Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 3
Background: Students' mental stability can be restored by comfort from a familiar home environment and support from their parents. However, many boarding students face various psychological and physical problems by themselves and cannot benefit from home care. The goal of this study is to examine psychological and emotional stress among students living in a dormitory.
Methods: Between October and November 2014, 124 students (74 male, 50 female) were enrolled at Korea International School (KIS) in Jeju, South Korea. By the Zung Selfrating Depression Scale (ZSDS), they were divided into two groups: the normal group and the depression group. I evaluated each group under the following circumstances: (1) individual school life, (2) physical health, (3) factor analysis of ZSDS. The Statistical Package for Social Sciences Software (SPSS-version 21) was used to analyze the data.
Results: 45.9% of all enrolled students scored in the mild to moderated depression range. Female students had a more prevalent depression rate (female: 54%, male: 41%). There was nearly no statistical difference in physical symptoms, except for dyspepsia, arthralgia, and lower back pain in the normal and depression groups respectively (P<0.05). The normal range group students had more study and exercise time. In the factor analysis of ZSDS, the depressive group had a more manifest depressed mood and 50 percentage higher ZSDS items score than the normal group: core depressive factor, anxiety factor.
Conclusions: Our study showed there was nearly no difference in physical symptoms between both groups. However, it informed that the group having depression has more problems with motor symptoms because the group lacks an adequate amount of exercise due to psychological instability. In addition, this study also showed that mood disturbance was clearly more intense while the cognitive functions related to academic performance were proven not to be problematic in the depressive group.
Keywords: Stress; Zung self-rating depression scale; High school students; Dormitory
Famous private boarding high schools are granted privileges to university entrance. However, since these boarding students are exposed to uncertainties in the future, they experience emotional instability and are more reserved and inward looking during the period of university entrance examinations, manifesting feelings of anxiety and distress. Furthermore, senior year of high school is a transition time from being an adolescent to being an adult, and they seek to fulfill individuality, as well as seek and build close and social relationships with other students [1].
Most students regain their psychological stability while living at home with their parents. However, boarding school students have to adjust to living away from the security of a family and away from parental guidance. Therefore, boarding students find psychological and physical problems because they do not receive care from home. For many boarding students, the separation from home for the first time may create feelings of doubt, confusion, and anxiety [2]. In the harassed mental symptom of boarding students, loneliness is the most terrible problem. They were overwhelmed by a longing for warm-hearted family loving. If they get over this process, loneliness leads an individual to achieve deeper self-awareness, a time to be creative, and an opportunity to attain self-fulfillment and to explore the meaning of life [3]. However, not every boarding student is psychologically mature enough to convert their loneliness to positive outcomes. Most outstanding students learn how to deal with the attachment and separation processes of interpersonal situations in normal psychological growth and to create a unique self-identity. However, those who fail to learn how to manage stressful situations suffer from unpleasant and distressing consequences due to their social and emotional loneliness [4].
In addition, unresolved loneliness can provide a source for depressive episodes. Depression can be manifested with a loss of interest, depressed mood, psychic anxiety, somatic anxiety, altered appetite and sleep, and painful physical symptoms [5]. Students with depressive symptoms can affect all areas of functioning including motivation, concentration, feelings of self-worth and mood [6]. During one’s senior year, which is considered to be the most crucial period of one’s life, various symptoms induced from depression may cause detrimental results. Thus, it is crucial to examine the psychological status of students who are in this important period of their lives. In this respect, the importance of this study lies in understanding differences between normal and depressive groups of students and intervening major issues for them.
The aim of this study was to investigate the prevalence of depressive students and the physical and mental symptoms difference among normal and depressive students within a dormitory.
