Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2013) Volume 3, Issue 2
Pancreas transplantation is performed to establish a normoglycemic state and to favorably influence the secondary complications of diabetes. Before pancreas retrieval the surgeons must inspect the organ to decide whether it is transplantable, to identify abnormalities in the hepatic arterial supply, to avoid traumatic injury to the pancreas during retrieval, and to procure an intact iliac bifurcation for back-table arterial reconstruction.Our aim is to describe the standard surgical technique for pancreas transplantation debating technique for exocrine drainage such as bladder versus enteric drainage.
<Keywords: Pancreas; Transplantation; Surgical technique; Anatomical landmarks
In the 1960s and 1970s pancreas transplantation achieved insulin independence, but complications such as pancreatic fistula, pancreatitis and rejection were responsible for high percentage of postoperative failure [1,2].
After introduction of cyclosporine A better graft selection, improved surgical techniques, preservation solutions, from 1980s onward simultaneous pancreas-kidney transplantation (SPK) became the procedure of choice for type I diabetic patients with end-stage renal disease [3-9].
Our aim is to describe the standard surgical technique for pancreas transplantation debating technique for exocrine drainage such as bladder versus enteric drainage.
Donor operation
Most pancreatic grafts are obtained from multiorgan donors, providing there is no history of diabetes mellitus, chronic pancreatitis or traumatic pancreatic damage.
A long incision is made from the jugular notch to the symphysis pubis in order to assess the presence of vascular anomalies and the absence of parenchymal injury. An extended Kocher manouvre allowed the exposure of the abdominal aorta, the mesenteric vein and the origin of the superior mesenteric artery (SMA) is identified. The abdominal aorta was distally encircled for the insertion of an infusion cannula with the cold perfusion.
The lesser sac is opened and the stomach is retracted cranially. The spleen is mobilized, the pancreatic tail is reflected medially and the dissection is carried out toward the portal vein. The inferior mesenteric vein is identified and ligated, the trifurcation of the celiac axis is reached and the left gastric artery is ligated.
After incision of the gastrohepatic ligament the common hepatic artery was dissected until the celiac trunk (TC), the common bile duct was distally ligated and transected the middle colic vein and artery were divided and ligated. The origin of splenic artery (SA) was isolated and encircled. The left gastric artery was preserved in the presence of an accessory left hepatic artery. The distal pylorus was transected with a GIA stapling device. The proximal jejunum was transected and jejuneal vascular arcades were divided the SMA and superior mesenteric vein (SMV) were then isolated. Preserving the inferior pancreatic duodenal artery (IPA) intact is mandatory.
The donor was fully heparinized after completion of dissections and the distal aortic cannula was placed. Supraceliac aorta was cross-clamped and Celsior or Wisconsin solution was infused approximately 2000 to 3000 mL. The section of PV was completed leaving approximately 1 to 2 cm lengths above the pancreas. The SMA was isolated and transected. If a replaced hepatic artery is found to arise from SMA, the proximal SMA should be left in continuity with anomalous hepatic artery and the distal SMA in continuity with the IPA. The pancreas graft was then removed. A bifurcated iliac arterial graft is normally required for the pancreas. Perfusion of the pancreas was done on the bench work.
Back bench work
Whole pancreatic duodenal graft includes the entire pancreas and the first, the second and sometimes a segment of the third duodenal portion. A Y iliac graft is usually employed to create a single arterial pedicle, by anastomosing their peripheral branches to the SMA and the SA.
Ex-vivo preparation of the pancreas is performed on the back table. The ends of the duodenal segment are re-stapled to form a segment 10-12 cm long avoiding encroachment upon Ampulla de Vater, and inverted interrupted 3-0 silk sutures is performed then a donor Y-graft is anastomosed to the allograft splenic and superior mesenteric arteries using 6-0 prolene. The vessels at the head of the pancreas are over sewn with 3-0 silk sutures in order to prevent bleeding.
Recipient operation
Pancreas transplantation can be performed with either a suprainguinal, retroperitoneal approach or through a midline intraperitoneal incision. For enteric drainage, the head of the pancreas and the duodenum can project transversaly or cephalad. If the bladder drainage technique is used, the graft is oriented so that the head and duodenum project caudad, directly into the pelvis and bladder.
