Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Editorial - (2016) Volume 6, Issue 1
Aim: To investigate the role of combination therapy using the cytokines antagonist, pentoxifylline in combination with a novel powerful antioxidant derived from grape product in the treatment of pancreatic disease.
Methods and Research Plan: We want to acknowledge that much of the groundwork has already been done demonstrating the positive effect of antioxidant therapy in pancreatic diseases including pancreatitis, chronic pancreatic disorders, fibrosis and even pancreatic cancer. It is also well accepted that pentoxifylline, originally described as a drug to aid blood circulation via actions on adenosine triphosphate, is also an effective and efficient inhibitor of platelet derived growth factor and other cytokines essential to the inflammatory and fibrotic processes. We have understood for several years that this immunopharmacological drug inhibits other key signalling molecules in the immune system, ultimately preventing the collagen synthesis and deposition which is critical in pancreatic, hepatic and intestinal fibrosis. Our aim is to combine these two forms of therapy in patients with chronic pancreatic disease while simultaneously optimizing conditions using as our basis the dramatic results that have already been reported widely in literature, by world class investigators.
Results and Conclusion: Results to date are promising. Our results presented here clearly indicate that pentoxifylline will block a process in a relatively rare form of intestinal fibrosis called collagenous colitis. This was our proof of concept. In this very selective disease the critical step is collagen deposition. Collagen synthesis resulting in deposition is the key factor involved and has a direct effect on the outcome in these patients with collagenous colitis. We were able to show that pentoxifylline would effectively reduce collagen deposition in the colons of a group of relatively heterogeneous patients with their one consistent variable being biopsy proven colonic collagen deposition and an elevated FSI or fibrogenic stimulation index. Our results also clearly indicate that the reduction in colonic collagen deposition occurring with pentoxifylline therapy is accompanied by a measurable DII or drug inhibition index and that the FSI was predictive of which cohort of patients would respond to this drug. Pentoxifylline was an effective anti-fibrotic agent while having little if any side effect and working in a very effective way to reduce the signs and symptoms of the disease. Long before we were able to see the histological proof in colonic biopsies, patients who prior to treatment showed a predictive DII were already reporting beneficial effects on their symptoms and clinicians were reporting improvement in clinical signs. At time points during the treatment period, biopsies revealed that the collagen was diminishing and results also indicate that the rate of reduction of collagen deposition related to the chronicity of the disease itself. The combination of a novel antioxidant derived from grapes together with the drug pentoxifylline has the potential to be effective in treating chronic pancreatic disease and may prevent and likely will slow the course of pancreatic fibrosis and the ensuing pancreatic cancer [1-10].
<Keywords: Chronic pancreatic disease, Collagenous colitis,Diagnostic tests for CPD and CC, Grape derived antioxidant,Pentoxifylline
Many disorders including pancreatitis, pancreatic fibrosis and pancreatic cancer are still some of the most difficult diseases and disorders to treat. The outcome remains grim for the vast majority of patients with chronic pancreatitis. There is a paucity of effective therapeutics. Perhaps it is time to rethink how we are developing new drugs to treat diseases and disorders that have been around for decades. Much research has been done and many research dollars have been spent and still we do not have effective therapeutics to treat some of the worst diseases, including pancreatic disorders.
Perhaps the time has come to go back to basics. Try to boost the body's immune system by taking advantage of what the host’s immune system already tries to do, but has so far been ineffective in doing, in response to some of our worst diseases. Then, and only then, we can attempt to add into the mix a drug that will effectively block a minor component of the pathway which is defective in that disease, disorder or form of inflammation. That combination therapy should be more effective and, as such, have a synergistic effect in its attack on the target defect in this disease. If done in this way, combination therapy would also cause less harm than some of the newer toxic agents that are being developed to target these diseases. Among the diseases most needing a new therapeutic approach, of course, are chronic pancreatitis, pancreatic fibrosis and pancreatic cancer.
