Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 1
Purpose: The purpose of this study was to clarify how sleep breathing indices and airway morphology vary according to skeletal classification and the relationships between airway morphology and sleep breathing indices.
Method: Forty-four non-syndromic female Japanese patients, who were diagnosed with jaw deformities and underwent surgical orthodontic treatment were enrolled in this study. Using the Alice 5 diagnostic sleep system (Philips Respironics; Murrysville, PA), the apnea hypopnea index (AHI), apnea index (AI), and 4% oxygen desaturation index (4%ODI) were evaluated in each patient before they underwent orthognathic surgery. The following dimensions were measured on 2D CT images: the cross-sectional area at the level of the hard palate (HP), the cross-sectional area at the top of the uvula (TU), the cross-sectional area at the base of the tongue (BE). The following volumes were measured on 3D CT images: the volume of the upper airway (total volume), the volume of the region between the level of the hard palate and the top of the uvula (HP- TU volume), the volume of the region between the top of the uvula and the base of the epiglottis (TP-BE volume).
Result: There were no significant differences in airway morphology or sleep breathing indices among the three groups. Negative correlations were detected between HP-TU volume and 4%ODI, and between the HP area and AHI (p<0.05).
Conclusion: Our results establish that upper airway morphology also has important effects on the nocturnal breathing of jaw deformity patients.
Keywords: Sleep breathing indices; Jaw deformities; Airway
Orthognathic surgery is performed to correct congenital and acquired jaw deformities. Guilleminault et al. [1] reported that obstructive sleep apnea syndrome (OSAS) can occur after mandibular setback surgery. Subsequently, several researchers have described the airway changes that occur after orthognathic surgery [2-4]. For example, mandibular setback surgery can narrow the pharyngeal airway space (PAS). However, it is unclear how jaw deformities affect sleep breathing indices.
It is generally considered that patients with mandibular retrognathism (skeletal class 2) have smaller airways than patients with mandibular prognathism (skeletal class 3). However, no detailed consensus has been reached regarding how airway morphology differs among patients with skeletal class 1, 2, and 3 relationships [5,6].
Computed tomography (CT) enables us to evaluate airway morphology three-dimensionally. We have already reported the optimal threshold levels for evaluating airway morphology with CT [7]. The purpose of this study was to clarify how sleep breathing indices and airway morphology vary according to skeletal classification and the relationships between airway morphology and sleep breathing indices.
Forty-four non-syndromic female Japanese patients, who were diagnosed with jaw deformities and underwent surgical orthodontic treatment at Yamaguchi University Hospital from July 2008 to December 2011, were enrolled in this study.
Their mean age at the time of the CT acquisition was 23.7 ± 8.2 years (Table 1), and their mean body mass index (BMI) was 19.9 ± 2.0 kg/m2. The patients were divided into three groups based on their ANB angles; i.e., 14 patients whose ANB angles ranged from 0 ° to 4 ° were placed in the skeletal class 1 group, 17 patients whose ANB angles were greater than 4 ° were categorized into the skeletal class 2 group, and 13 patients whose ANB angles were less than 0 ° were included in the skeletal class 3 group.
| Gender | Age(y) | BMI(kg/m2) | |
|---|---|---|---|
| Skeletal 1(n=14) | female | 25.5± 9.3 | 18.9± 1.9 |
| Skeletal 2(n=17) | Female | 22.6± 6.1 | 19.6± 1.9 |
| Skeletal 3(n=13) | Female | 23.1± 9.4 | 21.2± 1.8 |
Table 1: Distribution of subjects.
Patients with a history of breathing problems were excluded from the study. The study was approved by the Ethics Committee of Yamaguchi University Hospital, and all participants signed informed consent forms.
Examination of breathing during sleep
Using the Alice 5 diagnostic sleep system (Philips Respironics; Murrysville, PA), the apnea hypopnea index (AHI), apnea index (AI), and 4% oxygen desaturation index (4%ODI) were evaluated in each patient before they underwent orthognathic surgery. The indices were defined according to standard criteria.
The AI and HI measure the number of pre-defined events per hour of sleep. The pre-defined events were as follows: AI: a = 90% drop in the air temperature detected by an oronasal thermal sensor compared with the baseline, lasting for = 10 sec; HI: a = 50% reduction in nasal pressure from the baseline and an associated = 4% desaturation from the pre-event baseline. AHI was defined as the sum of the AI and HI [8]. The indices were measured in various body postures.
Measurements of airway morphology
A CT machine (SOMATOM Definition SIEMENS Co. Forchheim, Germany) and a multi-slice helical technique were employed in this study. All CT scans were acquired with the subjects in centric occlusion, and the slice plane was oriented parallel to the Frankfort horizontal (FH) plane.
