Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2015) Volume 4, Issue 3
Background: We hypothesize that the combination of an mTOR inhibitor, sirolimus, with a well-known cytotoxic agent, cyclophosphamide, provides a well-tolerated and promising alternative treatment for advanced, differentiated thyroid cancers (DTC).
Methods: This retrospective review extracted data from patients treated for advanced DTC at the University of Michigan Comprehensive Cancer Center from 1995 through 2013. Fifteen patients treated with combination sirolimus and cyclophosphamide were identified as the sirolimus+cyp group. Seventeen patients treated with standard of care and enrolled in clinical trials were identified as the comparison group.
Results: The one-year progression free survival rate (PFS) was 0.45, 95% CI [0.26, 0.80] in the sirolimus+cyp population and 0.30, 95% CI [0.13, 0.67] in the comparison population. The hazard ratio for PFS from initiation of treatment was 1.47, 95% CI [0.57, and 3.78]. In patients treated as first line, one-year PFS rate was 0.57, 95% CI [0.30, 1.00] in the sirolimus+cyp group and relatively unchanged at 0.29, 95% CI [0.11, 0.74] in the comparison group. The hazard ratio for PFS for first line patients was 1.10, 95% CI [0.4, and 3.5]. In patients with 3 or fewer sites of metastases, the one year PFS was 0.58, 95% CI [0.33, 1.00] in the sirolimus+cyp group, and 0.37, 95% CI [0.17, 0.80] in the comparison group. The average number of toxicities was 0.87 in the sirolimus+cyp patients and 1.71 in the comparison group.
Conclusions: The combination of sirolimus and cyclophosphamide was generally well tolerated with similar progression free survival, highlighting its applicability in patients with limited options.
<Keywords: Thyroid cancer; Advanced differentiated thyroid carcinoma; Sirolimus; Cyclophosphamide
The incidence of thyroid cancer has increased faster than that of any other malignancy in recent years. The American Cancer Society estimates 62,980 cases of newly diagnosed thyroid cancer and 1890 deaths in 2014 in the United States [1-4]. Surgery is the primary mode of therapy for patients with advanced, differentiated thyroid cancers (DTC), with radioiodine therapy (RAI) and thyroid hormone suppression as adjunctive therapies. Once patients with widely spread progressive disease become refractory to RAI, they are amenable to treatment with systemic therapies, primarily with tyrosine kinase inhibitors (TKIs). Several drugs have been tested in DTC and are beginning to change the scope of how this disease is treated. Recently sorafenib has received FDA approval for use in RAI-refractory, DTC. Though TKIs provide prolonged intervals of disease-free progression, patients ultimately become resistant to such treatments. Hence, therapies targeting other molecular pathways such as the AKT/mTOR pathway are needed [5-8]. The Cancer Genome Analysis and pre-clinical studies have discovered up to 33 mTOR mutations that may confer pathway hyperactivity [9-11].
Currently, mTOR inhibitors have been approved in renal cell carcinoma and mantle cell lymphoma [12,13] but activation of mTOR pathway has been noted in follicular, medullary, and anaplastic thyroid cancer [14-17]. PI3K/AKT pathway genetic alterations have been reported in follicular thyroid carcinoma and papillary thyroid cancer, suggesting a role for mTOR signaling in thyroid neoplasia [18,19]. Other signaling molecules including RET/PTC rearrangements and RAS mutations can lead to the activation of the PI3K/AKT pathway [5-7,18-21]. Furthermore, studies have demonstrated that the AKT/mTOR pathway is particularly over-activated in human primary follicular cancer harboring the BRAFV600E mutation [22]. In theory, multiple mutations and genes have been implicated with the mTOR pathway, demonstrating the utility of mTOR inhibitors, such as sirolimus, as a therapeutic target for thyroid carcinomas [7-9,14-17].