It is well characterized that pancreatitis is an inflammatory disease which starts with destruction of pancreatic tissue and ultimately results in pancreatic insufficiency. We also know from many sources that an increase in oxidative stress plays a key role in both clinical and animal studies [1]. It is also now well documented that selected foods are an excellent source of antioxidants but, unfortunately, many of these foods are not well tolerated by patients with chronic pancreatitis. The chronicity of this disease results in inadequate absorption and or digestion.
Quite frankly, we've been doing it the old way for too long. I have been involved in medical research since the early 1980s at NIH, and there are still very few effective therapeutics that have been developed for some of the major diseases that were plaguing us in the 1980s. It was all well and good to focus on disease mechanism and thus try to find out exactly what is happening at the molecular level in a disease, but it is taking far too long and too many people are dying. In my opinion, the scientific method that we have used for the past 30 years, to try to understand the mechanism behind a disease, while giving us exquisite detail about the mechanism, only serves to underscore the fact that we do not understand the total mechanism, and as a result, too much time to develop relatively ineffective treatments for some of the worst diseases of mankind. It is time to take another look at how we develop drugs to treat disorders and perhaps accept that we can never totally understand the mechanism and clinical complexities of the disease. Instead, we should use some broad strokes to target what we shall call a fatal flaw in the disease mechanism, and pair that with a powerful antioxidant agent which will boost patients' ability to fight the disease [11-19].
It is likely that combination therapy has the potential to change the future of clinical therapeutics, especially since RCTs already show antioxidant benefit. In chronic pancreatitis, Vitamin C in combination with other antioxidants significantly reduced pain [12].
With over 35 years of studies in the field of inflammation and fibrosis in other organ systems (including the liver and the gastrointestinal system, fibrotic studies in lung and collagen deposition studies in cardiac tissue and brain), the wealth of information generated by those studies and subsequent publications should now be applied effectively to studying pancreatic disorders including pancreatitis, pancreatic fibrosis and ultimately pancreatic cancer [14-16].
Though anatomically different from the liver and gut, the pancreas is in such close proximity and under the same stressors and affected by the similar growth factor pattern and signalling molecules that ultimately, with some tweaking, it may be possible to develop a novel effective anti-inflammatory, anti-fibrotic drug for the pancreas. It doesn't take a great stretch of the imagination to extend the results we have researched in great depth in these other organ system and apply them to the pancreas (Figures 1 and 2).
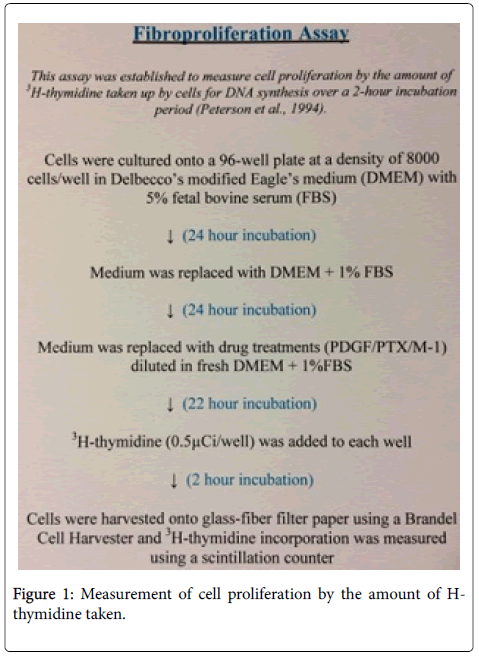
Figure 1: Measurement of cell proliferation by the amount of Hthymidine taken.
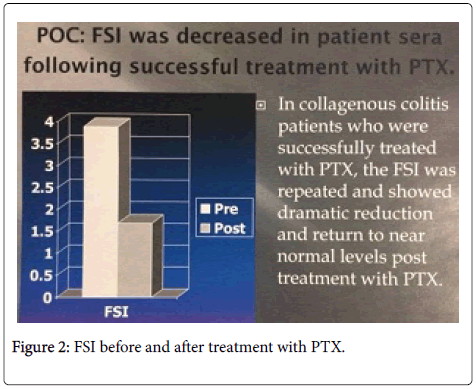
Figure 2: FSI before and after treatment with PTX.
