Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Short Communication - (2016) Volume 4, Issue 1
Objective: To compare ‘quality of life-related to eating and exercise’ (QOL ED) in women with and without PCOS who are seeking fertility treatment.
Method: Twenty-one women with and 128 women without PCOS aged 20 to 46 years attending IVF clinics in Sydney, Australia participated. Participants completed the QOL ED questionnaire containing six eating disorder subscores and a global score. Multivariate analyses included age and Body Mass Index (BMI) as covariates and logistic regression included current BMI.
Results: Women with PCOS had significantly poorer QOL ED global scores and poorer eating behavior, eating disorder feelings, psychological feelings and acute medical subscores. The total PCOS group was best represented by current BMI and the acute medical subscore. The non-obese PCOS group (BMI 19 to 29.9 kg/m2) was best represented by the eating disorder feelings subscore (reflecting a preoccupation with control of body weight and eating). Women with PCOS were significantly more likely to obtain a QOL ED global score above a non-eating disorder range (total sample 17% versus 8%; non-obese women 44% versus 12%) and a global score consistent with the presence of a current diagnosis of an eating disorder (total group 14.6% versus 2.3%; non-obese 22.2% versus 1.8%).
Conclusion: These findings support the assessment of disordered eating and lifestyle change as the first-line treatment of women with PCOS irrespective of BMI.
<Keywords: PCOS, Polycystic ovary syndrome, Infertility, Eating pathology, QOL ED
PCOS is a syndrome of clinical and/or biochemical signs of androgen excess, ovulatory dysfunction and polycystic ovaries with at least two of the three criteria to be present for a diagnosis. Women with PCOS are at increased risk of metabolic problems (impaired insulin resistance, impaired glucose tolerance, type two diabetes mellitus and cardiovascular disease), reproductive abnormalities (infertility, hyperandrogenism and hirsutism) and psychiatric illness (anxiety, depression and poorer quality of life). Anovulation is the predominant cause of infertility in PCOS [1].
The optimal treatment for infertile women with PCOS is not well established. Current guidelines suggest preconceptional counselling, lifestyle modifications including weight reduction and exercise, cessation of smoking, and a reduction in alcohol consumption. After these modifications, ovulation induction with anti-estrogen clomiphenes citrate, metformin or a combination of both may be trialled [2].
Approximately 60% of women with PCOS are overweight or obese [3]. Weight loss and dietary management have been associated with improved spontaneous ovulation in women with PCOS likely due to improved insulin sensitivity [4]. Polycystic ovary syndrome has also been associated with an increased prevalence of eating disorders, particularly bulimia nervosa [5]. It is suggested that psychological distress associated with adverse symptoms of PCOS may predispose individuals to disordered eating [6]. It is also suggested that eating disorders may create a hormonal environment predisposing individuals to the development of PCOS [6].
Are dietary and exercise interventions indicated prior to fertility treatment in all infertile women with PCOS? Are these interventions also indicated in infertile women without PCOS? We wish to compare the quality of life related to eating and exercise in these women. We hypothesise that infertile women with PCOS are likely to have poorer quality of life related to eating and exercise, and increased eating disorder pathology than infertile women without PCOS, independent of age and body weight.
The study was approved by the Northern Region Human Ethics Committee and IVFAustralia Ethics Committee.
Participants
The participants included 21 women with diagnosed PCOS (PCOS group) and 132 women without diagnosed PCOS (non-PCOS group) ages 20 to 46 years. PCOS was diagnosed using the Rotterdam Criteria which requires two of three of the following: clinical or biochemical signs of androgen excess, ovulatory dysfunction and polycystic ovaries [1]. These women were seeking fertility treatment at IVFAustralia clinics located in Westmead (21%, n=31) and Greenwich (79%, n=122) in Sydney.
Two women had been treated for an eating disorder in the past, both reported bulimia nervosa (binge eating and purging), neither had PCOS and had current BMIs 21 and 22 kg/m2. Women seeking fertility treatment for social reasons (i.e., single women or same sex couples) were excluded from the study.