Cyclophosphamide is an alkylating agent that is widely used in cancer treatment. Its action results in DNA damage and hastens cell death. Cyclophosphamide is among the most utilized drugs in chemotherapy, with FDA-approved indications in many different types of cancer including breast and ovarian carcinomas. Its role in thyroid cancer has not been well studied, though cyclophosphamide has been used in combination with vincristine and dacarbazine to treat advanced medullary thyroid cancer [23].
Due to the limited effective treatment options for advanced, iodine refractory, DTC, the combination of sirolimus and cyclophosphamide has been empirically used at the University of Michigan for the ease of administration with its oral formulation and its favorable toxicity profile. We hypothesize that this combination of a non-cell cycle specific alkylating agent with an mTOR inhibitor, targeting thyroid cancer on a molecular level, may lead to promising therapeutic advances.
Methods
Patient population
The sirolimus and cyclophosphamide (sirolimus+cyp) and comparison populations were extracted from a database of all patients treated for recurrent or metastatic, radioiodine (RAI)-refractory DTC at the University of Michigan Comprehensive Cancer Center from 1995 through 2013. There were a total of 2,460 patients treated for recurrent or metastatic, RAI refractory DTC in the initial database. EMERSE, a software tool, was utilized to create refined searches for the sirolimus+cyp and comparison patients. The search criteria were refined to include patients with follicular, papillary, and Hurthle cell carcinoma of the thyroid and exclude anaplastic, medullary, and undifferentiated carcinoma of the thyroid. A total of 2,182 patients were classified within this category. A significant portion of advanced DTC patients were initially being observed without active therapy due to a lack of progression of disease. When a disease progression occurred, patients were ideally started on clinical trials. Other patients were placed on the combination of sirolimus and cyclophosphamide therapy by clinician preference due to lack of clinical trials, progression on clinical trials, or ineligibility for clinical trials.
The chemotherapy medications of sirolimus and cyclophosphamide were entered into the search field to detect the sirolimus+cyp cohort. A total of 15 patients were identified, all of who had documented disease progression, as defined by RECIST criteria (24). Comparison group patients were identified as patients with advanced DTC with evidence of disease progression. The comparison population was actively enrolled in clinical trial regimens, which was the standard of care for disease progression. Both groups were considered advanced beyond the point of observation, necessitating chemotherapy. Three clinical trials were ongoing for patients with advanced, I-131 refractory DTC from 1995 to 2013. The trials were done sequentially without overlap. The terms “UMCC 2005-063”, “UMCC2010.0125”, “UMCC2009.086”, “sorafenib, “lenolidamide”, “lenalidomide”, “recentin”, “cediranib”, “revilimide”, “revlimid”, “revlamid”, “AG-013736” were used to identify the comparison group, yielding a total of 17 patients. There were a total of seven patients from the sirolimus+cyp group that crossed over with the comparison group, but the overlap was sequential.
This protocol was approved by the University of Michigan Institutional Board Review.
Disease progression
Computed tomography or magnetic resonant imaging of neck and chest were obtained at baseline. Tumor response was assessed every 8 weeks using the same imaging modality that was obtained at baseline. The RECIST was used to assess response and ≥20% increase in the sum of longest diameters of target lesions determined a progression event [24].
Statistical methods
The primary goal of this retrospective study was to evaluate the impact of the combination of sirolimus and cyclophosphamide on OS and PFS compared to existing targeted therapies in patients with advanced DTC.
The analysis included descriptive statistics and modeling. All eligible patients were included in the descriptive analysis. It was possible for a patient to be included in both the sirolimus+cyp cohort and the comparison cohort if that patient underwent both treatments at different time points. Baseline demographics and clinical characteristics were reported for the two groups. Frequency estimates for adverse events in the two groups were also reported. Two measures of treatment effect were used: overall survival (OS) and progression-free survival (PFS). For OS, time to death was defined as the time from initiation of treatment to death from any cause. For PFS, time to progression was defined as the time from initiation of treatment to time of disease progression or death from any cause. The Kaplan-Meier method was used to estimate curves for overall survival and for progression-free survival. One-year overall/progression-free survival probabilities were estimated using the Kaplan-Meier curves. In the sirolimus+cyp group where no events had occurred at one year, confidence intervals were calculated using the Clopper-Pearson method. A Cox-Proportional Hazards Model was used to estimate the hazard ratio of death/disease progression between the sirolimus plus cyclophosphamide cohort and all other patients. Confidence intervals for the hazard ratios were estimated using bootstrapping. The Cox model was applied to all patients, restricted to patients on first line treatment only, and restricted to all the patients with 3 or fewer sites of metastasis. All analysis was conducted using R v2.15.2.