A lot of the groundwork has already been laid by other investigators. It is simply a matter of taking that information in the context of the information already well published in other organ systems such as the liver and thus more rapidly develop new drugs to combat pancreatic disorders.
Our work in the gastrointestinal system specifically in collagenous colitis, (Figure 3) and our results obtained in liver disorders (including but not limited to hepatitis C and other hepatic fibrotic diseases) clearly indicate that platelet derived growth factor plays a key role [16]. While it is true that other major growth factors are involved, it appears that the fine-tuning of the fibrotic mechanism is under the influence of platelet derived growth factor.
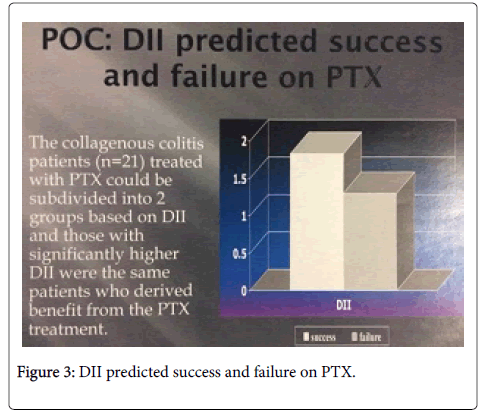
Figure 3: DII predicted success and failure on PTX.
Hence, if one can tweak the system by altering or inhibiting the action of platelet drive growth factor with a safe drug that has been used in other applications together with a nutraceutical such as an antioxidant derived from a natural food product, the combination of these two could effectively and safely, and with minimal side effects, alter the course of such diseases as pancreatitis and pancreatic fibrosis and perhaps prevent the ensuing pancreatic cancer.
With very limited side effects the patient would then have the opportunity to effectively fight off the continuing disease with their own immune system. We would simply be boosting the patient’s immune system with a powerful naturally sourced antioxidant which could together with a safe after-market drug (Figure 4) provide an effective cure. Unlike many of the newer toxic drugs that are being developed for fibrosis or cancer, this combination would work with the immune system of the patient while not destroying critical components of that defence system.
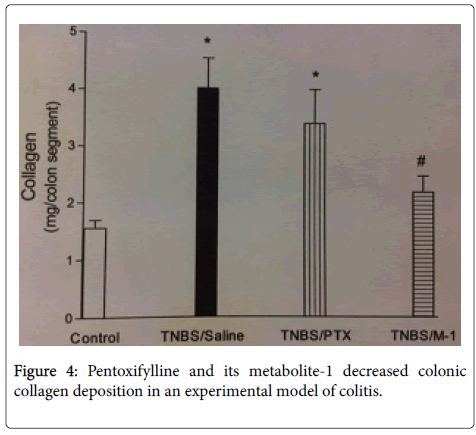
Figure 4: Pentoxifylline and its metabolite-1 decreased colonic collagen deposition in an experimental model of colitis.
We are currently doing proof of concept and pilot studies in this area. Our studies use a powdered extract loaded with antioxidants together with our patented antifibrotic/antifibrogenic/ antiinflammatory drug, pentoxifylline, (Figures 1-5) as a combination therapeutic which will in our opinion play a major role in the new regimen used to target diseases including, but not limited to, liver fibrosis and inflammation; diseases of the colon such as collagenous colitis (Figures 2, 3 and 5); and perhaps also ulcerative colitis and Crohn's; lung diseases including fibrosis; cardiac fibrosis; and even collagen storage diseases of the brain, including Alzheimer's. We feel it will effectively target pancreatitis and blockpancreatic fibrosis and the ensuing pancreatic cancer. Much work is left to be done but we feel that this novel combination is the new way to effectively target these diseases including pancreatic disorders.
