Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2015) Volume 3, Issue 1
Selective Serotonin Reuptake Inhibitors (SSRI) are prescribed to treat anxiety and depression disorders by altering levels of the neurotransmitter serotonin. Research has demonstrated that these medications negatively impact bone health in adults over the age of 30 years by affecting the activity of osteoblasts, yet the effects have not been studied in college-aged adults. The purpose of this preliminary study was to describe the relationship between SSRIs and bone health and muscle function in college-aged students. Nine SSRI users were matched with nine non-users for physical activity level, nutritional intake, sex, race and body mass index and split into four groups: high active SSRI users, low active SSRI users, high active controls and low active controls. Dual Energy X-Ray Absorptiometry (DXA) scans were taken of the total body, proximal femur and anterior-posterior (AP) spine to assess bone health and a series of muscle tests were used to asses muscle strength, power and endurance. Muscle power, measured via vertical leap height, was significantly higher in both high- and low-active controls than SSRI-users. Low active SSRI-users showed significantly lower total leg bone mineral density and femoral neck and total femur bone mineral content than low active controls. These preliminary results suggest that SSRI use may reduce the ability to produce maximal muscle power by altering the effects of serotonin on action potential conductance. Additionally, SSRIs may have a negative effect on bone health in a college aged population, but these negative effects may be overcome through adequate levels of physical activity.
<Keywords: Selective Serotonin Reuptake Inhibitors (SSRIs); Serotonin (5-HT); Bone Mineral Density (BMD); Bone Mineral Content (BMC); Dual Energy X-Ray Absorptiometry (DXA)
The base-rate of lifetime mental health problems in the US is over 40% and mood and anxiety disorders account for the majority of cases [1]. Among the most concerning trends related to depression rates is the increase in depressive symptoms in adolescent females over the age of 15 years at which time the prevalence of depression doubles that of adolescent males [2]. Researchers have reported that up to 25% of adolescent females show signs of depression beginning in grades 6-10, making this disorder the biggest contributor to morbidity and mortality among psychiatric disorders [3]. Relatedly, in the past two decades there has been an increase in the prescription of medicines that treat these disorders, specifically in adolescents [4]. Selective Serotonin Reuptake Inhibitors (SSRIs) are the most common and first choice medications prescribed to treat depression and anxiety in children and adolescents [5]. This medication is an antagonist that works by blocking the reuptake of serotonin by its receptors, thereby increasing levels of circulating serotonin [6]. In the brain, increasing levels of circulating serotonin is thought to help improve mood regulation; however, as serotonin (5-HT) is a widely used neurotransmitter in several physiological pathways, it has consequences beyond emotion alteration. For example, previous work has demonstrated that SSRI use interferes with the 5-HT receptors in bone, therefore impacting bone health [7-9].
Furthermore, researchers have suggested that both depressive symptoms and SSRI use contribute to a decrease in Bone Mineral Density (BMD): psychological effects of depression and anxiety indirectly impact bone by negatively altering physical activity and nutrition habits [10], while SSRI medications have been shown to directly impact bone health by inhibiting osteoblast activity [11]. Studies have demonstrated a decrease in BMD at several sites in both men and women with a history of SSRI use over the age of 30 years [12-14]. SSRIs have also been shown to impact the risk of falls and fractures that occur as a side effect of decreased BMD, with studies showing an 11% increase in the amount of falls suffered by adults over 65 years with a history of taking an SSRI in comparison to adults without reported use of this medication [15]. While these studies demonstrate the relationship between SSRI use and BMD in adults over 30 years old, there is a dearth of information on the effects in a younger population. Whereas the amount of antidepressant medications prescribed increased from 5.1 per 1000 population in 1989 to 15.4 per 1000 in 2007, with females receiving the majority of prescriptions and SSRIs being the most widely used antidepressant medication, there is a need for more research involving this medication and age group [16].