Procedure
The clinics were attended fortnightly between June 2009 and April 2012 by a research assistant, and women attending their first consultation on that day were approached. Participants completed a paper consent and questionnaire on the day and the data were subsequently entered into the electronic database. Eleven percent of eligible women declined participation in the study five percent of surveys was returned incomplete (Figure 1). Women refusing to participate cited time constraints or lack of interest as their main concerns. Women provided data for the previous three months prior to assessment.
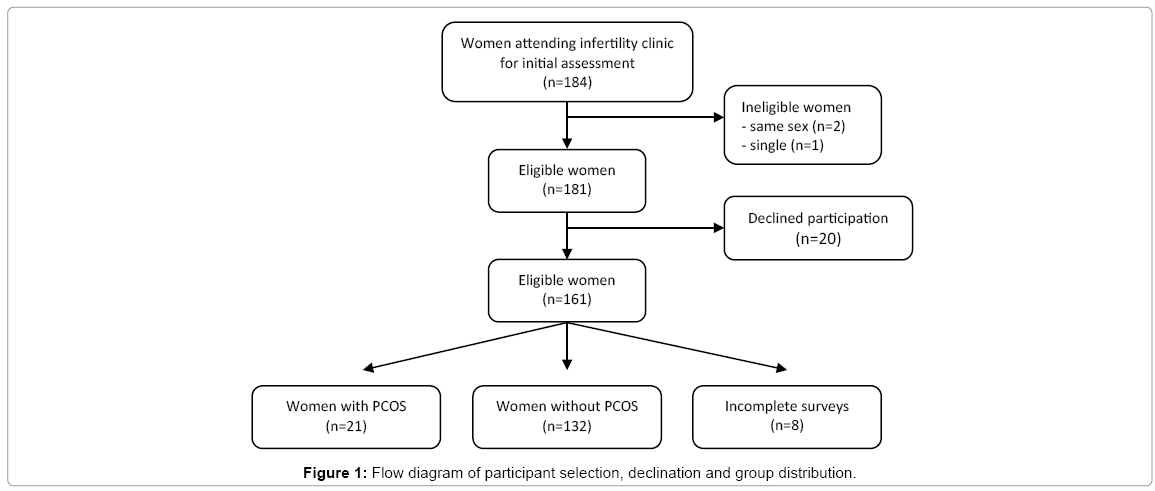
Figure 1: Flow diagram of participant selection, declination and group distribution.
Measures
Data were collected using the self-report eating and exercise examination (EEE) [7]. The EEE gathers information on height and weight, and contains the quality of life related to eating and exercise questionnaire (QOL ED). The QOL ED is a validated tool for assessing the effects of eating disorders on psychological, physical and behavioural function across time, and is contained within the EEE [7]. The QOL ED comprises 21 questions assessing five factors: eating behaviour (five questions), eating disorder feelings (five questions), psychological feelings (five questions), the effect of eating, exercise and body weight on both daily living (three questions), and acute medical status (one question assessing how their current physical health impacts their quality of life). A body weight subscore is based on BMI. A QOL ED global score is calculated from the six subscores. The QOL ED global score minus the body weight subscore (QOL ED minus BW) is also reported as eating and exercise thoughts and feelings are known to be related to body weight [7]. A QOL ED global score (minus body weight subscore) of greater than six lies outside the 95% CI of a non-eating disorder population [7]. A QOL ED global score (minus body weight subscore) greater than 10 is associated with a definite diagnosis of a current eating disorder [7].
Statistical analysis
SPSS version 21 (SPSS IBM, NY, USA) was used to perform the statistical analyses. Comparisons in descriptive details between the PCOS and non-PCOS groups were made using independent samples t tests for normally distributed continuous data and chi square for categorical data. Current BMI was significantly different between the two groups. Multiple Analyses of Variance (MANOVA) using Wilks’ Lambda tests with age and current BMI as covariates were used to compare QOL ED global scores and the five subscores between the PCOS and non- PCOS groups for the total group and non-obese group (current BMI 19 to 29.9 kg/m2). Wilks’ Lambda is reported as an F value, which when significant indicates a difference between the two groups for the score or subscore. We also determined which subscores were most predictive of the PCOS group (i.e., which of the subscores are more likely to be elevated in the PCOS group compared to the non- PCOS group). This was determined by logistic regression including current BMI and the subscores found to be significantly different in the regression for the total and non-obese groups.