For the revascularization technique, the portal vein is anastomosed end-to-side to the recipient iliac vein or vena cava using running 6-0 prolene sutures. A Carrel patch of graft donor aorta encompassing both the celiac axis, superior mesenteric arteries to which the donor splenic artery has been joined, is anastomosed end-to side to the recipient common or external iliac artery using running 6-0 prolene sutures.
Duodenal anastomosis can be hand-sewn or stapled using either circular or linear device. Hand-sewn anastomoses employ an external layer of interrupted non-absorbable sutures and an internal layer of continuous absorbable material [8,9].
Enteric anastomosis can involve either proximal jejunum or distal ileum, (Figure 1) and can be constructed end-to-end and side-to-side. The use of direct anastomosis is currently prevalent over Roux-en-Y loop.
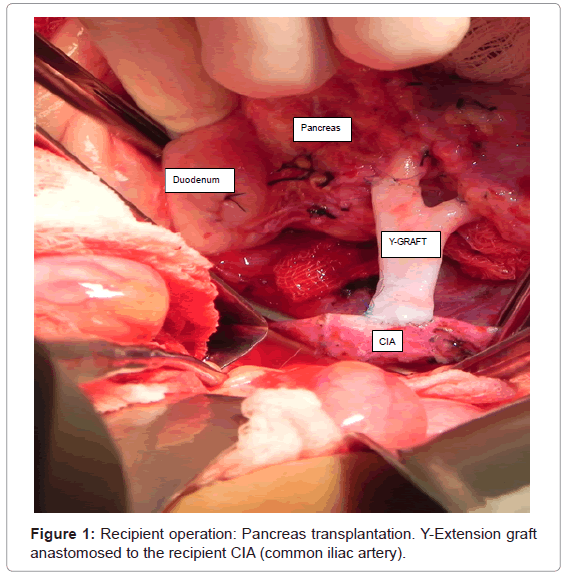
Figure 1: Recipient operation: Pancreas transplantation. Y-Extension graft anastomosed to the recipient CIA (common iliac artery).
In BD cases, the duodenal was anastomosed to the dome of the recipient bladder in a side-to-side manner. 2-layers anastomosis using 4-0 monofilament absorbable suture for an outer layer and 4-0 monofilament absorbable suture for a continuous full-thickness inner layer usually with manual anastomosis 4:0 PDS sewing.
Approximately 40 cm from the ileo-cecal valve, a segment of distal ileum, was anastomosed to the donor duodenum in a side-to-side fashion; with manual anastomosis with an interrupted double layer 4:0 PDS, for primary ED.
The application of pancreas transplantation for the treatment of diabetes has increased as the success rate has improved. Several institutions have patient’s survival rates in excess of 90% [10-12]. Thus, pancreas transplantation has the potential to have the same impact on the treatment of diabetes as kidney transplantation has had on the treatment of end-stage-renal disease.
During the donor operation a careful retrograde dissection of the vessel allows the preservation of the integrity of the arterial distribution to the liver and the pancreas. The preservation of the IPA when replaced/ accessory right hepatic artery (RHA) is found is mandatory [13]. In the presence of a RHAarising from SMA it was initially recommended to abandon the pancreas procurement in order to preserve the hepatic vessel. The other crucial point of pancreas procurement is the dissection of the SA. Manipulation should be limited to its origin from TC in order to preserve an intact vessel for the revascularization of the pancreatic allograft.
Enteric drainage is physiologic and will preserve the architectural integrity of the graft, but, monitoring of exocrine function is difficult except in the immediately postoperative period if a catheter from the duct has been brought externally [14]. The advantage of urinary drainage technique is the ability to directly monitor exocrine function, which has been shown to decrease prior to hyperglycemia during rejection episodes [15].
Pancreas transplantation can effectively treat type I diabetes mellitus. For maximal therapeutic benefit, pancreas transplantation should be performed in very early stage of disease and surgeons must be aware of both multiple techniques and anatomical variations in order to maximize the short and long-term results.