As bone provides structure, mechanical basis for movement, mineral storage and organ protection for the human body, its health is a critical aspect of overall health. Peak bone mineral density is attained in females between the ages of 18-20 years and in males between the ages of 20-22 years [17]. Therefore, achieving optimal bone health requires maximizing bone formation before this critical phase and minimizing bone resorption after it. Bone undergoes a continuous cycle of formation and resorption every 4-6 months, with formation overpowering absorption until peak BMD is reached [18]. Therefore, it has been suggested that if bone formation is inhibited in any way during childhood and adolescents, peak BMD may be negatively impacted, leaving the bone more susceptible to lower BMD and injury later in adulthood [19]. Given that there is evidence that SSRI medications inhibit bone formation, it may be that taking this medication before peak bone mineral density is reached may have a negative impact effect of decreasing BMD throughout adulthood [11].
Muscle health must also be examined to get a complete picture of the bone-muscle unit due to the relationship between muscle strain and BMD [20]. The mechano stat theory suggests that there is a doseresponse relationship between the level of stress placed on bone by muscular contraction and bone mass, content and geometry [21]. As more stress is placed on the bone via muscle contractions generated during physical activity, bone mineral density is positively influenced via increased osteoblast activity, suggesting that it is not only the frequency but also the intensity of physical activity that contributes to enhanced bone mineral density [20].
The purpose of this preliminary study was to examine the relationship between SSRI medication use with bone and muscle health in college students between the ages of 18 and 22 years. Specifically, bone health will be assessed by BMD and Bone Mineral Content (BMC) measurements and muscle health will be measured isokinetic strength, muscle power, muscle endurance and balance.
Upon receiving Institutional Review Board approval, participants were recruited from a college student body during the Spring 2013 semester via the Introduction to Psychology subject pool, all-college emails and campus-wide flyers. Nine participants taking SSRI medications (SSRI, 5 females, 4 males) were matched to nine controls (CON, 5 females, 4 males). The SSRI group consisted of participants who self-reported taking the medication for at least six consecutive months within the past two years to assure adequate effect of the medication on bone turnover. The CON group consisted of participants with no history of SSRI use matched according to sex, age, race, smoking status, BMI range and physical activity. BMI range was broken into underweight (<18 kg/m2), normal weight (18-24.9 kg/m2), over weight (25-29.9 kg/m2) or obese (>30 kg/m2) [22] and physical activity was categorized as athlete, recreationally active or non-active. Exclusion criteria included females with a history of amenorrhea lasting longer than three months or a chance of a current pregnancy. Participation in this study was voluntary and each participant was given copies of their personal data to keep at the conclusion of the study.
At the first testing session, participants reported to the Skidmore College Human Performance Laboratory to be consented. Participants in the SSRI group were recruited first so that the parameters for finding matched controls could be assessed. BMI classification of underweight, normal weight, overweight or obese was determined by height and weight measurements. Medication use, past skeletal injuries and menstrual history were recorded on a medical history questionnaire. Lifetime physical activity levels were assessed using the Bone-Loading History Questionnaire, which has been previously found to be reliable and valid [23]. More specific bone-loading physical activity levels were determined using the Bone-Specific Physical Activity Questionnaire, using a reliable algorithm to predict a bone loading score based on activity levels throughout life [24]. Nutritional intake habits, specifically calcium and vitamin K consumption were analyzed via dietary food logs, for which each participant was given instructions on how to record all food and beverage intake on two week days and one weekend day. A conversion chart was provided to assist in determining portion size (Nutritionist 4 software).Based on BMI category, physical activity questionnaire scores, sex and race matched controls were chosen for each participant in the SSRI group. A pool of healthy volunteers was screened and individuals were selected if they met the necessary parameters. Each selected participant in the CON group then came to a first testing session and completed the same questionnaires as the SSRI group to verify adequate matches.
Participants returned to the laboratory for a second test day within the same month in which a series of bone scans and physical tests were conducted to assess bone health and muscle function.
BMD and BMC were measured using Dual Energy X-Ray Absorptiometry (DXA) technology (DXA; GE/Lunar, iDXA, software version 13.40.038). Mineralized bone tissue per area scan (g/cm2) was measured at the Left Proximal Femur, Anterior-Posterior (AP) Lumbar Spine and total body. The former two scans were run at Hi-Res medium resolution at a current of 3000 μA, while the latter was run at Hi-Res medium resolution at a current of 150 μA. Laboratory precision for all scans is less than 1%.
