Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 5
Objectives: Fatigue and unrefreshing sleep are symptoms of fibromyalgia and part of its diagnostic criteria. The literature is inconsistent regarding the prevalence of sleep disorders in fibromyalgia. The purpose of the study was to determine if obstructive sleep apnea (OSA) was more common in patients with fibromyalgia than in a general internal medicine clinic population.
Methods: The records of 500 patients seen in a fibromyalgia clinic who fulfilled diagnostic criteria for fibromyalgia were compared with 500 patients seen in a general internal medicine clinic who did not have the diagnosis of fibromyalgia. The presence of a diagnosis of OSA was abstracted from each record. Patients were matched for age, sex, and body mass index. Descriptive statistics were used to characterize the sample. Pearson χ2 test and Fisher exact test were used for analysis.
Results: OSA was significantly more common in patients presenting to a fibromyalgia clinic compared with the patient population lacking the fibromyalgia diagnosis. This finding was independent of body mass index in overweight and moderately obese cohorts.
Conclusion: Patients with fibromyalgia should be screened for OSA because treatment of sleep disorders may help with symptoms of fatigue and unrefreshing sleep.
Keywords: Fibromyalgia patients; Sleep apnea; Sleep disturbances; Sleep problems
AHI: Apnea Hypopnea Index; BMI: Body Mass Index; BSQ: Berlin Sleep Questionnaire; CI: Confidence Interval; OSA: Obstructive Sleep Apnea; PSG: Polysomnography; REM: Rapid Eye Movement
Obstructive sleep apnea (OSA) is the most common of all sleep-related breathing disorders. The estimated prevalence in North America is approximately 20% to 25% in males and 10% in females when OSA is defined as an apnea hypopnea index (AHI) greater than or equal to 5 events per hour, as determined by polysomnography (PSG) [1-3]. The strongest risk factor for OSA in both sexes is obesity, and prevalence of OSA increases with increasing body mass index (BMI) [3,4].
Sleep-related symptoms such as waking unrefreshed, fatigue, tiredness, and insomnia are common in patients with OSA; these are also common concerns for patients with fibromyalgia, a chronic condition characterized by widespread muscle pain and various symptoms such as cognitive difficulty, anxiety, and depression. Given the frequency with which sleep issues are reported, fatigue and waking tired or unrefreshed are included in the American College of Rheumatology diagnostic criteria for fibromyalgia [5]. PSG studies have been conducted in patients with fibromyalgia to delineate the physiologic basis of sleep-related symptoms, and distinctive patterns of alpha intrusion in non–rapid eye movement (REM) sleep have been described (phasic alpha, tonic alpha, and low alpha activity) [6-9].
The literature is inconsistent regarding the prevalence of sleep disorders in patients with fibromyalgia and the potential role of sleep disorders in fibromyalgia symptoms [7]. In a retrospective chart review of 23 women with fibromyalgia, Shah et al. [10] reported that a high percentage (83%) had an AHI greater than 15, indicating moderate sleep apnea. Their findings were also consistent with previous reports that suggested increased sleep latency and arousal index and reduced REM sleep in patients with fibromyalgia [11,12]. In another study of 28 women with fibromyalgia, 96% had sleep-disordered breathing [13]. The rates of sleep apnea reported in these studies, however, were significantly higher than that reported by Hamm et al. [14] who observed sleep apnea in 25% of patients with fibromyalgia, with 43% having alpha-delta intrusion. Similarly, Chen et al. [15] reported that 19% of females and 32% of males with fibromyalgia had documented sleep apnea. Although most published studies do not compare the prevalence of sleep apnea in patients with fibromyalgia vs individuals without chronic pain conditions, one controlled study showed no difference between patients and controls regarding the prevalence of sleep-disordered breathing [16]. However, patients with fibromyalgia did have greater sleep fragmentation than controls, which was consistent with the high rate of insomnia and un-refreshing sleep reported by patients with fibromyalgia [17].
Limited data describe the prevalence of fibromyalgia in patients with known sleep apnea. A study by Alvarez Lario et al. [18] reported no significant correlation between sleep apnea and the number of tender points in a sample of 30 patients with sleep apnea. In that study, only 1 patient had fibromyalgia. Another study reported that although OSA did not appear to be a significant problem in females with newly diagnosed fibromyalgia, fibromyalgia may be a marker of occult sleep apnea in males [19].
Research in animal models indicates that treatment of sleep disorders could have a positive impact on pain [20], and the same relationship potentially is present in patients with fibromyalgia. Strong evidence linking sleep apnea with fibromyalgia is lacking, but a case report describing a woman with a 10-year history of fibromyalgia suggests that treatment of sleep apnea could markedly reduce or eliminate symptoms of fibromyalgia for some patients [21].