Demographics and weight data
The age, current BMI and desired BMI for the PCOS and non- PCOS groups and the total and BMI 19 to 29.9 kg/m2 groups are shown in Table 1. There were no differences between education level, ethnicity and marital status between the two groups. The PCOS group had a higher BMI than the non-PCOS group. Both groups contained women above the normal and overweight categories of BMI.
| Total group (all BMI) | Non-obese (BMI 19 to 29.9 kg/m2) | |||||||||
| PCOS group | Non-PCOS | PCOS group | Non-PCOS | |||||||
| (n=21) | (n=128) | (n=9) | (n=114) | |||||||
| Mean SD | Mean SD | F | Mean SD | Mean SD | F | |||||
| Age years | 34.6 | 4.5 | 35.5 | 5.4 | 0.7ns | 34.0 | 4.7 | 35.5 | 5.5 | 0.7ns |
| Current BMI kg/m2 | 29.8 | 7.7 | 24.6 | 5.9 | 3.6*** | 22.5 | 2.5 | 22.9 | 3.0 | 0.4ns |
| Desired BMIkg/m2 | 24.9 | 5.0 | 21.9 | 2.7 | 4.2*** | 20.9 | 1.4 | 21.3 | 2.0 | 0.7ns |
| Global scores | ||||||||||
| QOL ED globala | 8.4 | 4.0 | 4.5 | 3.5 | 9.3** | 6.7 | 5.0 | 3.9 | 3.1 | 7.4* |
| QOL ED global-BWab | 6.8 | 3.6 | 3.8 | 2.9 | 9.8** | 6.6 | 4.8 | 3.4 | 2.8 | 9.7** |
| Subscores | ||||||||||
| Body weighta | 1.6 | 1.5 | 0.7 | 1.1 | 0.2ns | 0.1 | 0.3 | 0.5 | 0.7 | 1.4ns |
| Eating Behavioura | 1.7 | 0.6 | 1.3 | 0.6 | 4.0* | 1.6 | 0.8 | 1.2 | 0.6 | 4.2* |
| Eating disorder feelingsa | 1.3 | 0.9 | 0.7 | 0.9 | 4.6* | 1.4 | 1.1 | 0.6 | 0.8 | 10.0** |
| Psychological feelingsa | 1.5 | 0.9 | 0.9 | 0.9 | 5.0* | 1.7 | 0.9 | 0.9 | 0.9 | 5.6* |
| Effect on daily livinga | 1.0 | 1.0 | 0.5 | 0.8 | 1.6ns | 1.0 | 1.3 | 0.5 | 0.7 | 4.3* |
| Acute medical statusa | 1.3 | 1.5 | 0.4 | 0.9 | 10.3** | 0.9 | 1.4 | 0.3 | 0.9 | 3.2ns |
| n | % | n | % | χ2 | n | % | n | % | χ2 | |
| QOL ED global-BWb>6c | 10 | 47.6 | 22 | 16.7 | 10.5** | 4 | 44.4 | 14 | 12.3 | 6.9* |
| QOL ED global-BWb>10c | 3 | 14.3 | 3 | 2.3 | 6.7* | 2 | 22.2 | 2 | 1.8 | 11.7* |
Table 1: Descriptive details and QOL ED global scores and subscores comparing the PCOS and non-PCOS groups.
QOL ED global scores
The QOL ED global score, the QOL ED minus BW score and subscores for both the PCOS and non-PCOS groups for the total group and non-obese group are shown in Table 1. The PCOS group had a significantly poorer (higher) QOL ED and QOL ED minus BW scores than the non-PCOS group after controlling for BMI and age. Eight of the 9 non-obese women with PCOS had BMI’s between 20 and 25 kg/m2.
