Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2012) Volume 2, Issue 2
We investigated the safety of peptide vaccination with HLA-A2402-restricted KIF20A and VEGFR1 epitope peptides in patients with advanced pancreatic cancer that was refractory to chemotherapy. This was a prospective nonrandomized, single-arm, phase I clinical trial with a fixed 2-mg dose of KIF20A and VEGFR1 peptides for patients with advanced unresectable pancreatic cancer. We determined the HLA genotype of the subjects after enrollment, results of which were held by the evaluative committee and kept from both patients and investigators until completion of the study. The primary endpoint was safety of the peptide vaccination with secondary endpoints being the immunological responses and clinical outcome. We compared study endpoints between the HLA-A*2402-positive and HLA-A*2402- negative groups. KIF20A and VEGFR1 peptides were subcutaneously administered on days 1, 8, 15, and 22 within a 28-day treatment cycle. Nineteen patients diagnosed with unresectable pancreatic cancer were enrolled from May 2009 to January 2010 at our Hospital. Twelve of the 19 patients received 4 or more vaccinations (at least one course). No patient had a severe adverse event in relation to this treatment. Findings from evaluation of clinical responses after one course showed that 2 cases had stable disease and 10 progressive disease. The median overall survival time (MST) for the 12 patients was 5.3 months. In the HLA-A*2402-positive group and HLA-A*2402-negative group, the MST was 6.0 months and 2.3 months (p=0.0373), respectively. Results of this study showed that vaccination with KIF20A and VEGFR1 peptides was a safe treatment, might be a promising treatment. This trial was registered with University Hospital Medical Information Network (UMIN) number UMIN000002022.
<Keywords: Pancreatic cancer, Peptide vaccination, Phase I clinical trial
The majority of patients with pancreatic cancer are diagnosed in the advanced, unresectable stage; therefore, pancreatic cancer has a high mortality. Single-agent gemcitabine (GEM) is the standard chemotherapy for unresectable pancreatic cancer at present, although its effect (median overall survival time (MST), 5.7 months; overall 1-y survival, 18%) has not been satisfactory [1].
Although some phase III trials of combination chemotherapy of cytotoxic agents with GEM have been attempted, statistically significant improvement in survival compared with treatment by GEM alone has not been shown [2-7]. Erlotinib, an oral human epidermal growth factor receptor type 1 tyrosine kinase inhibitor, in combination with GEM showed a statistically significant improvement in MST compared with treatment using GEM alone (erlotinib with GEM 6.24 months vs. GEM alone 5.91 months; p=0.038) [8]. This result showed only minimal prolongation of overall survival. Conroy et al. [9] reported a phase III trial that compared FOLFIRINOX (5FU/ leucovorin, irinotecan, and oxaliplatin) vs. GEM in ASCO2008. FOLFIRINOX was superior to GEM with regard to response rates (31.6% vs. 9.4%) and MST (11.1 months vs. 6.8 months). However, the toxicity was remarkable, and the FOLFIRINOX regimen has not been recognized as a standard treatment for pancreatic cancer with metastasis. Thus, novel treatment modalities to improve survival in patients with advanced pancreatic cancer are required.
Anticancer immunotherapy is considered to be a candidate modality for pancreatic cancer. Recently, analyses of gene expression profiles of cancer and normal cells using cDNA microarray technologies have provided an effective approach for the identification of tumor-associated antigens [10-17].
KIF20A belongs to the family of kinesin proteins, which are characterized by a conserved motor domain that binds to microtubules and couples ATP hydrolysis to generate mechanical force [18,19]. KIF20A was first identified to localize to the Golgi apparatus and to have an important role in the dynamics in this organelle by an interaction with the GTP-bound form of Rab6 [19]. Taniuchi et al. reported that KIF20A had been over expressed in pancreatic cancers analyzed on a cDNA microarray [20].
Vaccination with peptides derived from VEGFR-1 was shown to inhibit tumor growth in mice [21]. Ishizaki et al. [21] established CTL clones in vitro from human peripheral blood mononuclear cells with HLA-A*2402. These CTL clones were shown to have potent cytotoxicity in an HLA class I-restricted manner not only against peptide-pulsed target cells but also against target cells endogenously expressing VEGFR1. These results strongly suggest that VEGFR1 is a promising target for an antiangiogenic cancer vaccine and that further clinical development of this strategy is warranted.
We investigated the safety of peptide vaccination with HLAA2402- restricted KIF20A and VEGFR1 epitope peptides in patients with advanced pancreatic cancer that was refractory to chemotherapy.
Patient eligibility
Patients diagnosed with unresectable pancreatic cancer were enrolled in this trial from May 2009 to January 2010 at Juntendo University Hospital, Tokyo, Japan.