The studies published to date have been conducted in relatively small groups of patients, and the reported associations between fibromyalgia and sleep apnea in men vs women differ substantially. Furthermore, although previous studies have confirmed the association between increased BMI and OSA, no reports describe a case-control study design in a large sample that allows evaluation of OSA prevalence in fibromyalgia, independent of BMI. The purpose of this study was to examine the frequency of OSA, the most common sleep-related breathing disorder, in patients presenting to a fibromyalgia clinic.
This study was approved by our institutional review board, and only patients who consented to use of their medical records for research were included in the study.
Setting
Patients included in this study were seen from December 2010 through October 2011 in the Fibromyalgia and Chronic Fatigue Clinic at a tertiary academic medical center in the United States.
Clinical design
We reviewed the charts of 500 consecutive patients who fulfilled the 2010 diagnostic criteria for fibromyalgia [5]. The following data were abstracted: age, sex, BMI, results of the Berlin Sleep Questionnaire (BSQ), results of an overnight oximetry test, results of a polysomnogram, and whether the patient had a previous or new diagnosis of OSA.
The BSQ was created during the 1996 Conference on Sleep in Primary Care held in Berlin, Germany, in which 120 US and German pulmonary and primary care physicians participated [22]. The questionnaire consists of 3 categories related to the risk of having OSA, including 1 introductory question and 4 follow-up questions concerning snoring, 3 questions addressing daytime sleepiness and 1 follow-up question about falling asleep while driving; and 1 question addressing the presence of hypertension. Patient BMI is also noted. Patients can be classified into high or low risk of OSA on the basis of their responses. Patients are considered high risk if 2 or more categories have positive scores (low risk is defined as only 1 or no categories with a positive score).
Overnight oximetry continuously records a patient’s oxygen level with a pulse oximeter during sleep. An abnormal test is not diagnostic of OSA, but it can be useful to screen for patterns of desaturation and changes in heart rate suggestive of OSA and can prompt further diagnostic testing. All overnight oximetry tests in our study were reviewed by interpreters in the Pulmonary Function Lab at our institution and classified as normal or abnormal.
For PSG tests, OSA was defined as an AHI greater than 5 events per hour, with more than half of the disordered breathing events considered to be obstructive.
Controls
We used a random algorithm to select 1 matched control for each case from a pool of 21,944 outpatients seen in the general internal medicine division of our clinic during the same period; controls were matched by sex, age, and BMI. Charts of the controls were reviewed for a diagnosis of OSA. Patients with the diagnosis of fibromyalgia were excluded from the control pool.
Statistical Analysis
Descriptive statistics (mean, median, SD, and percent) were used to describe the sample. The Pearson χ2 test and Fisher exact test were used for analysis and odds ratios and 95% confidence intervals (CI) were calculated for the overall sample and each BMI category.
Of the 500 patients with fibromyalgia, 441 (88.2%) were women. Median age was 48 years (range, 18-82 years), and median BMI was 29.6 kg/m2 (range, 15.6-64.3 kg/m2). At presentation, 104 fibromyalgia patients (20.8%) had the diagnosis of OSA (Figure 1). Of the 396 remaining patients, 340 (85.9%) completed the BSQ and 191 (56.2%) had high risk of OSA; 146 (36.9%) underwent oximetry, and 63 (43.2%) had abnormal results. Forty-seven patients (11.9%) underwent PSG, and 32 (68.1%) received the diagnosis of OSA. Seventy-eight of 500 patients (15.6%) were advised to undergo PSG because of a high-risk BSQ score or an abnormal overnight oximetry test but were unable to stay for the evaluation.
