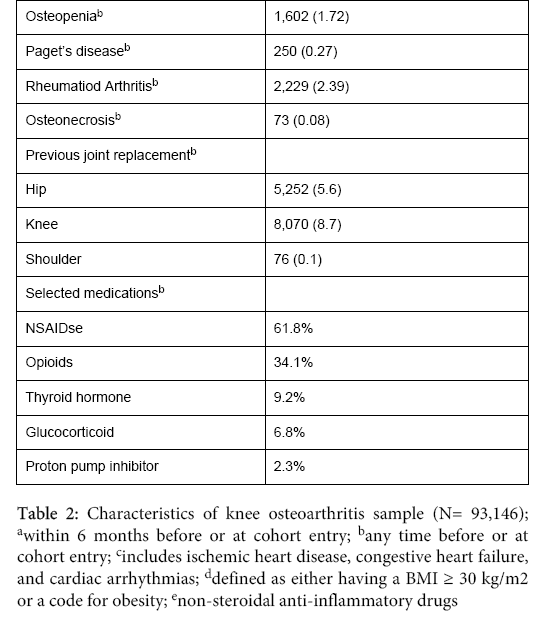
Table 2 Characteristics of knee osteoarthritis sample (N= 93,146) Table 3 Osteonecrosis rates by sex and age per 10,000 person-years in knee osteoarthritis population