The CT images were taken before the patients underwent orthognathic surgery. The slice thickness of the reconstructed images was 0.6 mm. The CT images were imported into a personal computer, and the airway was reconstructed using CT analysis software (Mimics version 14.12). The upper and lower thresholds used to produce 3D images from the CT data were -470 HU and -1024 HU, respectively [7].
The level of the hard palate and the base of the epiglottis were used as the upper and lower boundaries of the airway, respectively. The pharyngeal walls were used as the lateral and posterior boundaries of the model. The anterior boundary was defined by the soft palate, the base of the tongue, and the anterior wall of the pharynx.
The following dimensions were measured on 2D CT images: the cross-sectional area at the level of the hard palate (HP), the cross-sectional area at the top of the uvula (TU), the cross-sectional area at the base of the tongue (BE) (Figure 1).
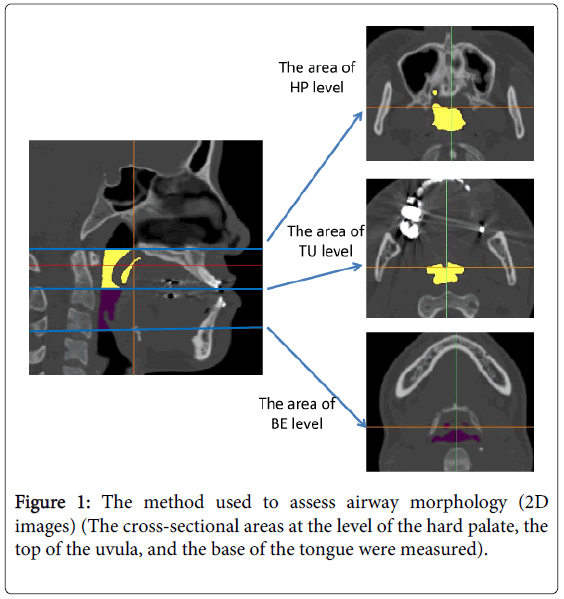
Figure 1: The method used to assess airway morphology (2D images) (The cross-sectional areas at the level of the hard palate, the top of the uvula, and the base of the tongue were measured).
The following volumes were measured on 3D CT images: the volume of the upper airway (total volume), the volume of the region between the level of the hard palate and the top of the uvula (HP-TU volume), the volume of the region between the top of the uvula and the base of the epiglottis (TP-BE volume) (Figure 2).
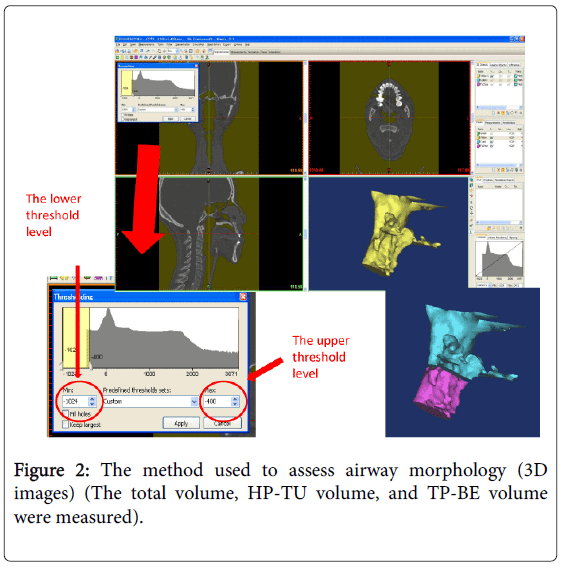
Figure 2: The method used to assess airway morphology (3D images) (The total volume, HP-TU volume, and TP-BE volume were measured).
Statistical analysis
SPSS software for Windows, version 11.0 (SPSS, Chicago, IL), was used for all statistical analyses. Descriptive statistics, including means and standard deviations for each group, were calculated. One-way analysis of variance was used to compare the airway morphologies and sleep breathing indices of the skeletal class 1, 2, and 3 groups. In addition, Spearman’s rank correlation coefficients were used to evaluate the correlations between airway morphology and the sleep breathing indices. Values of p<0.05 were considered statistically significant.
There were no significant differences in airway morphology or sleep breathing indices among the three groups (Tables 2 and 3). Negative correlations were detected between HP-TU volume and 4%ODI and between the HP area and AHI (p < 0.05) (Table 4).
| skeletal 1 | skeletal 2 | skeletal 3 | P value | |
|---|---|---|---|---|
| The total volume (mm3) | 15669.9 ± 5248.2 | 13088.7 ± 6059.8 | 11970.5 ± 4892.4 | 0.2 |
| The volume of HP-TU(mm3) | 8474.2 ± 3725.5 | 6143.5 ± 2811.6 | 5906.4 ± 3265.4 | 0.08 |
| The volume of TP-BE(mm3) | 7083.6 ± 2237.2 | 6733.1 ± 3432.2 | 5970.6 ± 1970.4 | 0.55 |
| The area of HP level (mm2) | 590.9 ± 172.5 | 511.9 ± 170.3 | 442 ± 238.2 | 0.14 |
| The area of TU level (mm2) | 242.5 ± 115.6 | 180.1 ± 103.7 | 216.6 ± 112.6 | 0.29 |
| The area of BE level (mm2) | 298.6 ± 77.3 | 273 ± 89.8 | 240.8 ± 97.6 | 0.24 |
Table 2: The relationship between airway morphology and skeletal morphology (one-way analysis of variance).
