Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Research Article - (2016) Volume 4, Issue 1
Introduction: Pedicle screw fixation is frequently applied to treat patient with degenerative diseases of lumbar spine and the reported rate of screw loosening may achieve the level of over 50% in case of osteoporosis. In this study, we hypothesized that a threshold of bone density in HU could be identified, below which the risk of pedicle screws loosening may be significantly increased.
Materials and methods: This is a prospective non-randomized study of patients with degenerative diseases of lumbar spine that underwent spinal instrumentations with pedicle screw fixation, 110 patients were enrolled. Preoperatively computed tomography was administered and bone density of trabecular bone of vertebra body was measured. Standard intervention includes pedicle screw fixation, unilateral foraminotomy and transforaminal interbody fusion with cage and autograft. Minimal follow-up period accounted for 18 months, cases with evident pedicle screw loosening on CT scans were registered. Logistic regression analysis was used to estimate the relationship between bone density loss and probability of implant instability.
Results: Logistic regression analysis demonstrated a strong inverse relationship between bone density measured in Hounsfield units and frequency of all cases of pedicle screws loosening. The obtained logistic regression equation analysis using derivatives of a high order showed a critical point of 81 HU that corresponds to the acceleration of total implant instability probability growth per unit of bone density loss.
Conclusion: Bone density in HU can be used as a criterion for implant instability prediction as far as a strong relation has been estimated between screw loosening probability growth and the decrease in bone density. Breakpoint of 81 HU corresponds to the increased risk of pedicle screws instability development.
<Keywords: Computed tomography; Spinal instrumentations; Screw loosening; Hounsfield units
Degenerative diseases of lumbar spine are commonly encountered clinical conditions in the adult population; sometimes this pathology requires stabilizing operative interventions. Pedicle screw fixation is frequently used to treat those patients, however implant instability have a considerable incidence in this group. It has been reported that the rate of this complication varies from 4% to 19-20% and even may rich a level of over 50% in patients with osteoporosis [1,2].
It has been shown that bone augmentation with various types of cement is effective to decrease the frequency of pedicle screws loosening, on the other hand the risk of intracanal and extravertebral cement leakage is significant in those patients [3,4]. In addition, cases with cement pulmonary embolism were also reported [5]. Apparently, the decision to perform bone augmentation should be supported by valid criterion that may justify the appropriate ratio of potential risks and benefits.
Computed tomography (CT) is a commonly employed diagnostic modality useful in the workup of a variety of spinal conditions. CT data is capable of accurately defining bone density using Hounsfield units (HU). The HU scale represents the relative radiodensity of a body tissue according to a calibrated gray-level scale, based on the values for air (−1000 HU) and water (0 HU); this scale is slightly non-linear [6]. The use of the HU scale has been utilized to measure the likelihood of success in dental implants and lumbar fusion, procedures which rely on a stable bone-implant interface [7-9]. In this study, we hypothesized that a threshold of bone density in HU could be identified, below which the risk of pedicle screws loosening may be significantly increased.
This is a prospective non-randomized study of patients with degenerative diseases of lumbar spine that underwent spinal instrumentations with pedicle screw fixation during the period of 2012-2013. One hundred and ten patients were enrolled in this study. Minimal period of follow-up accounted for 18 months. This study had been approved by IRB committee, written consent was received from all patients participating in this study.
Inclusion criterion was:
Degenerative disease that required spinal stabilization with pedicle screw fixation
Exclusion criteria were:
1. Presence of oncology
2. The use of bisphosphonates and other medications relevant to osteoporosis treatment prior to surgical intervention
3. Degenerative deformities that required correction
4. Implant malposition
Preoperatively computed tomography was administered to clarify the specificity of degenerative pathology and also bone density was measured in Hounsfield units on the level of L3. The CT scans were performed using a single CT scanner (Aquilion 32, Toshiba Corporation). The scans utilized a slice thickness was 0.5 mm, covering a scan area of 50 cm. The scan parameters included: tube voltage 120kV, tube current 300 mA, auto mAs range 180-400; 1.0 sec/3.0mm/ 0.5x32, helical-pitch 21.0. Integrated software was utilized for calculations of bone density (Vitrea Version 5.2.497.5523) incorporating a window width/window level ratio of 2000/500. Measurements of bone density of the cancellous portions of the vertebral bodies were obtained in HU at the level of L2 or L3 in the sagittal, axial and coronal planes. Measurements in the axial plane were taken at the level of the middle of the pedicles. Measurements in the sagittal and coronal planes were taken along the geometric center of vertebra body. Oval-shape trabecular bone samples were selected using the maximal achievable diameters without traversing into cortical bone to calculate bone density in each plane.
Standard technique was used to treat patients that include pedicle screw fixation, unilateral foraminitomy and transforaminal interbody fusion with cage and autograft; the number of operated levels ranged from 1 to 5.
Postoperatively planar X-ray examination was administered by the end of the third month after intervention, control CT was administered after 6-th and 12-th months mandatory and after 18-th months – optionally if fusion had not been achieved by 12 month of follow up. Cases with evidence of screw loosening were detected and registered. The criterion for pedicle screw loosening was radiolucent zone around the screw detected on CT images (Figure 1) [10]. Instability of implant was classified as partial and total if all screws were unstable.

Figure 1: CT axial image, radiolucent zone around pedicle screw is evident.
Statistical power analysis was performed to calculate the required sample size. Logistic regression analysis was performed to estimate the relationship between screw loosening rate and bone density measured in Hounsfield units. Derivatives of high orders were used to study the specificities of the estimated regression function.