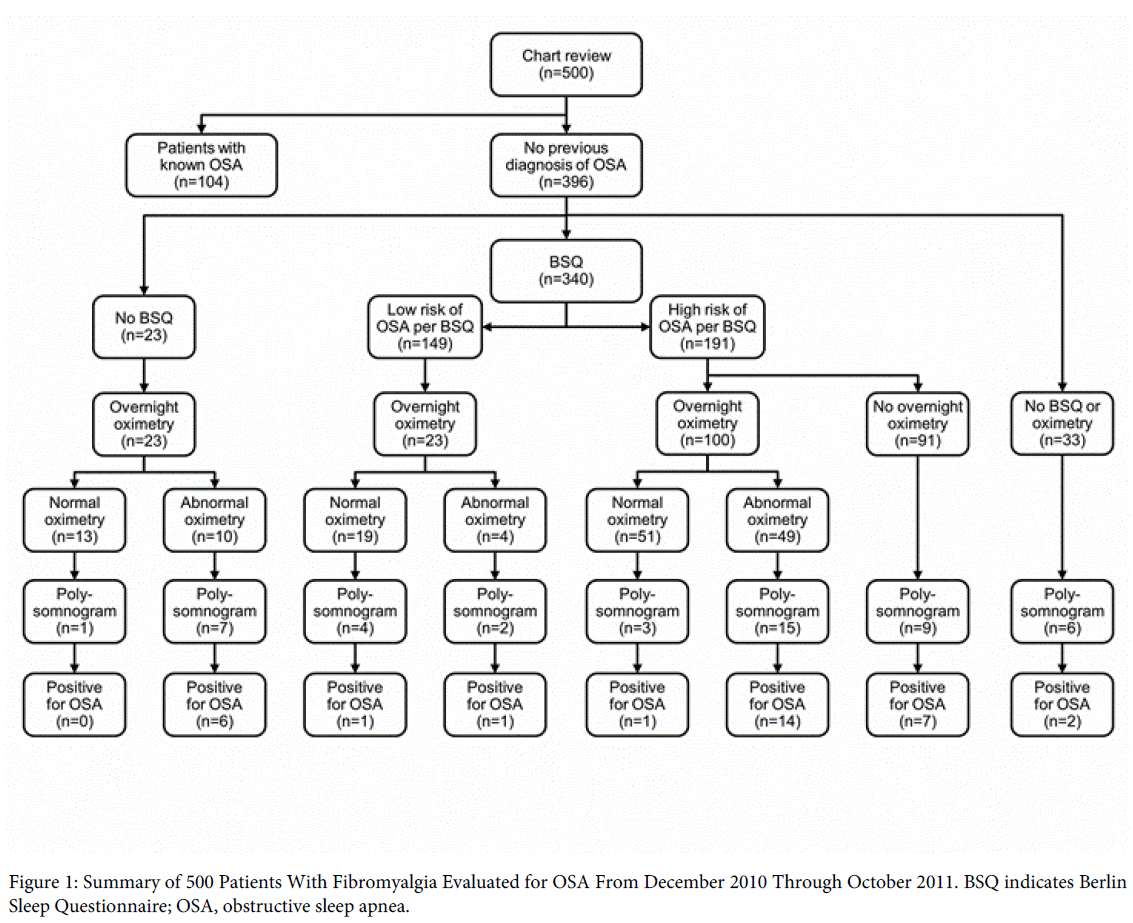
Figure 1: Summary of 500 Patients With Fibromyalgia Evaluated for OSA From December 2010 Through October 2011. BSQ indicates Berlin Sleep Questionnaire; OSA, obstructive sleep apnea.
The characteristics of the fibromyalgia and control cohorts (matched by sex, age, and BMI) are summarized in the Table 1. The Table further shows the percentage of OSA in the 2 groups, stratified by BMI category. In total, 104 (20.8%) in the fibromyalgia cohort had a previous diagnosis of OSA at initial presentation to fibromyalgia clinic, whereas 54 (10.8%) of the control group from the general internal medicine clinic had OSA, for an odds ratio of 2.17, 95% CI (1.52, 3.10). Among the 47 members of the fibromyalgia cohort who underwent PSG, 32 new cases were diagnosed. When including the 32 new cases of OSA in the fibromyalgia cohort, in total, 136 patients had a diagnosis of OSA, for a odds ratio of 3.09, 95% CI (2.19, 4.35). The higher rate of OSA in patients with fibromyalgia compared with controls was independent of increased BMI and this difference was statistically significant for two of the four BMI categories (25-29.9 kg/m2 and 35.0 kg/m2).
| Variable | Controls (n=500) | Patients With Fibromyalgia (n=500) | Odds Ratio | 95% CI | P Valuea | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Age, mean (SD), y | 47.27 (12.97) | 47.25 (12.98) | … | |||
| Female sex, No. (%) | 441 (88) | 441 (88) | … | |||
| BMI, mean (SD), kg/m2 | 30.33(8.35) | 30.29 (7.71) | … | |||
| BMI categories, No. (%) | ||||||
| <25.0 kg/m2 | 146 (29) | 146 (29) | … | |||
| 25.0-29.9 kg/m2 | 118 (24) | 118 (24) | … | |||
| 30.0-34.9 kg/m2 | 105 (21) | 105 (21) | … | |||
| >35.0 kg/m2 | 131 (26) | 131 (26) | … | |||
| OSA diagnosis, No. (%) | 54 (11) | 104 (21) | 2.17 | 1.52 | 3.1 | <0.001 |
| BMI, <25.0 kg/m2 | 3 (2) | 8 (5) | 2.69 | 0.71 | 10.21 | 0.22 |
| BMI, 25.0-29.9 kg/m2 | 5 (4) | 17 (14) | 3.48 | 1.28 | 9.52 | 0.012 |
| BMI, 30.0-34.9 kg/m2 | 16 (15) | 27 (26) | 1.73 | 0.92 | 3.25 | 0.09 |
| BMI, >35.0 kg/m2 | 30 (23) | 52 (40) | 1.82 | 1.14 | 2.9 | 0.005 |
Table 1: Characteristics of Fibromyalgia Cases and Controls and Prevalence of OSA (Stratified by BMI), aControls were matched for age, sex, and BMI.