Muscle function tests included an isokinetic assessment of quadriceps and hamstring strength, quadriceps endurance, quadriceps muscle power and the star excursion balance test. The large muscle groups of the hamstring and quadriceps were used to offer a more direct comparison between the lower trunk bone scans and lower body muscle groups. Furthermore, as there is a dose response relationship between muscle force generation and bone health, the large muscle groups were most likely to illustrate the potential effects described by the mechanostat theory [21]. Prior to muscle testing, participants performed a 5 minute warm up on a cycle ergometer (Monarch) at 50 rpm. The muscle tests were done in the same sequential order for each participant to control for potential muscle fatigue after each test.
Isokinetic strength of the quadriceps and hamstrings was assessed through a concentric test of flexion and extension strength using an isokinetic protocol(Cybex, HUMAC NORM 2004 V 4.2.8). Two tests were performed on each leg: 60°of motion per second for 5 slow repetitions against a heavy load and 180° of motion per second for 10 fast repetition against a lighter load. Participants were positioned on the machine according to the manufacturer’s User’s Guide and were verbally motivated by the researchers to use maximal force during each test.
Quadriceps endurance was measured by a timed wall sit in which participants placed their back against a wall with feet shoulder width apart and flat on the floor and hips and knees flexed to 90°. One foot was lifted and held approximately 5 cm off the floor until the participant felt maximum fatigue and voluntarily put the foot down. The same procedure was conducted on the opposing leg. Total time on each leg was recorded and added for a total score, which was compared to normative data to determine endurance levels [25].
Quadriceps muscle power was assessed using a vertical leap test (Vertec 22550 device). The maximum standing height was recorded as that reached with the participant standing on two feet directly under the device with both arms extended up. The participant jumped off two feet from a standing position and touched the highest rung possible, which was recorded as jump height. Three separate consecutive trials were conducted and the highest height achieved was recorded as maximal jump height. The difference between the standing height and jump height was recorded as vertical leap height.
Dynamic balance was assessed using the Star Excursion Balance Test which has repeatedly been shown to predict both lower extremity control and lower extremity injury in patients with balance deficits [26,27]. The protocol of Plisky et al. was followed to conduct this test [27], although participants only performed movement in the posterior medial direction (45°angle backwards on the same side of the body), as previous research has determined this as most representative in evaluating balance [26].
Descriptive data were reported as mean ± standard deviation unless otherwise noted. Due to low enrollment in the study, without adequate power, we present the data as preliminary data. To compare BMD, BMC and muscle function between SSRI and CON groups, unpaired t-tests were used. The groups were split into high and low physical activity groups based on a median split of past Bone Loading History Questionnaire scores for further data analysis. The median value of all 18 participants for past questionnaire scores was determined and participants with scores above that value were considered high active while participants with scores below this value were considered low active. Subsequent t-testswere carried out based on this split. Significance was set at p < 0.05.
Descriptive statistics show a successful matching of SSRI and CON group participants, as there were no significant differences between the groups in any characteristics (Table 1). Both groups had the same number of males (n=4), females (n=5), Asians (n=1) and Caucasians (n=8).
| Variable | SSRI N=9 | CON N=9 |
|---|---|---|
| Age (yrs) | 20.56 ± 1.33 | 20.89 ± 0.928 |
| Height (m) | 1.69 ± 0.075 | 1.72 ± 0.149 |
| Weight (kg) | 68.07 ± 13.09 | 66.36 ± 11.68 |
| BMI (kg/m2) | 23.73 ± 4.04 | 22.47 ± 3.12 |
| Body fat (%) | 25.84 ± 4.99 | 23.07 ± 6.57 |
| Ca (%DV) | 126.85 ± 63.65 | 78.92 ± 38.37 |
| Vitamin K (%DV) | 82.29 ± 133.92 | 55.59 ± 38.61 |
| Vitamin D (%DV) | 10.35 ± 12.49 | 16.24 ± 11.11 |
| BLHQ past | 57.29 ± 26.12 | 77.43 ± 42.41 |
| BLHQ present | 48.30 ± 15.79 | 57.55 ± 42.07 |
| BPAQ past | 79.85 ± 25.71 | 62.68 ± 34.09 |
| BPAQ present | 28.63 ± 25.71 | 29.08 ± 18.68 |
All values reports as ± standard deviation. %DV= percentage of recommended daily value, BLHQ= bone loading history questionnaire, BPAQ= bone-specific physical activity questionnaire. No units given to BLHQ or BPAQ score.