Inclusion criteria were as follows: (1) unresectable/recurrent pancreatic cancer refractory to chemotherapy or treatment could not be continued because of adverse events; (2) Eastern Cooperative Oncology Group (ECOG) performance status 0-2; (3) age over 20 years but less than 85 years; (4) presence or absence of measurable or evaluable lesions by Response Evaluation Criteria in Solid Tumors (RECIST) criteria was not taken into account; (5) surgery performed and recovery achieved or two weeks or more had passed since previous treatment; (6) survival of 3 months or longer expected; (7) white blood cell count >3000/mm3 but <15000/mm3, platelet count >75000/mm3, aspartyl aminotransferase (AST) and alanyl aminotransferase (ALT) <150IU/L, total bilirubin < 3.0 mg/dl and creatinine <2.0 mg/dl; and (8) written informed consent provided prior to the trial.
Criteria for exclusion of patients were: (1) pregnancy or lactation; (2) uncontrollable severe infectious diseases; (3) receiving treatment with steroid or immunotherapy at the time of this clinical trial; (4) presence of 2 or more uncontrollable malignancies; (5) presence of severe trauma; (6) insufficient recovery from an injury; and (7) being judged inappropriate as a participant by doctors.
Study design and treatment schedule
This study was a prospective non-randomized, double blind, single arm, phase I clinical trial with a fixed 2-mg dose of KIF20A and VEGFR1 peptide for patients with advanced unresectable pancreatic cancer. We determined the HLA genotype of the subjects after enrollment, results of which were held by the evaluative committee and kept from both patients and investigators until completion of the study. We compared data on the study endpoints between the HLA-A*2402-positive group and the HLA-A*2402-negative group. We established each dose of the vaccinated peptide to be 2 mg/body based on the results of past clinical trials. This study was approved by the Juntendo University Hospital’s ethical committee. This trial was registered with University Hospital Medical Information Network (UMIN) number UMIN000002022 (http://www.umin.ac.jp).
Endpoints
The primary endpoint of this trial was the safety of the peptide vaccination, and safety was evaluated according to the National Cancer Institute Common Toxicity Criteria (ver. 3.0). Immunological reactions at the injection sites (RAI) were defined by erythema and/or induration. The secondary endpoints were immunological responses and clinical outcome. Clinical outcomes included assessment using CT scanning in accordance with RECIST criteria, time to progression (TTP), and overall survival (OS). The effect of tumor reduction was evaluated at the end of one course according to RECIST criteria. CT scanning was performed after the first and second cycles, and thereafter after 2 cycles. TTP was determined as the time from the date of the initial vaccination until the documentation of clear disease progression. OS was calculated from the date of the initial vaccination to the date of death from any cause.
Treatment schedule
We established each dose of the vaccinated peptide to be 2 mg/ body based on the results of past clinical trials [22]. The KIF20A peptide and the VEGFR1 peptide were administered emulsified with incomplete Freund’s adjuvant (Montanide ISA*51VG; SEPPIC, Paris, France) and subcutaneously given on days 1, 8, 15, and 22 in a 28-day treatment cycle. The administration of the peptide vaccination was repeatedly performed until at least one course had been given.
Definition of dose-limiting toxicity (DLT)
DLT was defined as hematological toxicity of grade 4 or nonhematological toxicity of grade 3 or greater (excluding nausea, vomiting) when it could not be ruled out that peptide vaccination was the cause.
Peptides
The peptide with Good Manufacturing Practice grade to treat patients and measurement of CTL response, VEGFR1-peptide were synthesized and analyzed their quality by the American Peptide Company Inc. (Sunnyvale, CA, USA). KIF20A-peptide were synthesized and analyzed their quality by NeoMPS,
(San Diego, CA, USA).
Statistical analysis
TTP and OS curves were estimated using Kaplan–Meier methodology.
Characteristics
• A total of 19 patients were enrolled in this study. Twelve of the 19 patients received 4 or more vaccinations (at least one course), making these 12 patients eligible for evaluation. Characteristics of the 12 evaluated patients (9 males, 3 females; average age 63.4 years) are shown in Table 1. ECOG PS was 0 in 6 patients, 1 in 5 patients, and 2 in 1 patient. All 12 eligible patients previously had received chemotherapy, with 5 patients also undergoing surgery and 1 patient radiotherapy. Seven patients had liver metastasis, 4 had lymph node metastasis, 2 had lung metastasis, 2 had peritoneal dissemination, and 1 patient had bone metastasis. Eight of the 12 patients belonged to the HLA-A*2402- positive group.