This study included 75 females (68,2%) and 35 males (31,8%) with a mean age of 53 years (21-75 years). The age and bone density measurements are shown in Table 1.
| n=100 | Mean (mean+Standard error of mean) |
Standard deviation | Maximum | Minimum |
|---|---|---|---|---|
| Patient age | 53,81+1,15 | 12,11 | 75 | 21 |
| Mean bone density HU | 122,93+3,82 | 40,06 | 243,97 | 44,47 |
Table 1: Age and bone density measurements for the study cohort
By the end of follow-up period 55 patients presented with CT signs of pedicle screw loosening, 11 out of those reported were proved to have total instability of implants.
The logistic regression analysis demonstrated a strong inverse relationship between bone density measured in Hounsfield units and frequency of pedicle screws loosening. The parameters of the logistic regression model were ?0=-3,087054, p=0,0002; B1=0,0254, p=0,0001. Odds ratio(OR)=159,9735, 95% confidence interval (CI) [12,81554 ; 1996,914]. Coefficient of determination (R) = 92. Goodness of fit: Chisquare= 20,91574; p<0,0001. The graph of estimated regression equation was analyzed using derivatives of high orders and no critical points were found within clinically significant segment of 0-240 HU.
Cases with total implant instability were analyzed separately and again a strong relation was shown between total implant instability rate growth and bone density in Hounsfield units getting decreased. The parameters of the logistic regression model were ?0=-0,8596, p=0,4797 (insignificant); B1=0.0282, p=0,0202. OR=276,5576; 95% CI [2,440634 ; 31337,81], R=92. Goodness of fit: Chi-square=7,5264; p=0,0061. The obtained logistic regression equation analysis showed a critical point of 81 HU associated with the significant increase in rate of total implant instability (critical point associated with total implant instability probability growth acceleration per unit of bone density loss was detected using derivatives of logistic regression function of a high order). The estimated logistic regression graph with detected breakpoint is presented on Figure 2.
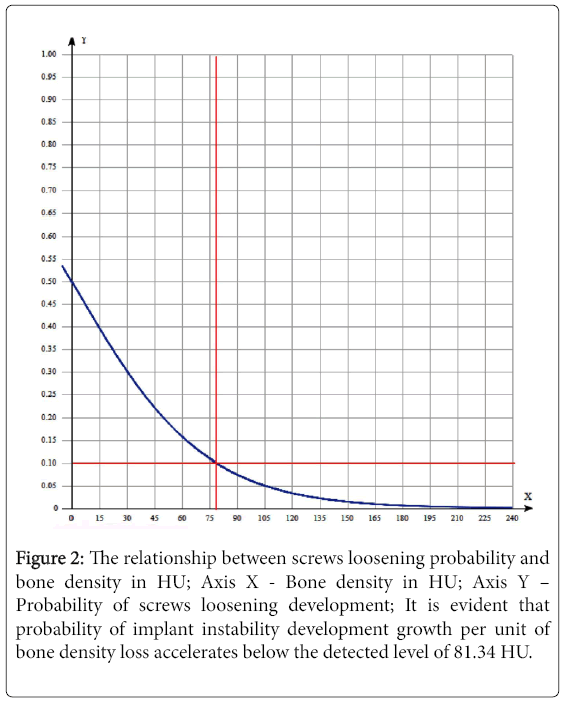
Figure 2: The relationship between screws loosening probability and bone density in HU; Axis X - Bone density in HU; Axis Y – Probability of screws loosening development; It is evident that probability of implant instability development growth per unit of bone density loss accelerates below the detected level of 81.34 HU.
Osteoporosis is a frequently detected morbid condition in the aged group of patients, this diagnosis is valid if T criterion value declines down to -2,5 and below and if bone mineral density averaged for lumbar levels is less than 0.8 g/cm2 [11]. Despite some guidelines for treatment and injury prevention have been worked out based on those criteria, the relationships between bone density loss and implant instability rate development after spinal instrumentations have not been estimated clearly yet [12]. Evaluation of those relationships might be helpful as far as clear guidelines for bone augmentation could be worked out to avoid further implant instability development after spinal instrumentations.
Computed tomography is frequently applied to determine the specificities for spinal pathology also bone density in HU can be evaluated so that data can be used for bone quality assessment. Despite the fact that bone density in HU has not been calibrated for osteoporosis detection, it has been proved that those figures have a strong positive relation with T-criterion and represent bone strength [13-15]. On the other hand clinicians are interested in criterion that will be helpful in complication prediction and decision making rather than just in getting the diagnosis of osteoporosis validated.
Logistic regression analysis demonstrated a strong inverse relationship between bone density measured in Hounsfield units and frequency of pedicle screws loosening. Estimated highly significant regression equation with statistically significant coefficients provides the evidence that likelihood of occasional associations is negligible. Estimated determination coefficient value means that bone density in HU changes explain 92% of pedicle screw loosening rate variability. Taking in view that considerable proportion of screw loosening detected on CT scans has a moderate clinical significance being asymptomatic in 80% of cases; the rate of total implant instability was analyzed to evaluate the acceptable cutoff criterion for bone augmentation application. Using derivatives of a high order it has been estimated that the decrease in bone density below 81 HU results in acceleration of total instability probability growth per unit of bone density loss. This breakpoint may have a clinical significance as an indication for cement augmentation of vertebra bodies if pedicle screw fixation is going to be applied in order to avoid screws loosening.
Limitation of the present study is that it is a non-randomized one and does not represent a real incidence of screw loosening after spinal instrumentations.
Bone density in HU can be used as a criterion for implant instability prediction as far as a strong relation has been estimated between screw loosening probability growth and the decrease in bone density. Breakpoint of 81 HU corresponds to the increased risk of pedicle screws instability development.