Table 1: Descriptive characteristics of SSRI and CON group
Two members of the CON group reported half-Asian or Hispanic ethnicities, but as the participant pool was limited and all other criteria were well matched, these two participants were matched to Caucasian SSRI participants.
Bone measurement and muscle function test results for each group are reported in Table 2 and Table 3, respectively. A significant difference was found in vertical leap height, with the CON group jumping significantly higher than the SSRI group (p=0.014). No other significant differences were seen in any other measure of bone health or muscle function between groups. However, average BMD was consistently lower in the SSRI group than the CON group at each measured site, specifically at the total femur, femoral neck and AP spine (8.8%, 6.8%, 2.3%, respectively).
| Test | SSRI N=9 | CON N=9 | p-value |
|---|---|---|---|
| Left leg cybex (ftlbs) | 135.63 ± 46.02 | 153.00 ± 60.68 | P=0.529 |
| Right leg cybex (ftlbs) | 136.00 ± 54.23 | 127.89 ± 52.49 | P=0.759 |
| Vertical leap (cm) | 43.44 ± 15.93 | 79.44 ± 36.00 | P=0.014 |
| Wall sit (s) | 116.38 ± 39.64 | 136.11 ± 50.90 | P=0.372 |
| Balance (cm) | 99.50 ± 17.07 | 96.88 ± 15.56 | P=0.738 |
All values reported as mean ± standard deviation.
Table 2: Comparison of muscle function tests between SSRI and CON groups.
| Bone | BMD (g/cm2) | BMC (g) | Area (cm2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| SSRI | CON | p | SSRI | CON | p | SSRI | CON | p | |
| Total body | 1.24 ± 0.14 | 1.29 ± 0.16 | .528 | 2689.11 ± 541.19 | 2801.56 ± 676.39 | .702 | -- | -- | -- |
| Total leg | 1.27 ± 0.16 | 1.34 ± 0.20 | .417 | 994.89 ± 227.93 | 1059.89 ± 307.02 | .617 | -- | -- | -- |
| Femoral Neck | 1.09 ± 0.14 | 1.17 ± 0.22 | .381 | 5.37 ± 1.04 | 5.78 ± 1.60 | .528 | 4.91 ± 0.57 | 4.91 ± 0.64 | .997 |
| Wards Triangle | 0.98 ± 0.21 | 1.09 ± 0.23 | .252 | 2.66 ± 0.92 | 3.04 ± 1.28 | .481 | 2.71 ± 0.61 | 2.72 ± 0.70 | .983 |
| Total Femur | 1.08 ± 0.17 | 1.19 ± 0.21 | .255 | 34.94 ± 7.06 | 38.38 ± 11.21 | .448 | 32.29 ± 3.52 | 32.11 ± 5.38 | .937 |
| AP spine | 1.28 ± 0.15 | 1.31 ± 0.17 | .679 | 56.50 ± 5.98 | 57.12 ± 14.19 | .905 | 44.33 ± 3.95 | 43.19 ± 6.73 | .669 |
All values reported as mean ± standard deviation.
Table 3: Comparison of bone health values between SSRI and CON groups.
Additional analyses examining the specific role that physical activity plays in the relationship between SSRI use and the bone and muscle variables were conducted after performing the median split of bone loading history questionnaire scores. This split yielded a median score of 58.6, classifying 10 participants as high active (5 SSRI, 5 CON) and 8 participants as low active (4 SSRI, 4 CON, Figure 1). Descriptive statistics were compared between the groups based on this split. As shown in Table 4, high active participants in the SSRI group consumed a significantly different percentage of recommended daily calcium thanhigh active control group participants (p=0.034). No other significant differences were seen either within each activity group or between the high and low active groups. Tables 5 and 6 report the bone measurement and muscle function test results, respectively, of each group based on the split. Significant differences were seen in total leg BMD, femoral neck BMC, total femur BMC and left leg peak torque between the low active SSRI and low active control groups, with the SSRI group having lower bone mineral and torque values than their controls (p=0.019, 0.047, 0.012, 0.038, respectively). No differences were seen between high active SSRI and high active CON groups or between the total high active and low active groups in regards to bone or muscle variables.