A cross-sectional study design was applied. The research population consists of 9th, 10th and 11th grade residential students in Korea International High School (KIS) students in Korea. A total of 124 dormitory students were enrolled in this study between October and November 2014. During the first stage, we conducted the presentation of written informed consent. For the second stage, we received the Zung Self-rating Depression Scales (ZSDS). Students were then divided into the normal and depression groups. Individual groups answered a questionnaire comprised of questions covering individual school life style (breakfast, snack, daily sleep time, daily class study time, daily self-study time, daily exercise time), physical status (neurologic, ophthalmic, auditory, respiratory, cardiovascular, gastrointestinal, urologic, dermatologic), and mental status.
We developed individual school life style items [7] and a physical symptom checklist based on a previous research study [8]. The ZSDS is a self-reported 20-item measure of the symptoms of depression. Items are ranked from 1-4, with higher scores corresponding to more frequent symptoms. Depression items score were scored as follows; 1=a little of the time, 2=some of the time, 3=a good part of the time, 4=most of the time [9,10]. The worst psychological condition is defined to have the highest score of 80 and the best condition is interpreted as the lowest score of 20. Total scores on the ZSDS indicated the level of depressive symptoms that may be of clinical relevance. The ZSDS were interpreted as follows: normal range (20-44), mildly depressed (45-59), moderately depressed (60-69), severely depressed (70 and above). A ZSDS score of ≥50 was considered indicative of clinical depression.
Normal and depressive groups were analyzed by 4 subgroups of ZSDS. The subgroups were divided with factor 1 to factor 4 [11]. Factor 1 was composed of 8 questionnaire items of ZSDS: item 1 (depressed affect), item 3 (crying spells), item 6 (decreased libido), item 14 (hopelessness), item 17 (personal devaluation), item 18 (emptiness), item 19 (suicidal rumination), item 20 (dissatisfaction). Factor 2 was composed of 4 questionnaire items of ZSDS: item 11 (confusion), item 12 (psychomotor retardation), item 16 (indecisiveness), item 10 (fatigue). Factor 3 was composed of 3 questionnaire items of ZSDS: item 4 (sleep disturbances), item 13 (psychomotor agitation), item 15 (irritability). Factor 4 was composed of 3 items of ZSDS: item 5 (decreased appetite), item 7 (weight loss), item 9 (tachycardia).