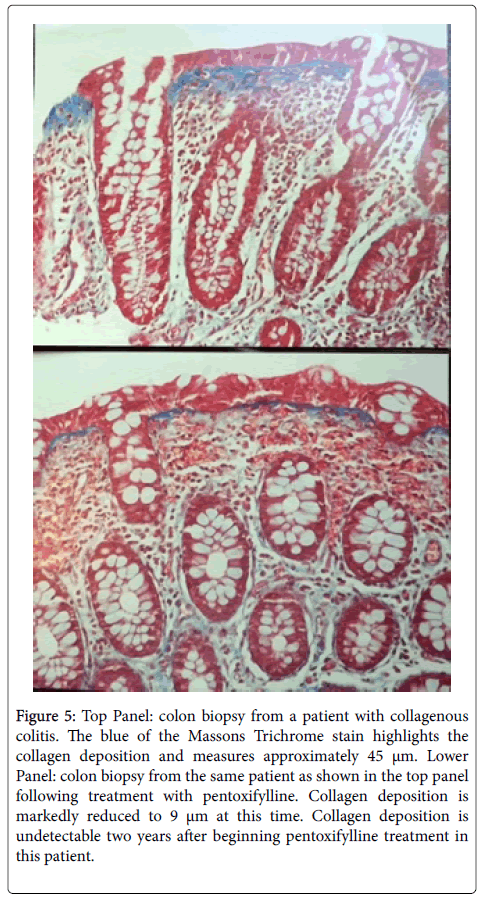
Figure 5: Top Panel: colon biopsy from a patient with collagenous colitis. The blue of the Massons Trichrome stain highlights the collagen deposition and measures approximately 45 μm. Lower Panel: colon biopsy from the same patient as shown in the top panel following treatment with pentoxifylline. Collagen deposition is markedly reduced to 9 μm at this time. Collagen deposition is undetectable two years after beginning pentoxifylline treatment in this patient.
This opens a new area of potential pharmaceutical/nutraceutical drugs which need not even be patented and need not be expensive. Such a combination therapy will be accessible by all chronic pancreatic disease patients that need the treatment. If these drugs can be developed and I think they can, these drugs do not have to cost patients and healthcare systems or drug plans, millions and millions of dollars, they could ultimately be over-the-counter medications.
The FSI is a good diagnostic test for many forms of fibrosis including hepatic, cardiac and intestinal fibrosis and collagen deposition in brain damage (Figure 1 and 2). There is a need for larger studies in these and other forms of fibrosis. The DII is a good diagnostic test to predict the beneficial effect of putative antifibrotic drugs (Figure 3), on an individualized patient basis; either alone or in combination with other drugs, e.g., anti-virals + PTX in HCV or antioxidants +PTX in CPD.
Collagenous colitis patient sera significantly increased ISMC proliferation.
FSI is an effective measure of fibrosis in collagenous colitis, and selected drugs inducing PTX significantly decreased that stimulated cell proliferation and c-Jun phosphorylation [14,15].
The DII may prove to be of significant utility in the development of novel therapeutics to treat IBD.
IL-18 is involved in IBD related ISMC proliferation [16].
Of recent interest are the very promising results that have been published by the Kalluri team in Nature 2015. Their results elegantly describe the use of exosomes for pancreatic cancer [17]. Perhaps another alternative includes pancreatic transplantation or development of an artificial pancreas in the future but in the interim one attractive therapeutic alternative requiring more clinical trial research is the combination therapy of pentoxifylline and antioxidants for chronic pancreatic disorders [18,19].
I would like to extend my special thanks and gratitude to our clinical collaborators Drs Tanton, Peltekian, Caldwell and scientists including Drs Robertson, Nebert, Dragunow, Gonzalez and Raoul. These studies were supported by CIHR, Innovacorp, and CIHR-Health Canada.
U.S. Patent Application Number 08/8700986
Uses for Pentoxifylline or functional derivatives/metabolites thereof: Patent No. 5985592
Date of Patent: November 16, 1999
U.S. Patent Application Serial Number 6025151
New uses for compounds which reduce c-jun gene expression
Date of Patent: Feburary 15, 2000
U.S. Patent Application Serial Number 6294350B1
Methods for treating fibroprliferative diseases
Date of Patent: September 25, 2001.