Our study showed that the percentage of patients with OSA was significantly higher in patients presenting to a fibromyalgia clinic compared with a population of patients who did not have the diagnosis of fibromyalgia. Furthermore, additional cases of OSA were identified in a fibromyalgia population after screening with the BSQ and performing overnight oximetry studies.
This finding still holds true even when comparing cohorts matched by age, sex, and BMI. Medical conditions affecting prevalence of OSA, independent of BMI (or only weakly associated with BMI), include end-stage renal disease and postmenopausal status. The pathogenesis of OSA in patients with end-stage renal disease appears to be associated with factors such as pharyngeal narrowing associated with fluid overload [23]. Menopausal and postmenopausal women have an increased risk of OSA compared with premenopausal women, independent of age and BMI, with hormone replacement therapy appearing to reduce the risk [24,25]. We did not investigate the menopausal status or hormone replacement therapy use of any patients or controls enrolled in this study. However, because the 2 groups were matched for age and BMI, menopausal status and possible hormone replacement therapy use are unlikely causes of the observed differences in OSA.
Various substances and medications such as alcohol, benzodiazepines, and narcotics have been associated with OSA, and these factors may well exacerbate OSA in patients who are already at risk. Common medications used in patients with fibromyalgia that may affect sleep include anticonvulsants, psychostimulants, hypnotics, anti-parkinsonians, antidepressants, opiates, and anti-inflammatory agents [7]. We did not abstract patient medication usage, but we believe that the fibromyalgia patients were more likely to use medications such as opioids (which can potentially interfere with sleep) compared with the control group, thus contributing to the higher risk of OSA in the fibromyalgia cohort.
Some have evaluated the prevalence of sleep apnea in other rheumatologic conditions. Two abstracts described the risk of OSA in patients with rheumatoid arthritis. Holman et al. [26] reported a 45% prevalence of OSA in men with connective tissue diseases, including rheumatoid arthritis. The prevalence of OSA was high, regardless of BMI or the type of inflammatory disease. In a study from Japan, more than half of 96 patients with rheumatoid arthritis (mostly female) had OSA [27].
Strength of our study is the large number of patients in the fibromyalgia and control cohorts. In addition, the American College of Rheumatology’s uniform diagnostic criteria for fibromyalgia was used to identify the fibromyalgia patients. We suspect that more patients in our fibromyalgia population had OSA than was recognized because 78 patients (15.6%) were noted to have high risk of OSA on the basis of their BSQ or an abnormal overnight oximetry but were unable to undergo further testing with PSG. A weakness of this study was that we did not review any PSG findings from the patients who had OSA diagnosed at another institution. Furthermore, we lacked follow-up on patients with fibromyalgia who were advised to have a local sleep study performed, based on our risk assessment. OSA very likely was underdiagnosed in the control population as well because the processes of evaluating OSA in the fibromyalgia clinic are different from those used in the general internal medicine practice. All patients presenting to our fibromyalgia clinic are screened with a BSQ unless they decline. If abnormal, overnight oximetry and/or PSG are pursued. General internal medicine clinic patients are not usually subjected to this level of rigorous screening. Also, clinicians are more likely to evaluate a female patient with fibromyalgia without a history of snoring for sleep apnea than a female patient without fibromyalgia, but with complaints of insomnia and fatigue.. Given that an additional 32 patients with fibromyalgia were diagnosed with OSA during their evaluation, our odds ratio of 2.17, 95% CI (1.52, 3.10) based on 104 patients with fibromyalgia and OSA at the time of their presentation to fibromyalgia clinic likely underestimates the true prevalence of OSA in fibromyalgia patients. Furthermore, because not all patients underwent PSG, we were unable to include odds ratios for upper airway resistance between the two cohorts. Future research with consistent screening in patients and controls would help clarify these issues.
Our results show a higher percentage of OSA in patients with fibromyalgia compared with general internal medicine patients. Clinicians who care for patients with fibromyalgia should be mindful of this association and consider appropriate screening and diagnostic studies if indicated.