Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2014) Volume 4, Issue 2
In over 90% of healthy people, the dorsal and ventral endodermal pancreatic buds fuse to form the adult pancreas. However, in about the remaining 10% of the population where the fusion does not occur, pancreatic divisum (PD) results. This indeed is the commonest congenital anomaly of pancreas. The dorsal root usually drains a part of pancreatic head, the body and tail of the pancreas via a minor papilla into the duodenum. The ventral root drains the uncinate process and part of the pancreatic head with the CBD via the major papilla into the duodenum and the two roots are communicated with one another. In classic PD (type1) there is a complete failure of fusion of ducts, and a small ventral duct (Santorini) drains through the larger major papilla, and a larger dorsal duct (Wirsung) drains through the smaller minor papilla. In type 2, there is a complete absence of duct of Wirsung. While in type (incomplete PD), there is a filamentous or tiny caliber communication between the dominant dorsal duct of Wirsung and duct of Santorini. In the western countries, the incomplete PD is uncommon with a reported incidence of 0.13%-0.9%. However recent reports from Japan and Korea show a much higher prevalence of 48% to 52%, of incomplete PD. In patients with a large duct, the majority of the pancreatic secretions pass through the minor papilla (instead of major) resulting in inadequate drainage and pain caused by obstruction. However while these features of PD are relatively well known, there are some aspects of PD, which are not so obvious. These include its true prevalence, its role in development of pancreatitis and carcinoma of pancreas, the genetic abnormalities and its association with pancreatitis in presence of PD and the appropriate management of these patients when symptomatic
<Keywords: Pancreatic Divisum, ERCP, Pancreatitis
In over 90% of healthy people, the dorsal and ventral endodermal pancreatic buds fuse to form the adult pancreas [1,2]. However, in about the remaining 10% of the population where the fusion does not occur, pancreatic divisum (PD) results [1-3]. This indeed is the commonest congenital anomaly of pancreas [1-3]. The dorsal root usually drains a part of pancreatic head, the body and tail of the pancreas via a minor papilla into the duodenum. The ventral root drains the uncinate process and part of the pancreatic head with the CBD via the major papilla into the duodenum and the two roots are communicated with one another. In classic PD (type1) there is a complete failure of fusion of ducts, and a small ventral duct (Santorini) drains through the larger major papilla, and a larger dorsal duct (Wirsung) drains through the smaller minor papilla [3] (figure 1). In type 2, there is a complete absence of duct of Wirsung. While in type 3 (incomplete PD), there is a filamentous or tiny caliber communication between the dominant dorsal duct of Wirsung and duct of Santorini [3] (figure 2). In the western countries, the incomplete PD is uncommon with a reported incidence of 0.13%-0.9% [4]. However recent reports from Japan and Korea show a much higher prevalence of 48% to 52%, of incomplete PD [4,5]. In patients with a large duct, the majority of the pancreatic secretions (up to 2000 ml daily) pass through the minor papilla (instead of major) resulting in inadequate drainage and pain caused by obstruction [2]. However while these features of PD are relatively well known, there are some aspects of PD, which are not so obvious. These include its true prevalence, its role in development of pancreatitis and carcinoma of pancreas, the genetic abnormalities and its association with pancreatitis in presence of PD and the appropriate management of these patients when symptomatic.
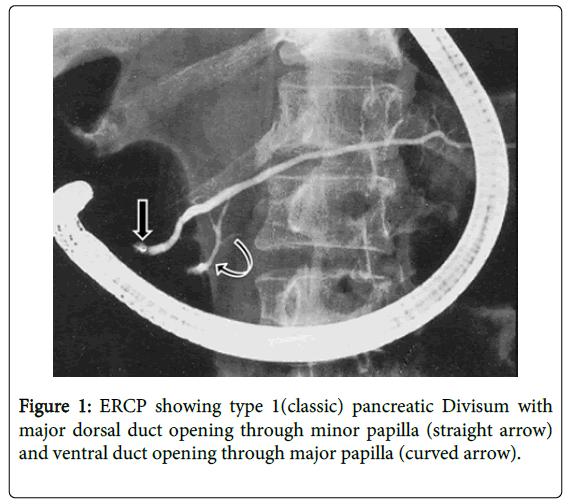
Figure 1: ERCP showing type 1(classic) pancreatic Divisum with major dorsal duct opening through minor papilla (straight arrow) and ventral duct opening through major papilla (curved arrow).