QOL ED minus BW score of greater than six and greater than ten was more frequent for PCOS total group and the non-obese group (Table 1).
QOL ED subscores
The results for the subscores are shown in Table 1. The total and non-obese PCOS groups had a poorer QOL (scored higher) for the subscores: eating behaviour, eating disorder feelings and psychological feelings (after controlling for age and BMI). The acute medical status was poorer for the total PCOS group, whereas the effect on daily living was poorer for the non-obese PCOS group. The best indicators of PCOS in the total group were BMI and the acute medical status subscore. The best indicator of PCOS in the non-obese group was the eating disorder feelings subscore.
Our study is the first to examine quality of life related to eating and exercise in women (with and without PCOS) seeking fertility treatment. These results suggest that women with PCOS have a poorer quality of life related to eating, and increased eating disorder pathology than other women seeking fertility treatment. The differences in eating pathology and the increased likelihood of eating disorders were present even when controlling for BMI.
Approximately 17% of all women and 12% of non-obese women without PCOS seeking fertility treatment had QOL ED scores above the range of women without eating disorders. Although the QOL ED scores consistent with a diagnosis of a current eating disorder were 2.3% and 1.8% which is within the 5% prevalence of eating disorders previously found in populations of women prior to pregnancy [8].
There is disagreement in the literature about the prevalence of eating disorders among women seeking infertility treatment, up to 21% [9,10]. Although the numbers are small in this study the data supports the increased incidence of eating disorders for women with PCOS but not for other infertile women. The discrepancy in the literature may reflect the different measure of eating disorders. In this study a QOL ED above the population range suggested a higher incidence of eating disorders, but women without PCOS were within the expected range when considering only those women scoring in the eating disorder diagnostic range.
A criticism of this study may be the small sample size, particularly of women with PCOS. Additionally, our questionnaire did not include information regarding the period and cause of infertility, the outcome of fertility treatment and medical comorbidities. This study suggests significant eating and exercise pathology in infertile women seeking fertility treatment, however larger more detailed studies are required to confirm and explore these results. We relied on women to self-report their height and weight. The body weight subscale score was omitted from the global QOL ED score and comparisons for global scores and subscores were performed with current BMI as a covariate. BMI was a significant covariate so BMI was included in the analysis of the best subscores reflecting PCOS. BMI and the acute medical subscore were predictive of the presence of PCOS when the women above BMI 29.9 kg/m2 were included in the analysis. This suggests the women’s QOL, particularly their medical status was related to their obesity. Non-obese women with PCOS were more preoccupied with controlling their eating and body weight; a major feature of women with eating disorders [11].
Lastly the Rotterdam Criteria has been criticised as over-diagnosing the prevalence of PCOS, as a result of vaguely defined criteria for clinical and/or biochemical hyperandrogenism, the high prevalence of polycystic ovaries in younger women and the requirement of only two of three criteria to be present for a diagnosis [12].
Future research should repeat this study with larger numbers to obtain more robust significance values to confirm our findings particularly with ‘normal’ and ‘non-obese’ women. The outcome of women with PCOS seeking fertility treatment should also be assessed to determine firstly if lifestyle interventions are more effective in women with higher eating disorder pathology, and secondly if eating disorder pathology has an effect on IVF outcome.
In conclusion, women seeking fertility treatment for PCOS have a poorer quality of life related to eating and exercise and a higher proportion of women with probable eating disorders than women without PCOS seeking fertility treatment. These findings support the guidelines recommending lifestyle changes as the first-line treatment for infertile individuals with PCOS. Women with PCOS seeking fertility treatment regardless of their BMI should be assessed for eating disorder pathology and the necessary treatment implemented prior to other fertility interventions. An assessment of eating and exercise may also be appropriate in women without PCOS seeking fertility treatment.
We would like to acknowledge the assistance of IVFAustralia staff Jane Early and Belinda Jones for their assistance with data collection.