The Statistical Package for Social Sciences Software (SPSS-version 21), chi-square test was used to analyze the data. Means and standard deviations were calculated for sub-scale scores of each group. The p-value of <0.05 were considered the level of statistical significance difference.
A total of 124 KIS students answered the study survey. The study subjects’ stratified characteristics are shown in Figures 1 and 2.
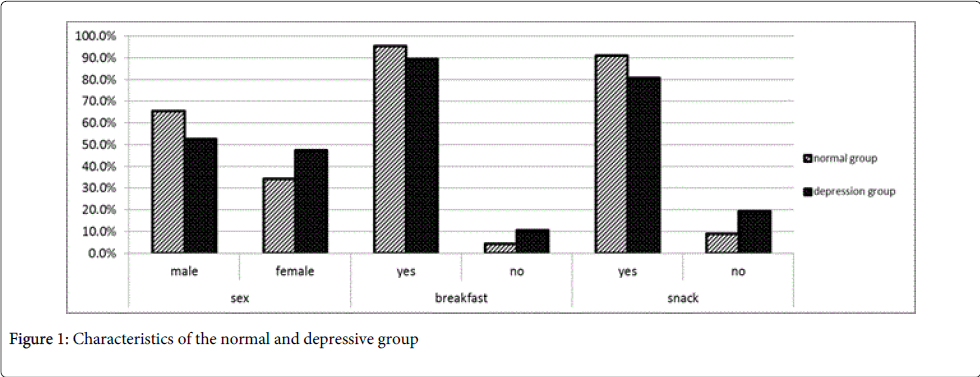
Figure 1: Characteristics of the normal and depressive group
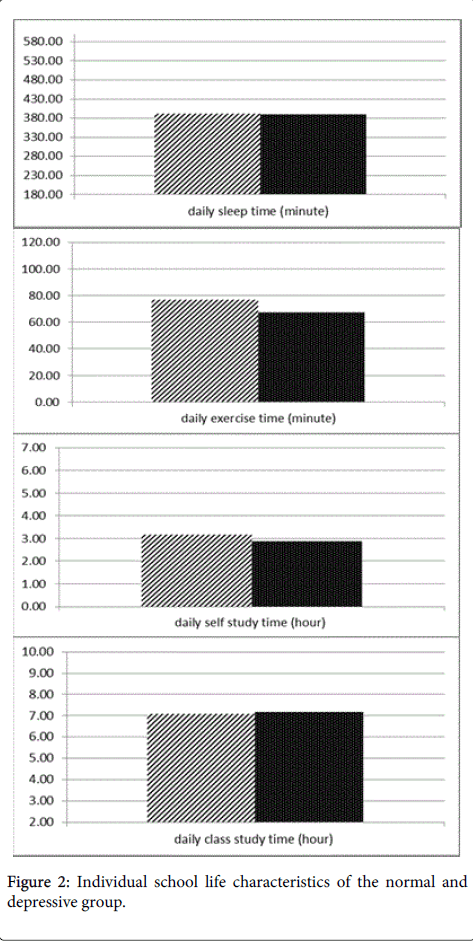
Figure 2: Individual school life characteristics of the normal and depressive group.
50 students (40.3%) were females. Male to female student in normal ZSDS range were 44 (65.7%)/23 (34.3%) and male to female student in depressive ZSDS range were 30 (52.6%)/27 (47.4%).
These results showed that female students had a more depressive tendency than male students. There was no significant difference of school life characteristics in the groups. The only minimal differences in the normal range group rather than the depressive group were more breakfast eating habits (95.5%/89.5%) and more daily exercise time (77.24 ± 51.69/67.37 ± 49.37).
Other students’ characteristics were similar with the normal to depressive group, respectively: daily sleep time (390.82 ± 63.06/389.65 ± 73.89 minute), daily class study time (7.08 ± 1.24/7.18 ± 1.02 hour) and daily self-study time (3.18 ± 1.53/2.98 ± 1.19 hour).
Tables 1 and 2 report the results for the prevalence of physical symptoms in both groups. There were no physical symptoms difference in the groups, except for more dyspepsia (47.4%), joint pain (36.8%), and back pain (59.6%) in the depressive group (p<0.05).
| Normal range; N (%) | Depression range; N(%) | P value | |
| Neurologic symptoms | |||
| Headache | 22 (32.8%) | 28 (49.1%) | >0.05 |
| dizziness | 16 (23.9%) | 21 (36.8%) | >0.05 |
| Tremor | 10 (14.9%) | 10 (17.5%) | >0.05 |
| Abnormal body sensation | 1 (1.5%) | 4 (7.0%) | >0.05 |
| Ophthalmic symptoms | |||
| Blurred vision | 15 (22.4%) | 20 (35.1%) | >0.05 |
| Eyeball pain | 11 (16.4%) | 16 (28.1%) | >0.05 |
| Decreased visual acuity | 22 (32.8%) | 24 (42.1%) | >0.05 |
| Eyeball strain | 33 (49.3%) | 36 (63.2%) | >0.05 |
| Auditory symptoms | |||
| Tinnitus | 21 (31.3%) | 25 (43.9%) | >0.05 |
| Decreased auditory function | 9 (13.4%) | 9 (15.8%) | >0.05 |
| Deafness | 4 (6.0%) | 9 (15.8%) | >0.05 |
Table 1: Prevalence of physical symptoms in head and neck.