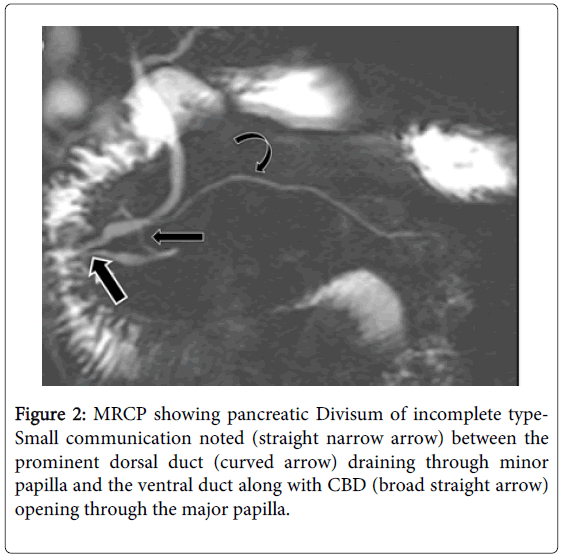
Figure 2: MRCP showing pancreatic Divisum of incomplete type- Small communication noted (straight narrow arrow) between the prominent dorsal duct (curved arrow) draining through minor papilla and the ventral duct along with CBD (broad straight arrow) opening through the major papilla.
Clinical features
Patients with PD who develop pancreatitis are typically younger in contrast to those who develop pancreatitis with normal pancreas anatomy. In addition, they are less likely to consume alcohol and are more likely to be female and have recurrent acute pancreatitis attack [6].
In a recent comprehensive analysis to determine the prevalence of PD in idiopathic pancreatitis (IP) compared to general population, data from 23 autopsy studies, 41 ERCP studies and 13 MRCP studies was analysed and the following observations were made [7,8]. In the autopsy and MRCP studies, the prevalence of PD in the general population was reported to be 8%. However in ERCP group, it was reported to be 4% in general population and 8% in patients with IP [7,8]. The difference is believed to be due to under recognition in ERCP and referral bias. In a recent systematic review of ERCP based detection rates of PD, further variation was noted based on various geographical location [9]. While the overall endoscopist detected PD was 2.9%, it was found to be 1.5% in Asia, 5.7% in United States, and 6% in Europe [9]. This geographical variation in prevalence of PD may however be attributed to the extent the endoscopist search for it and the referral bias rather than its true prevalence [8,9].
PD is reported in 3%-7% of cases of acute pancreatitis (AP) [2,8-12]. PD underlies 12%-50% of cases of AP in patients whose pancreatitis would otherwise be considered idiopathic [6]. However no clear association exists between PD and chronic pancreatitis (CP) [2,8]. Patients with PD who are otherwise well (Eg: those whose PD is discovered during imaging done for another purpose) can be reassured that they have only 5%-10% lifetime risk of developing pancreatitis [13].
However considerable controversy exists in the literature regarding whether PD is etiologically related to pancreatitis. Those who support PD being an etiological factor for pancreatitis base it on the following reasons. 1) An increased incidence (50% or 25.6%) of PD is noted on ERCP, in patients with idiopathic or recurrent acute pancreatitis (rAP) respectively [6,14]. 2) A logical explanation based on the concept of relative outflow obstruction of pancreatic juice through the minor duodenal papilla derived from provocative tests3 or due to increased dorsal ductal pressure in patients with PD compared with normal controls measured using endoscopic manometry [15]. 3) Isolated dorsal pancreatitis, as shown by irregular dilatation apparent on dorsal pancreatography alone [16,17] and 4) Improved outcome after endoscopic or surgical procedures that open the minor papilla [3,10,18]. Those who oppose these proposals argue that: 1) Fewer than 5% of the population with PD develop pancreatic symptoms [12]. 2) Some patients with PD who develop pancreatitis are not young [12]. 3) The association between pancreatitis and PD is questionable since ERCP series reflect referral populations that vary from center to center [19,20]. 4) Little direct evidence indicates outflow obstruction from the dorsal pancreatic duct during physiological pancreatic secretion; even the non-physiological secretin ultrasound test has failed to give consistent results [21]. 5) Responses to endoscopic and surgical management are variable and unpredictable [20,22]. So it appears that while there may be an association between PD and idiopathic pancreatitis (IP) and to certain extent rAP, its role in developing CP is questionable,
The frequency of PD in patients with rAP and CP of unknown origin was evaluated by MRCP [23]. The hypothesis of an interaction between anatomical and functional genetic anomalies (SPINK1, PRSS1 or CFTR gene mutation or polymorphism) was studied [23]. Patients with alcohol induced pancreatitis and subjects who underwent MRCP for non-pancreatic disease were used as controls [23]. The following observations were made. The frequency of PD was 7% in subjects without pancreatic disease, 7% in patients with alcohol induced pancreatitis, and 5%, 16%, 16% and 47% in those with idiopathic, SPINK1, PRSS1 or CFTR gene mutation associated pancreatitis [23]. The frequency of PD was higher in patients with CFTR gene associated pancreatitis as compared to those with idiopathic and alcoholic pancreatitis. CFTR mutations may increase the susceptibility to IP by at least 2 mechanisms: pancreatic ductal plugging and obstruction by viscous, proteinaceous ductal secretions [24] and by sensitizing the pancreas to an exuberant inflammatory response to injury [8]. These findings may suggest that PD by itself may not cause acute or chronic pancreatitis and that other factors such as genetic factors may play a role.