| skeletal 1 | skeletal 2 | skeletal 3 | P value | |
|---|---|---|---|---|
| AI (/hr) | 0.8 ± 1 | 1.3 ± 1.6 | 0.8 ± 0.8 | 0.4 |
| HI(/hr) | 0.007 ± 0.03 | 0.006 ± 0.02 | 0.6 ± 1.2 | 0.05 |
| AHI(/hr) | 0.8 ± 1 | 1.3 ± 1.6 | 1.3 ± 1.4 | 0.55 |
| 4%ODI(/hr) | 0.2 ± 0.2 | 0.5 ± 0.6 | 0.6 ± 0.9 | 0.16 |
Table 3: The relationship between skeletal morphology and SBI (oneway analysis of variance).
| AI | HI | AHI | 4%ODI | |
|---|---|---|---|---|
| The total volume | 0.13 0.39 |
0.05 0.74 |
0.17 0.24 |
0.22 0.14 |
| The volume of HP-TU | 0.23 0.12 |
0.12 0.4 |
0.26 0.08 |
0.33 0.02* |
| The volume of TU-BE | 0.05 0.71 |
0.03 0.82 |
0.08 0.58 |
0.16 0.28 |
| The area of HP level | 0.23 0.12 |
0.18 0.22 |
0.29 0.04* |
0.19 0.2 |
| The area of TU level | 0.2 0.17 |
0 0.96 |
0.22 0.13 |
0.28 0.06 |
| The area of BE level | 0 0.98 |
0.09 0.55 |
0.06 0.67 |
0.15 0.3 |
Table 4: The correlation between airway morphology and SBI (Spearman’s correlation coefficient by rank *p<0.05).
A number of reports have described the airway morphology of Asian patients with jaw deformities [5,6]. Kikuchi [5] reported that the volume of the lower part of the pharyngeal space is increased in patients with mandibular prognathism (skeletal class 3). On the other hand, Hong et al. [6] reported that the volume of the upper part of the pharyngeal space is greater in patients with skeletal class 3 malocclusion than in those with other malocclusions and that the volume of the upper part of the pharyngeal airway is significantly correlated with the anterior position of the mandible. Hence, previous studies have reported different findings regarding the relationship between airway morphology and mandibular position. In our study, neither airway volume nor any of the sleep breathing indices displayed significant differences among the skeletal class groups. We think that this was because most patients with jaw deformities are young. However, mandibular retrognathism is a morphological feature of OSAS patients; therefore, we will continue to follow-up the airway morphology of the patients in this study.
Secondly, the relationships between airway morphology and sleep breathing indices were examined in the whole subject population because there were no significant differences in sleep breathing indices or airway volume among the skeletal class groups. Many studies have evaluated the airway morphology of OSAS patients [9-12]. There are two methods for assessing the airway morphology of OSAS patients using CT. The first method is to examine the distance from the level of the hard palate to the base of the epiglottis [9-11]. The second method is to evaluate the position of the cervical spine [4,12]. Muto et al. [13] reported that the degree of craniocervical inclination affected the dimensions of the PAS. Although it is important to understand this relationship, investigating it raises ethical problems because it requires the acquisition of several CT scans. In addition, we considered that craniocervical inclination would not vary much in our study because all of the CT scans were taken in the supine position; therefore, we evaluated airway morphology by measuring the distance from the level of the hard palate to the base of the epiglottis.
As a result, we found that the HP-TU volume displayed a negative relationship with 4%ODI, a sleep breathing index. Some other researchers have reported similar results [14,15]. Tsuiki et al. [14] reported that the success of oral appliance therapy for OSAS depended on anterior titration of the patient’s mandibular position to enlarge the upper airway. Similarly, Gao et al. [15] reported that oral appliance therapy for OSAS works by enlarging the upper airway, mainly the region at the back of the soft palate, and keeping the airway open. Accordingly, many researchers have reported that upper airway morphology is closely related to OSAS. However, these studies only involved OSAS patients. Our results establish that upper airway morphology also has important effects on the nocturnal breathing of jaw deformity patients.
This work was supported by Grant-in-Aid for Scientific Research (C) (25293410) and Young Scientists (B) (25861954) from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) and Japan Society for Promotion of Science (JSPS) KAKENHI Grant Number (25293410 and 25861954).