| Normal range; N (%) | Depression range; N (%) | P value | |
| Cardio-pulmonary symptoms | |||
| Chest pain | 14 (20.9%) | 13 (22.8%) | >0.05 |
| Palpitation | 13 (19.4%) | 19 (33.3%) | >0.05 |
| Arrhythmia | 3 (4.5%) | 2 (3.5%) | >0.05 |
| Tachycardia | 3 (4.5%) | 4 (7.0%) | >0.05 |
| Edema | 7 (10.4%) | 3 (5.3%) | >0.05 |
| Common cold | 36 (53.7%) | 32 (56.1%) | >0.05 |
| Coughing | 35 (52.2%) | 33 (57.9%) | >0.05 |
| Sputum | 25 (37.3%) | 31 (54.4%) | >0.05 |
| Dyspnea | 8 (11.9%) | 3 (5.3%) | >0.05 |
| Hoarseness | 18 (26.9%) | 13 (23.2%) | >0.05 |
| Gastrointestinal symptoms | |||
| Epigastricpain | 13 (19.4%) | 12 (21.1%) | >0.05 |
| Dyspepsia | 19 (28.4%) | 27 (47.4%) | <0.05* |
| Difficulty swallowing | 4 (6.0%) | 4 (7.0%) | >0.05 |
| Nausea, vomiting | 12 (17.9%) | 18 (31.6%) | >0.05 |
| Diarrhea | 16 (23.9%) | 20 (35.1%) | >0.05 |
| Abdominal pain | 13 (19.4%) | 19 (33.3%) | >0.05 |
| Melena | 6 (9.0%) | 1 (1.8%) | >0.05 |
| Constipation | 12 (17.9%) | 16 (28.1%) | >0.05 |
| Frequent loose stool | 7 (10.4%) | 9 (15.8%) | >0.05 |
| Voiding and skin symptoms | |||
| Painful urination | 3 (4.5%) | 2 (3.5%) | >0.05 |
| Tenesmus | 5 (7.5%) | 3 (5.3%) | >0.05 |
| Frequent urination | 5 (7.5%) | 7 (12.3%) | >0.05 |
| diminished urine stream | 3 (4.5%) | 3 (5.3%) | >0.05 |
| itching sensation | 17 (25.4%) | 15 (26.3%) | >0.05 |
| skin eruption | 7 (10.4%) | 12 (21.1%) | >0.05 |
| Skeletal symptoms | |||
| joint pain | 12 (17.9%) | 21 (36.8%) | <0.05* |
| joint stiffness and motion limit | 3 (4.5%) | 8 (14.0%) | >0.05 |
| back pain | 27 (40.3%) | 34 (59.6%) | <0.05* |
Table 2: Prevalence of physical symptoms in body and extremity.
Table 3 presented the ZSDS score in both groups. The mean ZSDS score in the normal and depressive groups were 38.16 ± 4.60 and 51.11 ± 4.27, respectively. Mild depressed range ZSDS students were 44.7% and moderately depressed range ZSDS students were 1.6%.
| Normal group | Depressive group | |
| I feel down hearted and blue | 1.49 ± 0.63 | 2.23 ± 1.01 |
| Morning is when I feel the best | 3.27 ± 0.86 | 3.60 ± 0.65 |
| I have crying spells or feel like it | 1.13 ± 0.34 | 1.74 ± 0.79 |
| I have trouble sleeping at night | 1.42 ± 0.76 | 2.12 ± 0.96 |
| I eat as much as I used to | 2.36 ± 1.04 | 2.67 ± 1.00 |
| I still enjoy sex | 2.94 ± 1.14 | 3.40 ± 0.99 |
| I notice that I am losing weight | 1.48 ± 0.68 | 1.81 ± 0.95 |
| I have trouble with constipation | 1.37 ± 0.62 | 1.65 ± 0.95 |
| My heart beats faster than usual | 1.28 ± 0.62 | 1.63 ± 0.87 |
| I get tired for no reason | 1.84 ± 0.86 | 2.70 ± 1.05 |
| My mind is as clear as it used to be | 2.46 ± 0.99 | 3.37 ± 0.67 |
| I find it easy to do the things I used to | 2.33 ± 0.89 | 2.98 ± 0.89 |
| I am restless and can't keep still | 1.67 ± 0.63 | 1.98 ± 0.91 |
| I feel hopeful about the future | 2.01 ± 0.84 | 3.44 ± 0.65 |
| I am more irritable than usual | 1.66 ± 0.75 | 2.07 ± 0.99 |
| I find it easy to make decisions | 2.55 ± 0.82 | 3.21 ± 0.84 |
| I feel that I am useful and needed | 2.03 ± 0.73 | 3.16 ± 0.81 |
| My life is pretty full | 1.93 ± 0.70 | 3.11 ± 0.88 |
| I feel that others would be better off if I were dead | 1.22 ± 0.51 | 1.54 ± 0.65 |
| I still enjoy the things I used to do | 1.72 ± 0.69 | 2.70 ± 0.94 |
| Mean scale (sum) | 38.16 ± 4.60 | 51.11 ± 4.27 |
Table 3: Comparison of the Zung self-rating depression sale score in both group.
