Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Case Report - (2013) Volume 1, Issue 2
Hyperkalaemia is a very rare complication associated with zoledronic acid. We report the case of a patient with hyperkalaemia recalcitrant to treatment. A 72 year-old woman who was diagnosed with post-menopausal severe osteoporosis following a bone mineral density scan was treated with a single dose of zoledronic acid infusion. After 3 weeks, the patient’s serum potassium level increased from a baseline of 3.8 mmol/L to 5.9 mmol/L. Renal function was normal and all other possible causes of hyperkalaemia were excluded. She was started on oral sodium polystyrene sulfonate 15 g twice daily. Her serum potassium level remained persistently elevated over the next 9 weeks before it finally returned to a normal level on the 13th week after zoledronic acid infusion. We recommend close monitoring and prompt treatment of hyperkalaemia should it occur.
<Keywords: Zoledronic acid; Bisphosphonate; Hyperkalaemia
Bisphosphonates are commonly used for the treatment of diseases with excessive bone resorption. Zoledronic acid is a nitrogencontaining bisphosphonate that is administered intravenously. It is easier to administer due to its once per annum dosing and is the most efficacious of the commercially available bisphosphonates [1,2]. More recently, there is increasing evidence to suggest that zoledronic acid exhibits anti-tumour activity, in addition to their anti-osteoclast activity [3]. It is available as two licensed intravenous products: 1) Reclast® (zoledronic acid 5 mg/100 mL once yearly) for Paget’s disease of bone, prevention and treatment of osteoporosis in post-menopausal women and men; and 2) Zometa® (zoledronic acid 4 mg/5 mL, given as an infusion every 3 to 4 weeks) for the treatment of multiple myeloma or bone metastase in conjuction with standard chemotherapy, tumourinduced hypercalcaemia and prevention of skeletal-related events such as pathological fractures and spinal compression [3,4].
Zoledronic acid has been approved for use in the United States since 2001. However, it may have side effects yet to be elucidated. While we may be familiar with more common side effects such as renal toxicity, flu-like symptoms (bone pain, arthralgia, fever, nausea, chills), atrial fibrillation and hypocalcaemia, there have been increasing number of case reports describing rare but significant complications associated with zoledronic acid use [5,6]. These include osteonecrosis of the jaw, orbital inflammatory disease, transient changes in thyroid function tests, transient hepatotoxicity, flare up of hand osteoarthritis and lifethreatening hyperkalaemia [7-12].
There is only one reported case of hyperkalaemia associated with zoledronic acid use in the literature. We report a second case of hyperkalaemia associated with zoledronic acid use and draw comparisons between the two cases.
Our patient is a 72 year-old woman who has no significant past medical history. She presented to us with a comminuted intra-articular fracture of the left calcaneum and subsequently underwent open reduction internal fixation of the fracture. There was no complication during the peri-operative period. Post-surgery, a bone mineral density scan was ordered which revealed post-menopausal severe osteoporosis. The pharmaceutical company’s recommendations for renal assessment were done prior to administering zoledronic acid and the results were normal. Her serum creatinine was 55 umol/L and estimated glomerular filtration rate was 61.5 ml/min. A single dose of zoledronic acid infusion (5 mg/100 mL over 15 minutes) was given 6 weeks after her surgery and she was followed up with routine screening of her renal function. 3 weeks after the zoledronic acid infusion, the patient’s serum potassium level increased from a baseline of 3.8 mmol/L to 5.9 mmol/L (normal range 3.3 to 4.9 mmol/L). Other blood tests done showed the following results: serum creatinine level of 66 umol/L, urea level of 4.1 mmol/L, sodium level of 144 mmol/L, glucose level of 5.7 mmol/L, bicarbonate level of 25.7 mmol/L, calcium level of 2.35 mmol/L, 25 Hydroxyvitamin D level of 36.1 ug/L, parathyroid hormones level of 3.1 pmol/L, albumin level of 37 g/L, myoglobin level of <21.0 ug/L, creatine kinase level of 62 U/L and creatine kinase-MB level of 1.0 ug/L, which were all within normal range. Standard urinalysis did not reveal any urinary tract infection, proteinuria or glycosuria. 24 hours urinary potassium level was 45 mmol/day. Her blood pressure was normal and the blood sample was not haemolysed, which may falsely elevate the serum potassium level. She was referred to renal and endocrine physicians to rule out other causes of hyperkalaemia, including renal causes, hypercortisolism, hypoaldosteronism and thyroid diseases. A detailed dietary history was taken to exclude any recent change in diet involving potassium-rich food. She was also not on any other medications, nor was she taking any Traditional Chinese Medicine or supplements. Zoledronic acid was the only medication recently administered which could have accounted for the hyperkalaemia. All other possible causes of hyperkalaemia were excluded in our patient.