The reported incidence of pancreatic cancer in patients with PD ranges from 5.1% to 9.4% [25-27]. Among the several reports on this subject some consistent observations have been made. 1) The malignancy predominately occurs in dorsal pancreas (96% of cases) [26]. 2) The dorsal pancreatic duct shows extensive papillary hyperplasia plus atypical with a focal area of invasive adenocarcinoma, while the ventral pancreatic duct is lined with normal ductal cells [25,27]. 3) Microscopic findings of periductal and interlobular fibrosis have been detected in the non-carcinomatous pancreas of the resected pancreas implying chronic pancreatitis. Longstanding obstruction caused by relative stenosis of the minor papilla is believed to predispose to oncogenesis [25].
Investigations
Although CT scans and transabdominal scans are often used for patients with acute and chronic pancreatitis (Eg; to rule out other causes such as gallstones and pseudocyst formation), PD is not reliably detected by such scans [4,8,10,11,20,28]. In most cases PD is best diagnosed by Endoscopic retrograde cholangiography (ERCP), magnetic resonance cholangiography (MRCP), or endoscopic ultrasonography (EUS) [4,10,11,20,28]. ERCP is still considered as a gold standard for diagnosing PD [4,8,10,20]; however it is an invasive procedure and expensive, and has several drawbacks including failure to cannulate minor papilla, a high rate of complications such as ERCP induced pancreatitis, radiation and the use of iodinated contrast medium [4,20,28]. EUS is a safe first line test to evaluate PD in most patients who present with arP [28]. EUS allows the detailed evaluation of the pancreaticobiliary ductal system without injecting contrast in these ducts. Moreover, detailed images of the parenchyma is obtained [28]. Therefore EUS both radial and linear, has the potential for being minimally invasive diagnostic modality for PD [28]. A number of EUS criteria have been suggested for the diagnosis of PD [28]. These criteria have varying sensitivity and specificity and needs an objective and uniform criteria for best diagnostic accuracy [28]. Secretin EUS (S-EUS) has the potential for diagnosing minor papilla stenosis and thus helps in planning appropriate therapy [29]. On S-EUS, an abnormal response was defined as sustained (more than 10 minutes) 1mm, or more, dilatation of the dorsal duct following intravenous secretin (1 U/kg) [28,29]. EUS guided pancreatic duct interventions can help draining dorsal duct in symptomatic patients who failed minor papilla cannulation. Among the patients who were subsequently treated by stenting or sphincteroplasty, S-EUS predicted response to therapy in 95% and absence of response in 81% of patients [28,29]. EUS has a sensitivity of 100%, specificity of 81.3%, and positive predictive value of 72.7% and negative predictive value of 100% for diagnosis of PD [28, 29]. MRCP on the other hand, while having limited availability and high cost is rapidly becoming the noninvasive test of choice to diagnose PD [4]. MRCP together with MRI is without radiation, and can delineate duct and parenchyma morphology in detail [4]. Comparing to ERCP and MDCT, MRCP and MRI can be repeated more safely in follow up of patients of pancreatitis with PD since patients in this subgroup are likely to be younger and more sensitive to radiation [4]. MRCP with secretin stimulation can provide better visualization of pancreatic duct, resulting in higher sensitivity and specificity for diagnosis of the pancreatic abnormalities [4]. In addition, MRCP depicts the pancreatic duct in more physiologic state than under exogenous pressure following ERCP [4]. However, ERCP at present remains the test of choice to diagnose and manage PD for most of the patients who require therapeutic endoscopic intervention [8,11,20]. The sensitivity and specificity of the different imaging modalities have not yet been compared. While clinicians try to relate the symptoms in patients with various diagnostic tools, the abnormal findings do not play a role in decision making at most of the times. Clinical presentation are the predominant factor influencing the clinical decision for therapeutic approach [3,8,11].
The clinical conditions associated PD include rAP, CP and pancreatic type abdominal pain [1,30,31]. Most of the studies evaluating the efficacy of endoscopic treatment in PD have demonstrated best results in patients with rAP [28]. The lowest response rates have been observed in patients with only abdominal pain [31-33]. The mechanism responsible for pancreatic symptoms with PD do not necessarily develop dilation of the dorsal duct, possibly because of intermittent blockage of the pancreatic duct [28,31]. Hence it becomes difficult to identify the patients who would benefit from endoscopic therapy [28]. Various strategies to identify the best responders to therapy have been tested [7]. These include treating patients with demonstrable rAP only, or treating patients with minor papilla stenosis identified by investigations like secretin MRCP, minor papilla manometry or resistance passage of a 3 Fr, 4 Fr or 5 Fr catheters across the minor papilla during ERCP [7].