Patient characteristics
The sirolimus+cyp population included 15 patients designated with advanced, RAI refractory DTC treated with sirolimus plus cyclophosphamide between 1995 and 2013. The comparison population included 17 patients on clinical trials for advanced RAI refractory DTC between 1995 and 2013. Patient age ranged from 38-79 and the median age in sirolimus+cyp population was 60 years and 62 years in the comparison population. The gender distribution was similar between the sirolimus+cyp and the comparison population (Table 1). Baseline performance status was assessed prior to treatment, the majority of which were ECOG 1. All comparison patients and fourteen of fifteen sirolimus+cyp patients received prior thyroidectomy. Approximately half of the patients received radioactive iodine (RAI) in both groups. The remainder of patients was deemed RAI-refractory upfront and thus not suitable for I-131 therapy. The combination of sirolimus and cyclophosphamide was first line in 47% of the sirolimus+cyp population, while the comparison group was treated with corresponding targeted therapies in clinical trials as first-line treatment in 82% of the patients. The comparison group comprised of patients treated with clinical trial medications with tyrosine kinase inhibitor activity. Three comparison patients were treated with Axitinib; eight comparison patients with sorafenib; six comparison patients with cedirinb/lenolidamide. All of the sirolimus+cyp population and comparison population had advanced disease with lung involvement at time of treatment initiation. Two of the sirolimus+cyp population patients had metastases to the brain that were successfully treated with radiation prior to the commencement of treatment, while none of the comparison population had brain involvement. Thyroglobulin levels were available for 13/15 sirolimus+cyp patients. Seven of the patients displayed an increase in thyroglobulin levels and five patients displayed a decrease in thyroglobulin levels during the treatment period; one patient had variable levels. In the comparison group, 14/17 patients had available thyroglobulin levels. Six of the patients displayed an increase in thyroglobulin levels and six patients displayed a decrease in thyroglobulin levels during the treatment period; two patients had variable levels. Overall, the baseline characteristics demonstrate that the sirolimus+cyp patients were at later stages of illness as evidenced by lack of patients with ECOG status 0 in this group. In addition, the sirolimus+cyp patients began therapy with higher risk disease with more Hurthle cell histology, number of brain metastases, and average number of metastatic sites.
| Characteristic | Sirolimus+cyp (n=15) | Comparison (n=17) | |
|---|---|---|---|
| Baseline Age | 60.3 (38-79) | 62.5 (52-71) | |
| Gender (%) | Male Female |
60.0 40.0 |
52.9 47.1 |
| Performance Status (%) | 0 1 2 |
0 86.7 13.3 |
17.6 70.6 11.8 |
| Histology (%) | Hurthle Papillary Follicular |
26.7 60.0 13.3 |
11.8 76.5 5.9 |
| Site (%)* | Lung Lymph Node Bone Neck Mediastinum Kidney Retina Brain Adrenal Liver |
100 73.3 46.7 40.0 6.7 6.7 6.7 13.3 6.7 0 |
100 47.1 35.3 29.4 11.8 0 0 0 11.8 5.9 |
| Treatment Therapy | Sirolimus/Cyclophosphamide Sorafenib Axitinib Cedirnib/Lenolidamide |
15 0 0 0 |
0 8 3 6 |
| Treatment Line (%) | First Second Third |
46.7 40.0 13.3 |
82.4 17.6 0 |
| Prior Thyroidectomy (%) | 93 | 100 | |
| Cumulative RAI Activity (miC) | 223.1 (8-500) | 293.3 (50-553) | |
| Avg No. Metastatic Sites | 3 (1-6) | 2.41 (1-5) | |
| Median No. Metastatic Sites | 3 | 2 | |
| Pts 3 or Fewer Metastatic Sites (%) | 67 | 77 | |
| *Some patients have metastases at multiple sites. Patients were included in all applicable groups. | |||
Table 1: Patient characteristics.