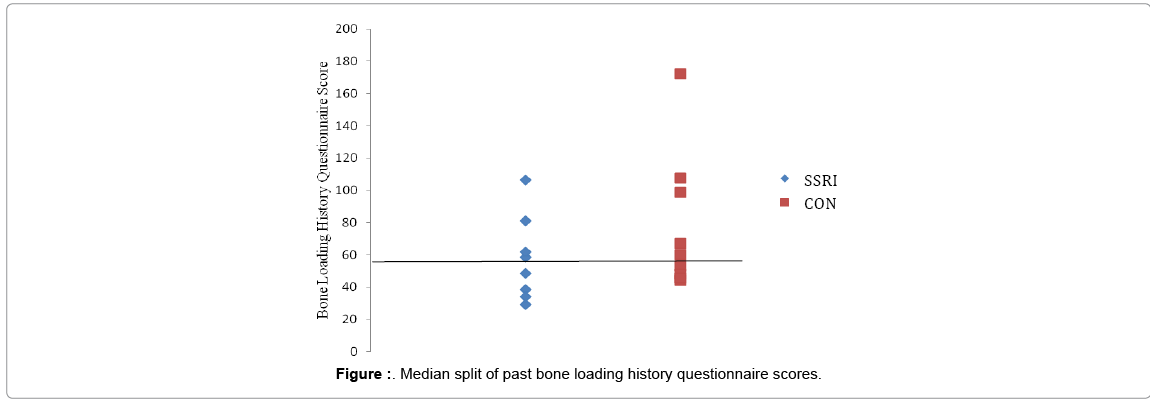
Figure 1: Median split of past bone loading history questionnaire scores.
| Variable | High | Low | ||||
|---|---|---|---|---|---|---|
| SSRI n=5 | CON n=5 | p | SSRI n=4 | CON n=4 | p | |
| Age (yrs) | 20.75 ± 0.50 | 21.00 ± 0.00 | 0.356 | 20.00 ± 1.83 | 20.50 ± 1.29 | 0.670 |
| Height (m) | 1.72 ± 3.97 | 1.66 ± 10.17 | 0.298 | 1.66 ± 10.28 | 1.77 ± 19.88 | 0.374 |
| Weight (kg) | 71.38 ± 4.17 | 62.90 ± 11.62 | 0.219 | 57.63 ± 2.53 | 64.63 ± 8.00 | 0.146 |
| BMI (kg/m2) | 24.11 ± 1.53 | 22.73 ± 2.21 | 0.346 | 21.12 ± 2.28 | 21.03 ± 3.27 | 0.967 |
| Body fat (%) | 25.53 ± 5.75 | 24.40 ± 7.11 | 0.814 | 25.85 ± 5.73 | 21.98 ± 7.76 | 0.452 |
| Ca (%DV) | 139.12 ± 48.29 | 60.46 ± 31.22 | 0.034* | 111.07 ± 72.84 | 71.30 ± 52.09 | 0.409 |
| Vitamin K (%DV) | 27.75 ± 11.37 | 122.07 ± 161.72 | 0.289 | 117.54 ± 179.17 | 45.91 ± 49.69 | 0.470 |
| Vitamin D (%DV) | 15.17 ± 14.52 | 15.06 ± 16.62 | 0.993 | 5.47 ± 6.20 | 6.32 ± 6.83 | 0.861 |
| BLHQ past | 77.04 ± 22.01 | 99.59 ± 51.42 | 0.451 | 37.56 ± 8.27 | 47.72 ± 3.96 | 0.969 |
| BLHQ present | 55.29 ± 14.15 | 66.42 ± 60.67 | 0.733 | 41.32 ± 15.86 | 41.83 ± 18.79 | 0.398 |
All values reports as ± standard deviation. %DV= percentage of recommended daily value, BLHQ= bone loading history questionnaire. No units given to BLHQ score. *p<0.05.