Figure 3 provides a four factor of the Zung Self-rating Depression Scale; core depressive factor (factor 1), cognitive factor (factor 2), anxiety factor (factor 3) and somatic factor (factor 4). There are 7 items which demonstrated a gap exceeding 50 percent in item scores between two groups. Additionally, six items were from factor 1 (items 1: depressed affect, items 3: crying spells, items 14: hopelessness, items 17: personal devaluation, items 18: emptiness, items 20: dissatisfaction). These results indicate that the major problem in the depressive group is a depressive mood. The last one is item 4 (sleep disturbance) of factor 3. This result is identified with the result of daily sleep time, the only category which showed a difference among school life characteristics in the two groups.
According to an investigation conducted by the Ministry of Health and Welfare in Korea in 2007, the depression rate (when is defined as depression influencing even daily life for more than two weeks in one year) of middle school students and high school students increased from 29.9% in 2005 to 41.3% in 2007 [12]. The studies about the increase in depression of Korean teenagers demonstrate that academic stress from studying, prospects, future, and school life based on an educational system that only focuses on college entrance exams is the main factor of depression besides developmental features during the adolescent period [13,14] According to a recent study, the academic stress level of Korean students was 50.5%, the highest among the 30 countries in the Organization for Economic Cooperation and Development (OECD). This is a rather high figure compared to the total average of 33.3% [15].
In Korea, in order to make a good college entrance result, high school students want to live in famous high school dormitories in order to study hard. However, because of the strict school life and the massive amounts of studying students do, they have huge physical and mental problems. Residency is a time when future work habits and self-care behaviorisms can be strongly influenced. However, most boarding schools are located far away from students’ homes. There may be various problems because students’ homes differ. These stressors can impact mental health, such as family disconnections, community dysfunctions, and social disadvantages [16]. Parents are usually the most meaningful source of social support in early life, and the perception of parental love and caring have important effects on biological and psychological health and illness throughout life [17]. In previous studies of psychological health of the resident and day students, full boarding students were more likely to experience obsessive-compulsive disorder, sensitivity in relationships, depression, anxiety, paranoia, and psychosis symptoms compared to day students [18]. Residency in dormitory school is a time when future work habits and self-care behaviors can be strongly influenced. If residents are provided opportunities to develop self-care practices to help cope with the stress of the future profession, it may mitigate more severe mental dysfunction and burnout later. Wellness health behaviors that buffer stress reactivity include physical activity, exercise, a nutritious diet, mind-body activities, prayer, seeking social support, getting restful sleep [19].