Toxicity
Toxicities are noted in Table 2. The most common toxicities in the comparison group were grade II/III hypertension associated with Cedirinib and Sorafenib (35%), grade II/III fatigue (35%), and grade III hand foot syndrome associated with sorafenib (18%). In the sirolimus+cyp population, the most significant toxicity was anemia secondary to cyclophosphamide, seen in 20% of patients. Notably, the average number of toxicities was 0.87 in the sirolimus+cyp patients and 1.71 in the comparison group.
| Toxicity | Sirolimus+cyp Patients (%) | Comparison Patients (%) |
|---|---|---|
| Anemia | 20.0 | 0 |
| Decrease Appetite | 6.7 | 5.9 |
| Infection | 6.7 | 0 |
| Leukopenia | 6.7 | 0 |
| Nausea | 6.7 | 0 |
| Neutropenia | 6.7 | 5.9 |
| Pancytopenia | 6.7 | 0 |
| Rash | 13.3 | 5.9 |
| Weight Loss | 6.7 | 5.9 |
| Diarrhea | 0 | 5.9 |
| Dizziness | 0 | 5.9 |
| Dyspnea | 0 | 5.9 |
| Fatigue | 0 | 35.3 |
| Dysphagia | 0 | 5.9 |
| Hand Foot Syndrome | 0 | 17.6 |
| Hypertension | 0 | 35.3 |
| Liver Function Abnormal | 0 | 5.9 |
| Mucositis | 0 | 17.6 |
| Pulmonary Embolism | 0 | 5.9 |
| Thrombocytopenia | 0 | 5.9 |
Table 2: Common toxicities.
It is important to recognize that the comparison population toxicities were clearly designated with respect to grade as the patients were part of clinical trials. The toxicities in the sirolimus+cyp group were not always described with reference to grade but explicit documentation was available with regards to dose reductions and dose interruptions. The patients were followed for a significant duration of time (median follow up of 31.9 months in sirolimus+cyp group and 18.7 months in the comparison group), although one cannot preclude the incidence of late onset toxicities.
Treatment tolerance
Both sirolimus+cyp and comparison populations had similar rates of dose reductions (68% vs 59%) and dose interruptions (68% vs 59%). Permanent drug cessation occurred in 24% of the comparison patients and in none of the patients in the sirolimus+cyp group (Table 3). Sirolimus was rarely associated with dose reductions (2/15 patients required brief dose reductions and interruptions due to rash and infection). The typical dose of cyclophosphamide on initiation was 100 or 150 mg Monday through Friday, every other week, and the median maximum tolerated dose of cyclophosphamide was 50 mg Monday through Friday, every other week. The typical dose of sirolimus on initiation was 4 or 6 mg daily and the median tolerated dose was 4 mg daily.
| Dose Tolerance | Sirolimus+cyp Patients | Comparison Patients |
|---|---|---|
| Dose Reduction (%) | 67.7 | 58.8 |
| Dose Interruption (%) | 67.7 | 58.8 |
| Permanent Interruption (%) | 0 | 23.5 |
Table 3: Dose tolerance.
Response to treatment
The one-year overall survival probability for the sirolimus+cyp group was 0.70, 95% CI [0.49, 1.0] and was 0.93, 95% CI [0.82, 1.0] for the comparison group (Figure 1). The hazard ratio between the sirolimus+cyp and comparison groups was 3.04, 95% CI [0.80, 11.6] (Figure 1). The OS and PFS were confounded by the fact that 7 patients in the sirolimus+cyp group did cross over with the comparison group, but the overlap was sequential. Of the patients that overlapped, the majority (5/7) were treated with clinical trial regimen as first line therapy and combination sirolimus plus cyclophosphamide as subsequent therapy. Almost half of the sirolimus+cyp population treatments were thus second line or third line therapies.