Table 4: Characteristics of SSRI and CON groups according to past physical activity level (high and low).
| High | Low | |||||
|---|---|---|---|---|---|---|
| SSRI n=5 | CON n=5 | p | SSRI n=4 | CON n=4 | p | |
| Total body | ||||||
| BMD | 1.32 ± 0.16 | 1.35 ± 0.21 | 0.801 | 1.13 ± 0.04 | 1.22 ± 0.05 | 0.055 |
| BMC | 2943.00 ± 530.72 | 2953.00 ± 859.55 | 0.984 | 2268.75 ± 173.29 | 2612.25 ± 385.88 | 0.155 |
| Total leg | ||||||
| BMD | 1.37 ± 0.17 | 1.43 ± 0.25 | 0.721 | 1.15 ± 0.02 | 1.25 ± 0.06 | 0.019* |
| BMC | 1114.25 ± 234.42 | 1136.40 ± 378.29 | 0.922 | 824.00 ± 107.22 | 964.25 ± 196.47 | 0.257 |
| Femoral neck | ||||||
| BMD | 1.18 ± 0.17 | 1.26 ± 0.25 | 0.601 | 1.01 ± 0.08 | 1.06 ± 0.09 | 0.540 |
| BMC | 6.02 ± 1.04 | 6.31 ± 2.07 | 0.804 | 4.53 ± 0.36 | 5.11 ± 0.29 | 0.047* |
| Area | 5.11 ± 0.41 | 4.93 ± 0.67 | ||||
| Wards triangle | ||||||
| BMD | 1.12 ± 0.26 | 1.21 ± 0.25 | 0.599 | 0.86 ± 0.09 | 0.96 ± 0.10 | 0.180 |
| BMC | 3.26 ± 0.97 | 3.44 ± 1.62 | 0.847 | 1.94 ± 0.26 | 2.54 ± 0.49 | 0.077 |
| Area | 2.92 ± 0.48 | 2.74 ± 0.74 | 0.694 | 2.29 ± 0.47 | 2.69 ± 0.76 | 0.401 |
| Total femur | ||||||
| BMD | 1.17 ± 0.19 | 1.28 ± 0.23 | 0.479 | 0.99 ± 0.13 | 1.07 ± 0.12 | 0.370 |
| BMC | 38.67 ± 0.19 | 41.68 ± 14.71 | 0.725 | 29.59 ± 0.96 | 34.25 ± 2.43 | 0.012* |
| AP spine | ||||||
| BMD | 1.36 ± 0.19 | 1.36 ± 0.19 | 0.999 | 1.21 ± 0.07 | 1.25 ± 0.06 | 0.419 |
| BMC | 57.75 ± 7.62 | 60.03 ± 19.24 | 0.831 | 53.67 ± 3.31 | 53.49 ± 3.40 | 0.942 |
Values reported as mean ± standard deviation. *p<0.05
Table 5: Bone health values for SSRI and CON groups according to past physical activity level (high and low)
| High | Low | |||||
|---|---|---|---|---|---|---|
| SSRI n=5 | CON n=5 | p | SSRI n=4 | CON n=4 | p | |
| L leg cybex (ftlbs) | 176.25 ± 19.91 | 166.50 ± 84.39 | 0.830 | 95.00 ± 11.97 | 139.50 ± 95.00 | 0.038* |
| R leg cybex (ftlbs) | 177.50 ± 39.95 | 131.60 ± 69.90 | 0.279 | 94.50 ± 25.94 | 123.35 ± 30.76 | 0.203 |
| Vertical leap (cm) | 41.21 ± 9.99 | 81.79 ± 40.77 | 0.096 | 46.36 ± 23.58 | 76.50 ± 34.92 | 0.202 |
| Wall sit (s) | 144.25 ± 39.18 | 150.20 ± 36.92 | 0.822 | 85.35 ± 16.82 | 118.50 ± 65.94 | 0.368 |
| Balance (cm) | 0.57 ± 0.06 | 0.57 ± 0.09 | 0.983 | 0.59 ± 0.12 | 0.56 ± 0.06 | 0.675 |
Values reported as mean ± standard deviation. *p<0.05
Table 6: Muscle function values for SSRI and CON groups according to past physical activity level (high and low).
The purpose of this preliminary study was to investigate the relationship between SSRI antidepressant medication and bone and muscle health in a college aged population. The only difference in muscle function that was seen was in the quadriceps power muscle test, which showed that the CON group jumped significantly higher than the SSRI group. As this test assessed muscle power, it is likely that SSRI use may affect the production of muscle power without impacting strength or endurance. No significant differences were found between the SSRI and CON groups in BMD; however, when the groups were split according to activity level, DXA scan results showed significant differences in BMD of the total leg and BMC at the femoral neck and total femur.