Management
The aim of treating symptomatic patient with PD is to improve the drainage of dorsal pancreatic duct by improving the patency of the minor papilla [1,4,8,11,18,20,28]. This could be achieved by endoscopic intervention or surgical procedures. Endoscopic management of symptomatic patients with PD would include minor papillotomy, papillary dilatation, stent insertion and boutilinium toxin injection, which have all been employed with varying outcome [10,18,20]. Thus, whereas historically the primary treatment approach was surgical, today a greater proportion of these patients undergo initially endoscopic therapeutic interventions. The standardized approaches include ERCP with subsequent endoscopic minor papilla sphincterotomy and sphincteroplasty or endoscopic dilatation and stenting [7,18,20,33,]. In a meta-analysis regarding the response rate of procedure in symptomatic patients with PD, following observations were made [9]. In patients who underwent endoscopic therapy, the response rate was found to be slightly lower than those undergoing surgery [69.4% -(range 33.3-100%) vs. 74.9% (range 50-100%)] respectively [9]. The response rate for patients with rAP was (79.2% for endoscopic therapy and 83.2 % for surgery) respectively [9]. However the endoscopic response was marginally higher than that of surgery, for CP group (69% for endoscopic therapy and 66.7% for surgery) respectively; p=0.029. In addition, the response rate for CP group was higher than that for pain type group [9]. While most would agree that endoscopic therapy would be the initial approach, there are others who report a good clinical outcome following a differentiated surgical approach early in the course of management, particularly after the initial failure of endoscopic intervention [10].
The surgical approach includes surgical reinsertion of the minor papilla in those patients with soft pancreas and who have no signs of inflammatory mass or fibrosis [10]. This has a reported success of 70%. The remaining 30% required second operation for persisting symptoms following which an overall 96% success rate was achieved [10]. The surgical resection and reimplantation of the pancreatic dorsal duct creates a greater orifice than simple endoscopic sphincterotomy or stenting and is the obvious reason for successful surgical outcome in those patients who failed initial endoscopic therapy [10]. In patients with signs of pancreatic fibrosis and/or inflammatory mass, a duodenum preserving pancreatic head resection is carried out. In those patients where there were no such signs and the pancreas was not hard enough for suturing, a pylorus preserving Whipple resection is recommended [10]. The outcome of the various surgical procedures have been generally good with 85% success rate following reimplantation of papilla in patient with rAP3 and 81% following duodenum preserving pancreatic head resection (DPPHR) in patients with rAP or CP [34]. An important advantage of surgical procedure compared to non-surgical approach is reduction of hospitalization from 77 days prior to operation (range 47-123) to 0 days (range 0-10.5) postoperatively [10]. The preoperative hospitalization was during a median period of 5 years of conservative management. During this period a median of 3 endoscopic interventions were carried out before surgical procedure was performed [10]. The postoperative morbidity following reinsertion of the minor papilla ranges from 25 to 34.8% and includes wound infection, anastomotic leakage; the need for second operation being 44.6% [10,35]. The morbidity post (DPPHR) and ppW (pylorus preserving Whipple) ranges from 24 to 44% [36]. The complications post endoscopic therapy ranges from 13.3% to 50% and include pancreatitis, (5-7%), haemorrhage, perforation .The overall mortality post endoscopic intervention is 5.8% and ERCP related 30 day mortality is 1% [37,38]. Interestingly there has been a recent report of managing PD associated chronic pancreatitis with Frey procedure with results comparable to the procedure being carried out in patients with alcohol induced chronic pancreatitis [39]. While the number of cases seems to be small in this series, the distinct advantage of removing the fibrotic tissue in the head of pancreas (the epicenter of pain) coupled with wide drainage of the duct and the fact that this procedure is less extensive compared to a pancreaticoduodenectomy, is appealing as a potential management option [39].
The prevalence of PD in the general population is 4-8%. Majority of these are asymptomatic and have a 5-10% lifetime risk of developing acute pancreatitis. PD may be an etiological factor in patients who develop idiopathic and recurrent acute pancreatitis particularly in the presence of CFTR gene mutations. While ERCP is still a gold standard in diagnosing and managing patients with PD, EUS and MRCP are emerging as equally good alternative in initial diagnosis. Patients are treated only when they are symptomatic and the maximum benefit is seen in patients with rAP and IP. Endoscopic intervention is considered as an initial approach for symptomatic PD. However they are associated with significant complication rate, especially when performed repeatedly. These patients who fail to respond to endoscopy therapy would benefit from surgical intervention. This would include reimplantation of minor papilla, DPPHR for patients with pancreatic fibrosis or inflammatory mass or ppW when above is not technically feasible.