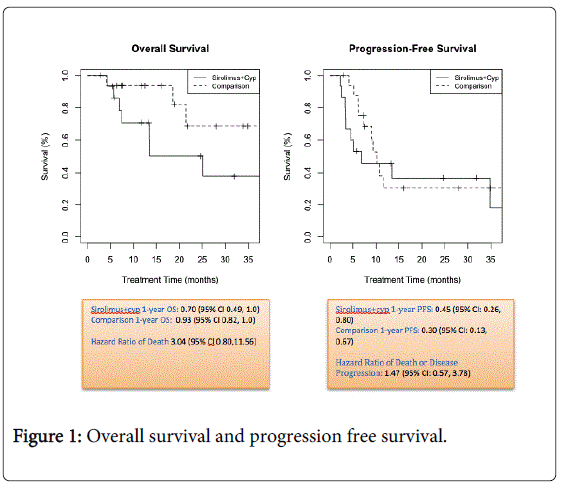
Figure 1: Overall survival and progression free survival.
Progression was noted in 11/15 sirolimus+cyp patients and 10/17 comparison patients. Progression was defined as RECIST criteria; events included disease progression and death. The one-year progression-free survival probability for the sirolimus+cyp group was 0.45, 95% CI [0.26, 0.80] and was 0.30, 95% CI [0.13, 0.67] for the comparison group (Figure 1). The hazard ratio was 1.47, 95% CI [0.57, 3.78] (Figure 1).
Two subgroup analyses were conducted in order to identify patients with less severe disease. The first focused on patients undergoing first line treatment only, and the second was limited to patients with less than or equal to 3 sites of metastasis. When restricted to patients on first line therapy, the one-year overall survival probability for sirolimus+cyp was 1.0, 95% CI [0.47, 1.0] and was 1.0, 95% CI [0.63, 1.0] for comparisons (Figure 2). The one-year progression-free survival probability was 0.57, 95% CI [0.30, 1.0] for sirolimus+cyps and was 0.29, 95% CI [0.11, 0.74] for comparisons (Figure 2). The hazard ratio of death between the sirolimus+cyp and comparison groups was 2.41, 95% CI [0.30, 7.21]. The hazard ratio of death/disease progression was 1.10, 95% CI [0.35, 6.16] (Figure 2).
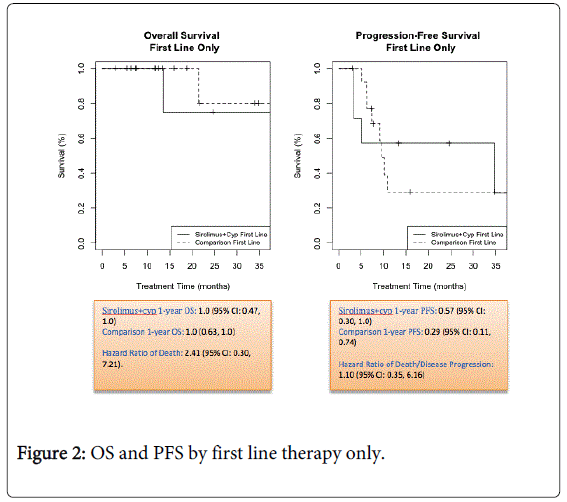
Figure 2: OS and PFS by first line therapy only.