The production of power or producing strength over time is highly dependent on the activation of neurons in the Central Nervous System (CNS). Muscle power is produced when neuronal cell bodies in the brain stem release monoamines to supercharge motoneurons to carry an action potential from the motor cortex to the skeletal muscle. Power production can be increased by either increasing the frequency of the action potentials or by increasing the amount of motoneurons recruited to perform the movement. Studies have shown that motoneurons are activated by 5-HT2 and aplha1 receptors, with a very high density of 5-HT in the spinal cord and spinal motoneurons [28]. Furthermore, 5-HT activity has been shown to increase just before a muscle contraction, with a positive linear relationship between the extent of this increase and the magnitude of the movement [6]. The presence of 5-HT allows for a plateau potential to be reached by enhancing excitatory persistent inward currents and reducing the outward current [29]. Previous research has shown that the presence of 5-HT receptor antagonists inhibited these currents and produced a more prolonged and less effective release of sodium, contributing to a loss of ability for motoneurons to fire. However, because the antidromic stimulation was not impaired, it is likely that the activation of the current was not the limiting factor in the motoneuron firing, rather it was the reduced effectiveness of the current on the motoneurons [28]. As such, it is possible that the use of SSRIs blocks 5-HT from binding to the necessary receptors to elicit an effective current and subsequent action potential. As an antidepressant medication, the inhibition of 5-HT reuptake allows for increased circulating 5-HT levels in the brain, which is believed to improve mood. However the results of this study suggest that SSRI medication may also block 5-HT receptors downstream and, through the mechanisms described above, reduce the speed of motoneuron firing enough to inhibit muscle power production.
It is important to note that the average jump height increased with each subsequent trial, alluding to the learning curve that takes place in this muscle function test. In future research, muscle power assessed by a Wingate cycle test might be preferred by reducing the possible learning curve effects seen with the vertical leap test. Furthermore, assessing muscle power using a Wingate test would allow for further investigation as to whether peak strength or peak velocity is the limiting factor in power production in people taking SSRIs.
BMD was 6.8%, 8.8% and 2.3% lower in SSRI users at the femoral neck, total femur and AP spine when compared to the matched controls, however these differences were non-significant. Although lacking the statistical power, these results are consistent with previous research, which has demonstrated that SSRIs alter the formation and function on osteoclasts and osteoblasts by reducing cell viability and inducing apoptosis [11]. Furthermore, mice studies have determined that altering levels of circulating 5-HT decreases bone formation. Specifically, high levels of circulating 5-HT are associated with decreased osteoblast activity due to its interactions with Tryptophan hydroxylase (Tph) and the Lpr5 gene. Lrp5 is responsible for regulating bone formation and inhibition of its activity has been associated with a reduction in BMD [20]. The expression of Lpr5 is inversely related to Tph, the rate limiting enzyme in the production of 5-HT in the gut and brain. As such, alterations in circulating 5-HT correspond with an increase in Tph activity, leading to a decrease in circulating Lpr5 activity and therefore a decrease in BMD [30]. Other research has supported this relationship by showing mice with a Lpr5 loss-of-function mutation to have low osteoblast activity and low bone mass. Wild type mice, which showed normal levels of 5-HT related to normal Tph levels, did not exhibit the effects of decreased Lpr5 activity and its consequent effects on bone mass. Although this model speaks directly to the production of serotonin, its implications can be applied to the effects of SSRI use. It is likely that SSRI use increases circulating levels of Tph in conjunction with circulating levels of 5-HT, thereby altering the Lpr5 gene function. In addition to the small effect size seen with the small sample used in this study, it is possible that the lack of statistical significance in our results was a result of SSRI dosage. Because not all members of the SSRI group reported current dosage of their medication, this variable was not considered. Future studies should look for a relationship between SSRI dosage and exact duration of use and bone mineral density, as it is possible many years of exposure are needed for the negative consequences to be significant.