As our patient was clinically asymptomatic and had no ECG changes, she was started on oral sodium polystyrene sulfonate 15 g twice daily for the treatment of her hyperkalaemia. Her serum potassium level remained persistently elevated over the next 9 weeks before it finally returned to normal level on the 13th week after zoledronic acid infusion (Figure 1).
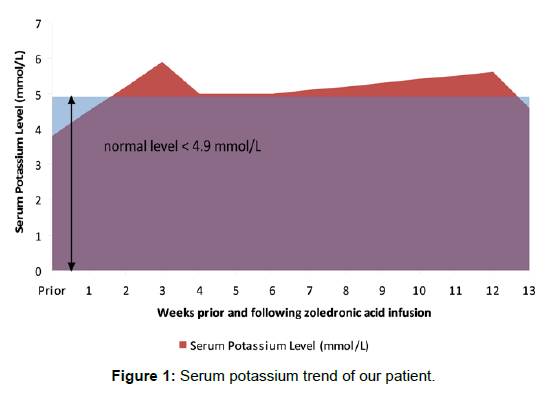
Figure 1:The barriers to falls model.
Zoledronic acid is a nitrogen-containing bisphosphonate. Like other bisphosphonates, it has a high affinity for hydroxyapatite crystals of the bone, with preferential localization at sites with high bone turnover [1]. During bone resorption, the acidic pH of the subcellular space beneath the osteoclasts causes the dissolution of bone mineral. Bisphosphonates are released and internalized by osteoclasts. Once internalized, it acts by inhibiting farnesyl diphosphate synthase, thereby altering several important processes for osteoclast function [13]. In vitro studies have shown that zoledronic acid has the highest affinity for hydroxyapatite crystals and it appears to inhibit farnesyl diphosphate synthase 3-, 7-, 17- and 67-fold more effectively than risedronate, ibandronate, alendronate and pamidronate, respectively [1,2].
Zoledronic acid is not metabolized in humans and its excretion occurs almost exclusively by the kidneys through glomerular filtration. Urinary excretion is independent of infusion duration and dose but shows a correlation with creatinine clearance. Within 24 hours after its administration, up to 41% of the dose infused will be excreted unmetabolized in the urine and approximately 60% of the dose is retained in the skeleton [14]. The relatively long duration of action of zoledronic acid is attributable to its high binding affinity to bone mineral. Bone remodeling processes will slowly release and recycle retained zoledronic acid back into the systemic circulation, for excretion through the kidneys and re-deposition across bone surfaces at lower concentration than following the initial dose [15]. The redeposited zoledronic acid will then undergo a similar, continuous cycle of release and recycle back into the systemic circulation. While the early elimination half-life of zoledronic acid is 1.87 hours, the terminal elimination half-life may be as long as 7 to 189 days [16,17].
While hyperkalaemia is documented as a rare side effect of zoledronic acid on the producing company database, there were no cases of hyperkalaemia reported in the literature until recently. Panteliou et al. first reported a case of life threatening hyperkalaemia following a single 5 mg dose of zoledronic acid infusion for the treatment of Paget’s disease [12]. The patient had a history of ischaemic heart disease and his condition was complicated by cardiac arrest 10 days following the zoledronic acid infusion. Despite a normal renal function, he had persistent hyperkalaemia throughout his hospitalization stay. He passed away 26 days after his cardiac arrest.
Our patient also had hyperkalaemia following a single 5 mg dose of zoledronic acid infusion and her renal function was also normal. However, unlike the previous patient described, our patient did not have any history of ischaemic heart disease and she was suffering from osteoporosis rather than Paget’s disease.
Using the two cases, we postulate that hyperkalaemia associated with zoledronic acid infusion: 1) can occur in patients with normal renal function and the exact pathogenesis has yet to be elucidated; 2) can occur in patients with no other co-morbidities except isolated, agerelated osteoporosis and 3) can be recalcitrant to treatment and last as long as 13 weeks after the zoledronic acid infusion. However, further product surveillance will be required to validate these postulations.
In conclusion, hyperkalaemia is a rare complication associated with zoledronic acid use and it can be recalcitrant to treatment. This may be due to the prolonged half-life of zoledronic acid in the human body. Continued product surveillance will be necessary to clarify the pathogenesis and formulate good management guidelines. Until more data is available, we recommend that zoledronic acid should be used with great caution in patients with renal impairment, cardiac arrhythmia and previous ischaemic heart disease. In bisphosphonate naïve patients, renal function and serum electrolytes should be checked before starting zoledronic acid, as well as regularly and up till 13 weeks after starting zoledronic acid. If hyperkalaemia occurs, aggressive and prolonged treatment to reduce the serum potassium level may be required depending on the patient’s clinical presentation.
The authors thank Yanni Xu for her technical support.