Depression is a seriously disabling health problem with a life time prevalence of 16% and with a female to male ratio of about 5:2 [20]. Studies suggest gender differences in residents’ experience of distress; female residents have higher levels of anxiety and depression while males experience higher levels of depersonalization [21,22]. The tendency of females to report more depressive symptoms than males might be responsible for their greater likelihood of meeting criteria for a depressive disorder, even though males and females with depressed mood reports similar levels of subjective, social and occupational impairment. Several studies have shown that a female preponderance in rates of depression occurs at low symptom thresholds and becomes more pronounced as the number of symptoms increase [23]. According to the findings in our study, female students in the depression ZSDS range were a more prevalent ratio (47.4%) than the normal range (34.3%). Typical depressive symptoms include depressed mood, decreased interest, diminished pleasure, feeling of worthlessness, inappropriate guilt, decrease appetite and libido, and insomnia [24]. Moreover, clinical manifestations of depression differ by gender, with females more often reporting disturbances of appetite and sleep, fatigue, somatic anxiety and hypochondriasis [25]. Menstruation disorders are especially more prevalent in early puberty among girls. These severe menstruation disorder signs affect quality of life [26]. Throughout adolescence, these disorders increase with a steep slope and are more prevalent among girls who are more vulnerable to various psychosocial factors, so the ration of girls’ involvement in these disorders compared to boys is 1.3:1 [27].
Depressive symptoms have been grouped into psychological and somatic or into affective, somatic and cognitive symptoms [5,28] In the primary care setting, approximately two thirds of patients with depression report somatic symptoms solely as the reason for consultation [5]. Depression is mostly difficult to recognize in such patients, being the major reason for under-diagnosis and under-treatment of depression [11]. Traditionally, the heterogenous symptoms of depression have been grouped into different symptomatic dimensions according to their clinical significance but there is no consensus on how this is best done. We decided to evaluate the status and degree of depression among boarding students by using a ZSDS questionnaire and factor analysis of the ZSDS. The ZSDS has been used as a prevalent method to evaluate depression disorders among different nationalities. Tens items are worded positively and the the other 10 are worded negatively. The four factors were divided into core depressive factor (factor 1), cognitive factor (factor 2), anxiety factor (factor 3) and somatic factor (factor 4), according to the nature of the symptoms [11]. Core depressive factor (factor 1) appears to primarily reflect emotional or affective symptoms of depression. Cognitive factor (factor 2) appears to reflect symptoms related to difficulty in concentration, decision making, confusion or loss of mental clarity, and psychomotor retardation. Anxiety factor (factor 3) appears to reflect symptoms related to irritability, psychomotor agitation, restlessness, and sleep disturbance. Somatic factor (factor 4) includes 3 ZSDS items: items 5 (decreased appetite), items 7 (weight loss), and items 9 (tachycardia). Remnant 2 ZSDS items were not classified: items 2 (diurnal variation), items 8 (constipation). In our study, there are 7 items which showed a gap exceeding 50 percent of item score between two groups. Since 6 items were from factor 1 representing depressed mood, it was indicated that emotional and affective disorder were the most evident issues in the depressive group.
The study was commenced to investigate the physical and mental status of senior high school students who are endeavoring to resolve the uncertainty of their future, and was designed to understand the changes of psychological status among boarding students who are facing university entrance and trying to achieve their dream but cannot gain support from their home environment. Unlike other general high schools in Korea, which only focus on students’ academic performance, KIS emphasizes various extracurricular activities (sports, art, field trips, etc.), as well as academic achievement. This tendency would probably affect the students and in fact there was no significant difference between the normal and depressive groups in terms of physical symptoms. However, emotional stress can be a great burden for adolescents living in a dormitory who should manage their lives by themselves. This study also showed that mood disturbance was clearly more intense while the cognitive functions related to academic performance were proven not problematic in the depressive group. In the adolescent period, neglected depressive mood can be converted to major depressive disorder. Major depressive disorder not only produces decrement in health that are equivalent to those of other chronic disease, but also worsens mean health scores substantially more when comorbid with these diseases. To solve this problem, it seemed that difficulty in talking to parents, teachers and issues arising from peer relations should first be managed. For this, good social support from school administrative officers, teachers, parents, and classmates may help individuals and provide relief to distressed students, nourishing them to maintain sound mentality. To deal with specific issues among boarding students, a comparison study between boarding and day students would be helpful in the future.