We performed a close analysis of the bone-muscle relationship by splitting the groups based on activity level, with high active participants scoring above 58.6 on the past Bone Loading History Questionnaire and low active participants scoring below this value.When examining the differences between high and low active groups, the high-active CON group consumed significantly more calcium than the high-active SSRI group. However, the lack of physiological differences between these groups when calcium intake was accounted for suggests that this result did not affect bone or muscle health. Dietary values were obtained from self-reported food logs andhigh standard deviations contributed to the significant difference. As such, further investigation on the relationship between calcium intake, activity level and bone health is needed for conclusions to be drawn.
The physical activity division showed that the low-active SSRI group had significantly reduced BMD and BMC at three sites compared to the low-active CON group, including total leg BMD (8.7%), femoral neck BMC (11.3%) and total femur BMC (13.6%). However, there were no differences in BMD or BMC at any site between the high-active SSRI and high-active CON groups. These results suggest that SSRI use may negatively impact bone turnover and therefore bone health, but that this impact may be mitigated by physical activity. Previous research has shown that weight bearing physical activity increases BMD through positively influencing bone architecture, size and composition [31]. Researchers have shown that placing mechanical stress on rabbit bone leads to an enhancement in osteoblast activity and an inhibition of osteoclast activity, causing bone formation to outweigh resorption [32]. In humans, using weight bearing physical activity to place an adequate level of stress on bone increases BMD in a similar way. It is therefore likely that the positive effects of bone turnover induced by exercise outweigh the inhibition of bone formation caused by SSRI use, suggesting that physical activity may be particularly relevant to patients on this medication.
Previous research has also reported direct associations between 5-HT levels and physical activity. Altering 5-HT activity via inhibiting the 5-HT transporter or through SSRI treatment led to a reduction in cage activity in mice [33]. Knocking out the 5-HT transporter led to a reduction in bone mineral accrual of weight-bearing and cranial bones. Because the cranial bones were also affected, the reduction in bone mineral accrual was more likely caused by the lack of transporter activity rather than the reduced mechano sensitivity from the decrease in cage activity. On the other hand, mice treated with SSRIs only showed a reduction in bone accrual in the weight bearing bones, not the cranial bones. This suggests that the use of SSRIs does not induce a decrease in bone mineral accrual alone, rather through a combination of altered 5-HT levels and reduced mechano sensitivity [33]. This may suggest that it is not only the SSRI use that negatively impacts bone, but also the depression related decreases in physical activity. This point is particularly relevant when considering the lack of BMD and BMC differences seen between the high-active SSRI and CON groups.
The apparent interaction between physical activity levels and SSRIs on bone health and muscle function comes with important implications. Research has shown a bidirectional relationship between depression and physical activity in teenagers. Jerstad et al. reported that young females who showed symptoms of depression were 35% less likely to be physically active and that those who were physically active were 16% less likely to develop major depression [34]. This association was thought to be due to the increase in serum 5-HTlevels seen with physical activity. Not only can this increase in physical activity potentially improve depressive symptoms [34], it also appears to suppress negative effects that this medication may have on bone.
The results of this study were limited by the sample size. The confidential nature of mental health and medication use made recruitment difficult on a college campus, leading to a smallsample size. Although there were no significant differences in the descriptive statistics between SSRI and CON groups, high within group variability may have contributed to a lack of significant results. Further research on the relationship between SSRI use and bone health and muscle function should include a larger sample size to allow for greater sensitivity and specific results to be seen. Furthermore, it is important to note that the control group did not report any history of depressive symptoms. Depression has been shown to lead to lack of movement and physical activity [34] and although the control group showed higher BLHQ scores in this study, this difference was not significant. As such, this study cannot conclude whether the relationship between the variables in question was due directly to SSRI use or was an effect of reduced physical activity as a side effect of depression in the SSRI group.
In summary, this pilot study suggests that SSRI medication use in college age individuals may negatively impact the production of muscle power, but is only associated with bone health in a historically inactive population. This suggests that regular physical activity throughout childhood and adolescence may protect against potential negative effects of SSRIs on bone, though future prospective longitudinal research is needed. Further, future studies may involve exercise interventions on participants as they first begin SSRI medication use to more specifically quantify these effects in a young population.
A special thank you to Dr. Casey Schofield, Ph.D. Skidmore College