| Patient | Primary | Prior Therapy | ||||||
| No. | Sex | Age | PS | Tumor Site | HLA | Surgery | Chemotherapy/ Radiation (RT) | Metastatic Sites |
| M | 61 | 1 | Pt | non A2402 | - | GEM+S-1 | Liver | |
| F | 73 | 0 | Pb | A2402 | - | GEM+S-1 | Liver | |
| M | 61 | 1 | Ph | A2402 | - | GEM+S-1 | Lymphaden | |
| M | 69 | 1 | Ph | A2402 | + | GEM | Lung, Lymphaden, Peritoneum | |
| M | 70 | 0 | Ph | non A2402 | - | GEM | Liver | |
| M | 52 | 0 | Ph | A2402 | + | S-1, GEM | Liver | |
| F | 66 | 0 | Ph | A2402 | + | GEM, S-1, RT | Liver | |
| M | 61 | 2 | Pt | A2402 | + | GEM, S-1 | Liver, Peritoneum | |
| M | 69 | 0 | Pb | non A2402 | + | S-1, GEM+S-1 | Liver | |
| M | 61 | 1 | Ph | A2402 | - | GEM, S-1 | Lymphaden | |
| M | 62 | 0 | Pt | A2402 | - | GEM, S-1 | Lung, Bone | |
| F | 56 | 1 | Pb | non A2402 | - | GEM | Lymphaden | |
Table 1: Characteristics.
Toxicity
All 12 eligible patients were evaluated for adverse events (Table 2). No patient had a severe adverse event in relation to this treatment. Nine of the 12 patients had erythema, pruritus, or induration at the injection sites (reactions at the injection sites; RAI) (Table 3). Of the 3 patients without RAI, 2 patients belonged to the HLA-A*2402- negative group.
| Toxicity | Grede | Total patients n=12% |
|||
| 1 | 2 | 3 | 4 | ||
| Blood/ Bone marrow | |||||
| Leukopenia | 1 | 1 (8.3) | |||
| Anemia | 2 | 2 (16.7) | |||
| Thrombocytopenia | 2 | 2 (16.7) | |||
| Metabolic | |||||
| Hypernatremia | 1 | 1 (8.3) | |||
| Hyponatremia | 1 | 2 | 3 (25) | ||
| Hypokalemia | |||||
| Hepatic | |||||
| Elevated AST | 3 | 1 | 4 (33.3) | ||
| Elevated ALT | 1 | 1 | 2 (16.7) | ||
| Elevated ALP | 3 | 1 | 4 (33.3) | ||
| Elevated billirubin | 1 | 1 | 2 (16.7) | ||
| Renal | |||||
| Creatinine | 1 | 1 (8.3) | |||
| Constitutional symptoms | |||||
| Fever | 2 | 2 (16.7) | |||
| Anorexia | 5 | 2 | 7 (58.3) | ||
| Fatigue | 3 | 3 (25) | |||
| Edema | 2 | 2 (16.7) | |||
| Gastrointestinal | |||||
| diarrhea | 1 | 1 (8.3) | |||
| nausea/ vomiting | 4 | 1 | 5 (41.7) | ||
Table 2: Summary of toxicity.
| PatientNo. | HLA | Antitumor effect | Dermatology (Grade 1) | |||
| 1course | 2course | Rash | Induration | Pruritus | ||
| 1 | non A2402 | PD | ||||
| 2 | A2402 | PD | PD | 1 | ||
| 3 | A2402 | PD | ||||
| 4 | A2402 | PD | 1 | 1 | ||
| 5 | non A2402 | PD | ||||
| 6 | A2402 | PD | 1 | |||
| 7 | A2402 | PD | 1 | |||
| 8 | A2402 | SD | 1 | |||
| 9 | non A2402 | PD | PD | 1 | ||
| 10 | A2402 | PD | 1 | |||
| 11 | A2402 | SD | SD | 1 | 1 | |
| 12 | non A2402 | PD | PD | 1 | 1 | |
Table 3: Dermatology and Clinical outcome.
Clinical outcomes
The evaluation after one course showed stable disease in 2 cases and progressive disease in 10 cases (Table3). The two cases with stable disease were HLA-A*2402-positive. The MST was 5.3 months when all 12 patients were analyzed. Comparison of the HLA-A*2402-positive group and the HLA-A*2402-negative groups showed the MST to be 6.0 months and 2.3 months (p=0.0373), respectively (Figure 1).