In patients with 3 or fewer sites of metastases, the one-year overall survival probability was 0.77, 95% CI [0.54, 1.0] for the sirolimus+cyp group and was 1.0, 95% CI [0.63, 1.0] for the comparison group (Figure 3). The one-year probability of progression-free survival for the sirolimus+cyps was 0.58, 95% CI [0.33, 1.0] and was 0.37, 95% CI [0.17, 0.80] for the comparisons (Figure 3). The hazard ratio of death between the sirolimus+cyps and comparisons was 2.83, 95% CI [0.34, 6.34], and the hazard ratio of death/disease progression was 1.35, 95% CI [0.45, 4.76] (Figure 3).
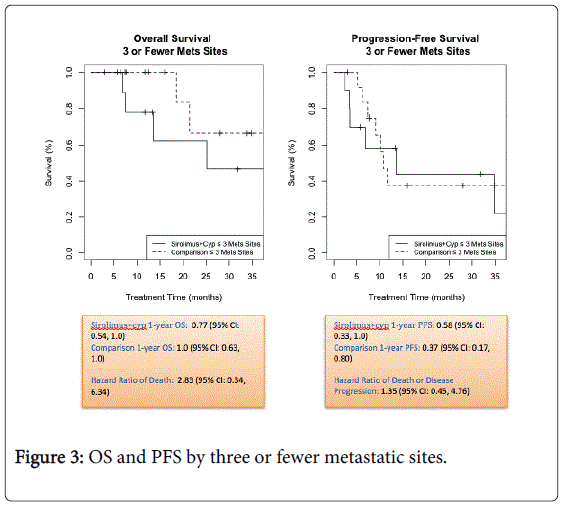
Figure 3: OS and PFS by three or fewer metastatic sites.
We evaluated the efficacy and safety of a widely known cytotoxic drug, cyclophosphamide, with a specific molecular targeted inhibitor, sirolimus, a combination that has been studied in other solid tumors, including soft tissue sarcomas [25,26]. The rationale for this combination stems from its favorable toxicity profile and ease of administration through an oral formulation. Additionally, preclinical data demonstrates the interplay of the mTOR pathway in differentiated thyroid carcinomas [14-17]. Currently, sorafenib and doxorubicin are the only FDA approval agents for the treatment of advanced, iodine refractory DTC [27-31]. Doxorubicin is rarely used and once patients fail treatment on sorafenib, their only option is to enroll onto clinical trials. But, due to a paucity of available trials and strict eligibility criteria, patients are left with few possibilities for effective therapy.
This retrospective study suggests an alternative treatment strategy with efficacy that is perhaps similar to that of other targeted therapies in terms of progression free survival. Amongst all patients, the hazard ratio of disease progression or death was 1.47, 95% CI [0.57, 3.78]. In addition, the one-year progression-free survival probabilities were similar between the sirolimus+cyp group and comparison group. This does not give evidence of a difference in the hazard of progression between the two groups. In contrast, the hazard ratio of death between sirolimus+cyps and comparisons was 3.04, 95% CI [0.80, 11.56], and the one-year survival probabilities for sirolimus+cyps, 0.70, 95% CI [0.49, 0.99], and comparison, 0.93, 95% CI [0.82, 1.0], suggest that the sirolimus+cyp group may have increased risk of death compared to the comparison group. However, it is important to note the differences in baseline characteristics between the sirolimus+cyp and comparison groups, which suggest that the sirolimus+cyp groups may have had more advanced disease. Two of the 15 patients in the sirolimus+cyp group had metastases to the brain, portending poor prognosis, while none of the comparison group patients had brain metastases. These two patients were observed to have a PFS of only 3-5 months. Taking this into consideration, one can speculate that the PFS could be improved in patients with fewer, less aggressive sites of metastases. Although further studies are needed, this suggests that an increased risk of death in the sirolimus+cyp group may be attributable to more advanced disease at baseline.
Collectively phase II studies with sorafenib in advanced DTC patients report PFS intervals of 6-10 months [29,30]. These findings were confirmed by Brose et al. in a large, multi-center, multi-national randomized control trial (DECISION) of sorafenib versus placebo, reporting a PFS of 10.8 months with sorafenib [31,32]. Most recently the SELECT trial has noticed promising data with the TKI, Lenvatinib, however the side effect profile is concerning with 40% of patients undergoing treatment related side effects [33].