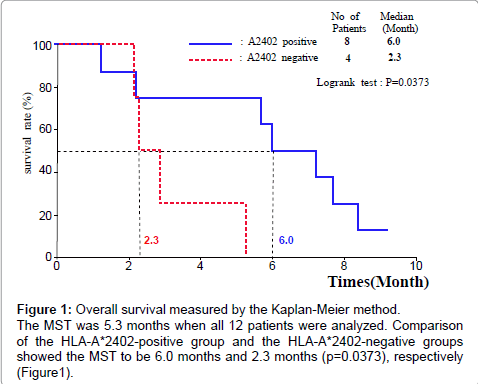
Figure 1: Overall survival measured by the Kaplan-Meier method. The MST was 5.3 months when all 12 patients were analyzed. Comparison of the HLA-A*2402-positive group and the HLA-A*2402-negative groups showed the MST to be 6.0 months and 2.3 months (p=0.0373), respectively (Figure1).
CTL response
An IFN-γ ELISPOT assay was conducted using PBMC periodically obtained from patients to assess the cellular immune responses to KIF20A and VEGFR1. Positive CTL responses specific to the vaccinated peptide were determined as previously described [22]. The positive CTL responses to KIF20A were seen in five of the eight patients (62.5%), to VEGFR1 were three patients (37.5%).
Although some phase III trials of combination chemotherapy of cytotoxic agents have been attempted for advanced pancreatic cancer, results have been no more satisfactory than treatment with GEM alone [2-7]. Recently therapeutic cancer vaccinations have attracted attention as a novel cancer treatment.
The US Food and Drug Administration (FDA) approved an autologous cellular vaccine (Provenge®) for the treatment of prostate cancer. The approval was based on results of a clinical phase III trial comprised of 512 patients with asymptomatic or minimally symptomatic metastatic prostate cancer in which OS was increased by 4 months compared to placebo [23]. The MAGRIT trial began in October 2007 to investigate the efficacy of MAGE-A3 antigen-specific cancer immunotherapeutic agents in preventing cancer relapse when administered after tumor resection in patients with MAGE-A3- positive stages IB, II, and IIIA non-small cell lung cancer [24].
Recently, clinical trials using epitope peptides for oral cancer [25] and melanoma [26] were reported. Miyazawa et al. [22] reported a phase I clinical trial combining VEGFR2 peptide vaccine with GEM that was conducted in patients with advanced pancreatic cancer. The disease control rate was 67%, and the MST was 8.7 months. No doselimiting toxicity was observed in each dose cohort. They assumed the optimal dose of the peptide for further clinical trials to be 2 mg/body.
We observed no severe adverse reaction related to the treatment in this trial. Specific adverse events related to this vaccine treatment were RAI. Of the 3 patients without RAI, 2 patients belonged to the HLA-A*2402-negative group. The MST in the patients with RAI was 6.0 months while it was 2.2 months (p=0.0426) in the patients without RAI. It was reported that RAI may be a surrogate marker to predict clinical response to peptide vaccination [26]; our results also suggested this possibility.
In reports of combination therapy with anticancer agents and vaccination, there has been no investigation of safety and clinical outcome from peptide vaccination according to HLA type. Among the Japanese population, 60.8% share a common HLA-A*2402 allele [27]. Although this trial had a small number of patients, we did recognize that overall survival was prolonged in the HLA-A*2402- positive group in comparison with the HLA-A*2402-negative group (MST 6.0 months vs. 2.3 months, p=0.0373: Figure1). Although, in this study, we did not use placebo, patients with HLA-A*2402- negative became control group naturally because these peptides are HLA-A*2402 restricted. In examining OS, we included patients who had dropped out of the study. This peptide vaccination was effective in patients with depending on status of HLA-A*2402 positive states, and it should be a significant difference in OS between positive or negative HLA-A*2402 groups.
At present, we are investigating the clinical outcome in a phase II clinical trial using peptide vaccination with HLA-A2402-restricted KIF20A and VEGFR1 epitope peptides in patients with advanced pancreatic cancer.
Results of this study showed that vaccination with KIF20A and VEGFR1 peptides was a safe and feasible treatment. We would like to further investigate clinical outcome using this treatment.
The authors would like to thank Prof. Yusuke Nakamura, Dr. Takuya Tsunoda, Dr. Koji Yoshida, Mr. Ryuji Osawa, and Ms. Sachiko Yoshimura, Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, The University of Tokyo, for their excellent advice and cooperation and providing all the peptides. And we also great thank for Prof. Hideoki, Ogawa Chairman of the Board of Directors, Juntendo University, Prof. Ko Okumura, Juntendo University, Prof. Eiki, Kominami President of Juntendo University, Prof. Yasuhiko Tomino, Dean, Juntendo University, Prof. Hajime Arai, Director and Prof. Kazuhiro Sase, Juntendo University Hospital for excellent lead and suggestion.