Furthermore, we observed an interesting finding in two sub groups - namely, patients treated as first line treatment with the combination of sirolimus and cyclophosphamide and patients with fewer sites of metastases on initiation with sirolimus and cyclophosphamide. Focusing on the sirolimus+cyp group of patients with metastases limited to less than or equal to 3 sites, we demonstrate a greater one-year progression-free survival probability in the sirolimus+cyp group compared to the comparison group. Additionally, the hazard ratio of disease progression/death indicates little difference between the sirolimus+cyp and comparison group.
In addition, patients treated as first line showed an encouraging response with one-year progression free survival probability for the sirolimus+cyps. One could speculate that therapy in a treatment naïve patient with fewer sites of metastases would naturally produce better results, partly due to better baseline prognostic factors. However, this same benefit was not seen in the comparison patients with similar characteristics. The one-year PFS probability in comparison patients restricted to first line was nearly half that of sirolimus+cyp patients. Furthermore, the one-year PFS probability of comparison group patients as first line remains relatively unchanged from one year PFS probability in patients with any line of therapy.
Although 83% of patients were first line treatment in the comparison group, the one-year PFS probability was still only 0.29, 95% CI [0.11, 0.74], suggesting that sirolimus and cyclophosphamide may have sustained responses in patients treated early and first line. Our sirolimus+cyp supports the association of the mTOR pathway with thyroid cancer tumor-genesis [10,14-17]. It proposes the utility of mTOR inhibitors in advanced RAI-refractory thyroid cancer and guides future investigations in molecular oncology and targeted therapy [8,9].
In the DECISION study the most notable adverse event was, hand foot syndrome (76% patients), with 20% experiencing grade 3/4 toxicity [32]. In the SELECT study, there were similar side effect profiles with the TKI, Lenvatinib. Hypertension was noted in 67% of patients with discontinuation of the drug in 14% of patients [33]. Within our cohort, the average adverse event rate was lower in our sirolimus+cyp group compared to the comparison patients. None of the patients in the sirolimus+cyp group required discontinuation of the drug due to adverse effects, a stark comparison to the 25% comparison group patients that required permanent cessation of the clinical trial medication. This suggests that this regimen is largely well tolerated. Of the patients that sustained the most common toxicity of anemia, intermittent IV iron transfusions for those who were iron deficient were sufficient to curb the symptoms and resume the medication.
The limitations of our study stem, predominantly, from the small number of patients and the retrospective nature of this investigation. Due to the size of the study, our observations were not statistically significant and our sub group analysis for first line treatment was based on seven and fourteen patients in the sirolimus+cyp and comparison groups, respectively. Additionally, the comparison group was not uniformly the same in terms of treatment and the sirolimus+cyps and comparisons were not evenly matched by age, sex, or extent of disease. As our study combination therapy was not part of a randomized controlled trial, the adverse effects may have been under-reported. However, patient charts were scrutinized to identify drug interruptions and permanent drug cessation. Clinically significant side effects were carefully monitored for and addressed in the documentation. Furthermore, a thorough search of side effects included in the chart was undertaken to minimize any overlooked and under-reported adverse effects. Although long term side effects of the combination drug could not be effectively evaluated, it is reassuring to note that a subset of the study patients were successfully treated for years without consequence. Due to the crossover of our patients from sirolimus+cyp to the comparison group, they are not independent sets of patients. Through the use of the bootstrap we were able to account for this in the estimates of the hazard ratios and the resulting wider confidence intervals.
In summary, our study emphasizes the promising role of mTOR inhibitors in combination with cytotoxic agents in treatment of advanced RAI-refractory thyroid carcinomas. Future prospective trials are needed to help ascertain the true risks, benefits, and quality of life questions that this investigation raises.
Dr. Haymart is supported by NIH 1K07CA154595-02. Support was provided by the Punya Thyroid Cancer Research Foundation